Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Cassiano Teixeira"
We found (45) results for your search.Abstract
Rev Bras Ter Intensiva. 2015;27(1):26-35
DOI 10.5935/0103-507X.20150006
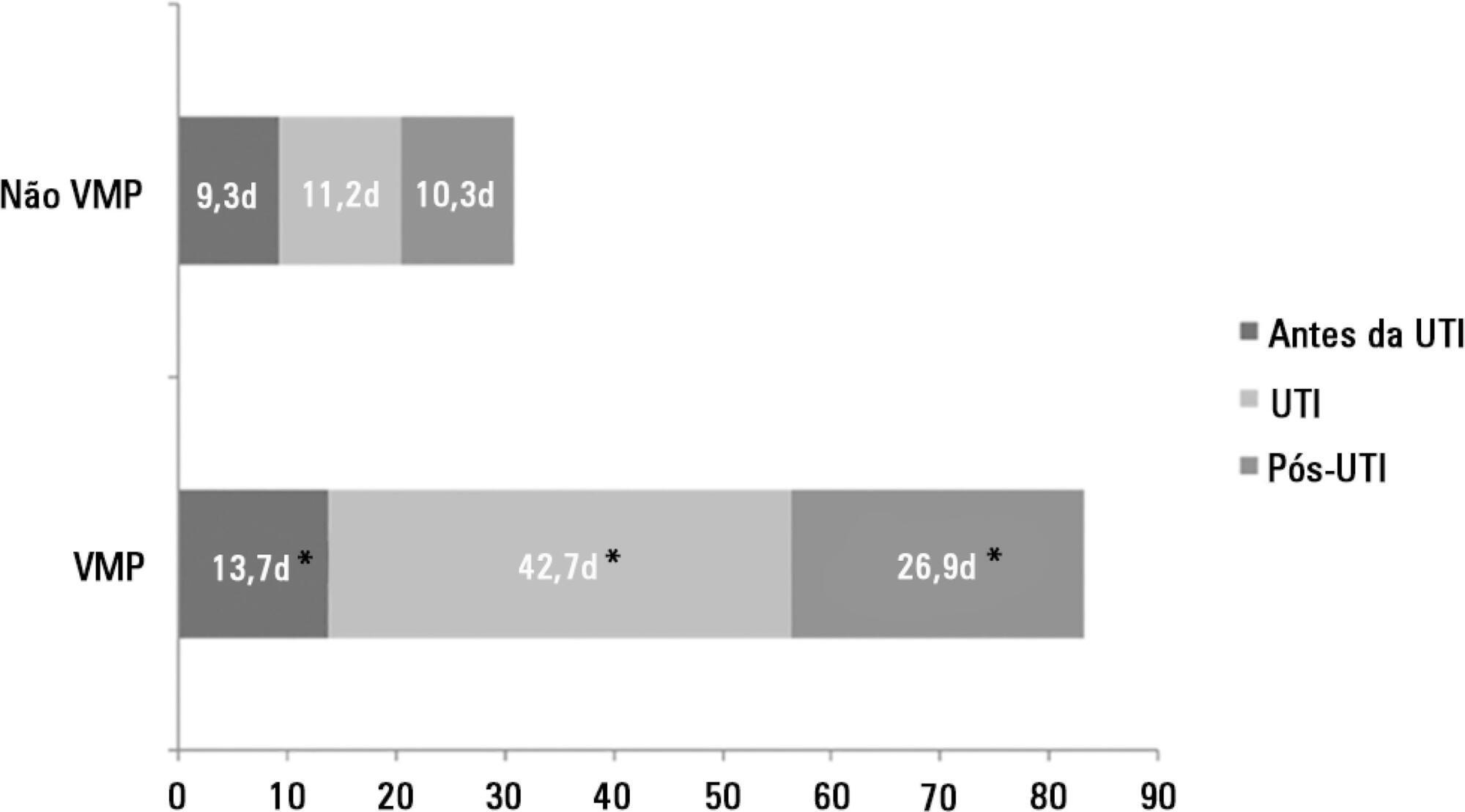
The number of patients who require prolonged mechanical ventilation increased during the last decade, which generated a large population of chronically ill patients. This study established the incidence of prolonged mechanical ventilation in four intensive care units and reported different characteristics, hospital outcomes, and the impact of costs and services of prolonged mechanical ventilation patients (mechanical ventilation dependency ≥ 21 days) compared with non-prolonged mechanical ventilation patients (mechanical ventilation dependency < 21 days).
This study was a multicenter cohort study of all patients who were admitted to four intensive care units. The main outcome measures were length of stay in the intensive care unit, hospital, complications during intensive care unit stay, and intensive care unit and hospital mortality.
There were 5,287 admissions to the intensive care units during study period. Some of these patients (41.5%) needed ventilatory support (n = 2,197), and 218 of the patients met criteria for prolonged mechanical ventilation (9.9%). Some complications developed during intensive care unit stay, such as muscle weakness, pressure ulcers, bacterial nosocomial sepsis, candidemia, pulmonary embolism, and hyperactive delirium, were associated with a significantly higher risk of prolonged mechanical ventilation. Prolonged mechanical ventilation patients had a significant increase in intensive care unit mortality (absolute difference = 14.2%, p < 0.001) and hospital mortality (absolute difference = 19.1%, p < 0.001). The prolonged mechanical ventilation group spent more days in the hospital after intensive care unit discharge (26.9 ± 29.3 versus 10.3 ± 20.4 days, p < 0.001) with higher costs.
The classification of chronically critically ill patients according to the definition of prolonged mechanical ventilation adopted by our study (mechanical ventilation dependency ≥ 21 days) identified patients with a high risk for complications during intensive care unit stay, longer intensive care unit and hospital stays, high death rates, and higher costs.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):26-35
DOI 10.5935/0103-507X.20150006
The number of patients who require prolonged mechanical ventilation increased during the last decade, which generated a large population of chronically ill patients. This study established the incidence of prolonged mechanical ventilation in four intensive care units and reported different characteristics, hospital outcomes, and the impact of costs and services of prolonged mechanical ventilation patients (mechanical ventilation dependency ≥ 21 days) compared with non-prolonged mechanical ventilation patients (mechanical ventilation dependency < 21 days).
This study was a multicenter cohort study of all patients who were admitted to four intensive care units. The main outcome measures were length of stay in the intensive care unit, hospital, complications during intensive care unit stay, and intensive care unit and hospital mortality.
There were 5,287 admissions to the intensive care units during study period. Some of these patients (41.5%) needed ventilatory support (n = 2,197), and 218 of the patients met criteria for prolonged mechanical ventilation (9.9%). Some complications developed during intensive care unit stay, such as muscle weakness, pressure ulcers, bacterial nosocomial sepsis, candidemia, pulmonary embolism, and hyperactive delirium, were associated with a significantly higher risk of prolonged mechanical ventilation. Prolonged mechanical ventilation patients had a significant increase in intensive care unit mortality (absolute difference = 14.2%, p < 0.001) and hospital mortality (absolute difference = 19.1%, p < 0.001). The prolonged mechanical ventilation group spent more days in the hospital after intensive care unit discharge (26.9 ± 29.3 versus 10.3 ± 20.4 days, p < 0.001) with higher costs.
The classification of chronically critically ill patients according to the definition of prolonged mechanical ventilation adopted by our study (mechanical ventilation dependency ≥ 21 days) identified patients with a high risk for complications during intensive care unit stay, longer intensive care unit and hospital stays, high death rates, and higher costs.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student's t-test and chi-squared analysis.
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student's t-test and chi-squared analysis.
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):269-270
DOI 10.5935/0103-507X.20190021
Abstract
Rev Bras Ter Intensiva. 2019;31(2):269-270
DOI 10.5935/0103-507X.20190021
Abstract
Rev Bras Ter Intensiva. 2011;23(3):269-282
DOI 10.1590/S0103-507X2011000300004
The role of intensive care specialists in the maintenance of deceased potential donors is not restricted to hemodynamics. Appropriate endocrine-metabolic management is fundamental to maintaining energy support and hydroelectrolytic control, which cooperate for hemodynamic stability. Hematological changes are also important, especially considering the issues caused by inappropriate transfusions. In addition, this article discusses the role of appropriate protective ventilation to prevent inflammatory responses and to provide more transplantable lungs. Finally, judicious assessment of infections and antibiotic therapy is discussed
Abstract
Rev Bras Ter Intensiva. 2011;23(3):269-282
DOI 10.1590/S0103-507X2011000300004
The role of intensive care specialists in the maintenance of deceased potential donors is not restricted to hemodynamics. Appropriate endocrine-metabolic management is fundamental to maintaining energy support and hydroelectrolytic control, which cooperate for hemodynamic stability. Hematological changes are also important, especially considering the issues caused by inappropriate transfusions. In addition, this article discusses the role of appropriate protective ventilation to prevent inflammatory responses and to provide more transplantable lungs. Finally, judicious assessment of infections and antibiotic therapy is discussed
Abstract
Rev Bras Ter Intensiva. 2017;29(3):279-286
DOI 10.5935/0103-507X.20170038
We aimed to investigate a potential association between B-lines and weaning failure.
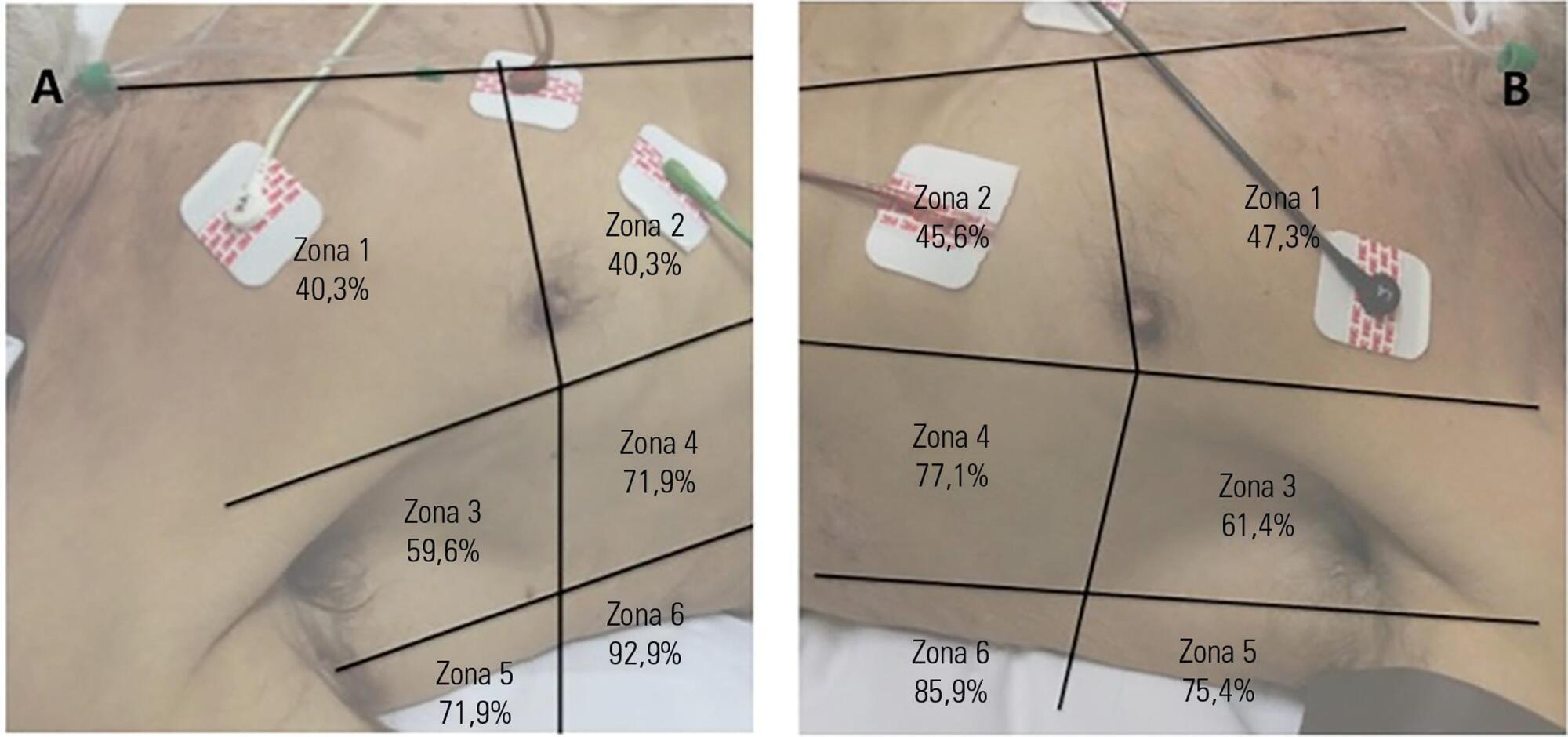
Fifty-seven subjects eligible for ventilation liberation were enrolled. Patients with tracheostomy were excluded. Lung ultrasound assessments of six thoracic zones were performed immediately before and at the exnd of the spontaneous breathing trial. B-predominance was defined as any profile with anterior bilateral B-pattern. Patients were followed up to 48 hours after extubation.
Thirty-eight individuals were successfully extubated; 11 failed the spontaneous breathing trial and 8 needed reintubation within 48 hours of extubation. At the beginning of the T-piece trial, B-pattern or consolidation was already found at the lower and posterior lung regions in more than half of the individuals and remained non-aerated at the end of the trial. A trend toward loss of lung aeration during spontaneous breathing trials was observed only in the spontaneous breathing trial-failure group (p = 0.07), and there was higher B-predominance at the end of the trial (p = 0.01).
A loss of lung aeration during the spontaneous breathing trial in non-dependent lung zones was demonstrated in subjects who failed to wean.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):279-286
DOI 10.5935/0103-507X.20170038
We aimed to investigate a potential association between B-lines and weaning failure.
Fifty-seven subjects eligible for ventilation liberation were enrolled. Patients with tracheostomy were excluded. Lung ultrasound assessments of six thoracic zones were performed immediately before and at the exnd of the spontaneous breathing trial. B-predominance was defined as any profile with anterior bilateral B-pattern. Patients were followed up to 48 hours after extubation.
Thirty-eight individuals were successfully extubated; 11 failed the spontaneous breathing trial and 8 needed reintubation within 48 hours of extubation. At the beginning of the T-piece trial, B-pattern or consolidation was already found at the lower and posterior lung regions in more than half of the individuals and remained non-aerated at the end of the trial. A trend toward loss of lung aeration during spontaneous breathing trials was observed only in the spontaneous breathing trial-failure group (p = 0.07), and there was higher B-predominance at the end of the trial (p = 0.01).
A loss of lung aeration during the spontaneous breathing trial in non-dependent lung zones was demonstrated in subjects who failed to wean.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):293-302
DOI 10.5935/0103-507X.20170055
To compare the functional capacity of younger elderly individuals (60 to 79 years old) with that of older elderly individuals (≥ 80 years old) during the first 6 months after discharge from the intensive care unit.
A multicenter prospective cohort study was conducted, in which data on intensive care unit admission and outcomes after hospital discharge (immediate post-discharge, after 3 months and after 6 months) were collected. Muscle strength was evaluated through the protocol of the Medical Research Council and dynamometry (handgrip); the ability to perform activities of daily life and functional independence were assessed by the Barthel index and the usual level of physical activity (International Physical Activity Questionnaire); and quality of life was assessed by the 12-Item Short-Form Health Survey Version 2.
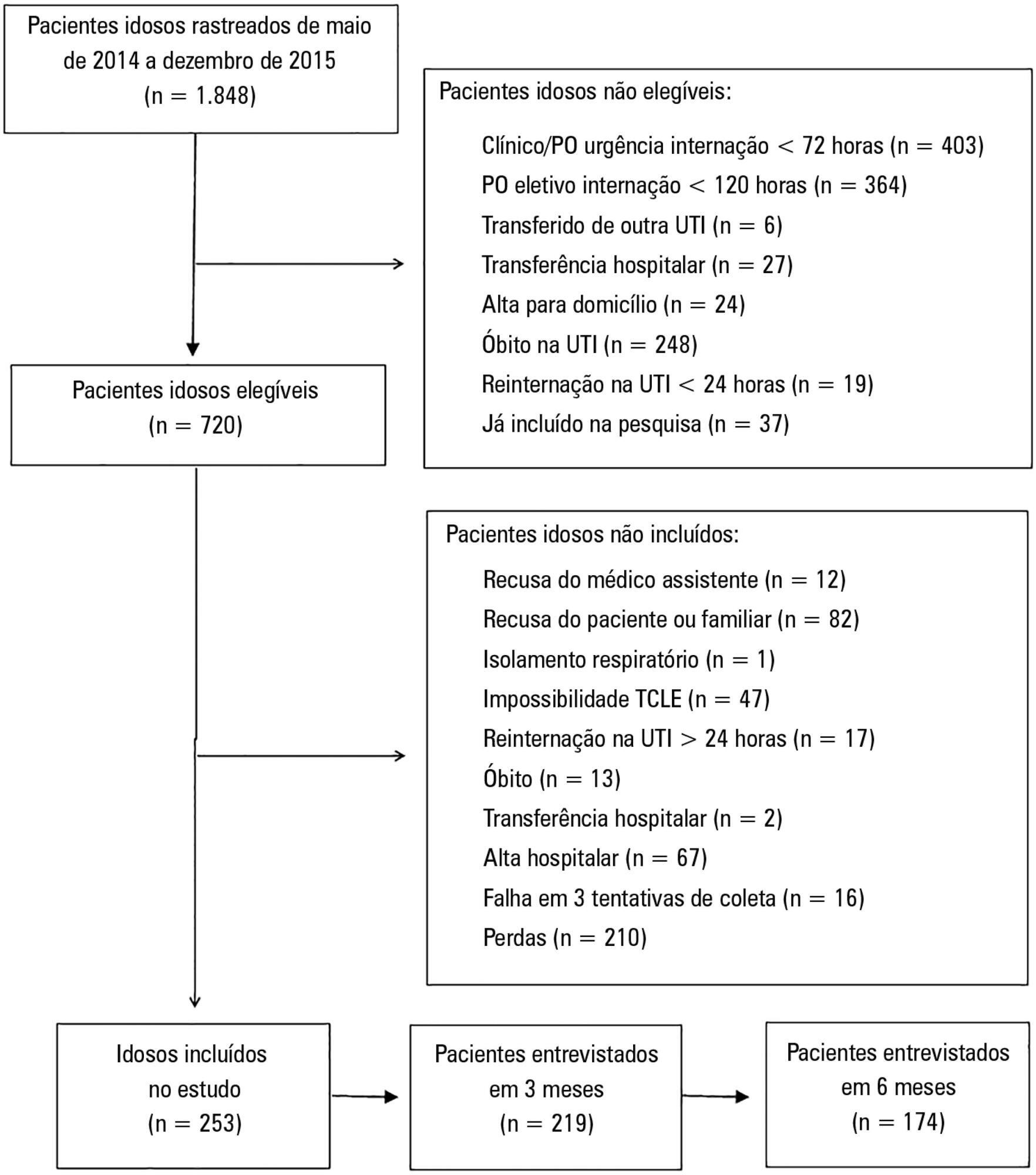
Among the 253 patients included, 167 were younger elderly (between 61 and 79 years old), and 86 were older elderly (≥ 80 years old). During the sixth month of evaluation, the older elderlies presented a higher need for a caregiver (69.0% versus 49, 5%, p = 0.002). Functional capacity prior to intensive care unit admission and in the third month after discharge was lower in older elderlies than in younger ones (Barthel prior to the intensive care unit: 73.0 ± 30.0 versus 86.5 ± 22.6; p <0.001, Barthel in the third month: 63.5 ± 34.0 versus 71.5 ± 35.5, p = 0.03), as was the usual level of physical activity (International Physical Activity Questionnaire in the third month: active/very active 3.4% versus 18.3%, no physical activity 64.4% versus 39.7%, p < 0.001, and International Physical Activity Questionnaire in the sixth month: active/very active 5.8% versus 20.8%, no physical activity 69.2% versus 43.4%, p = 0.005). Older elderlies had lower muscle strength when assessed according to handgrip in both the dominant (14.5 ± 7.7 versus 19.9 ± 9.6, p = 0.008) and non-dominant limb (13.1 ± 6.7 versus 17.5 ± 9.1, p = 0.02). There were no differences in functional capacity loss or reported quality of life between the age groups.
Although there were great functional capacity losses after discharge from the intensive care unit in both age groups, there was no difference in the magnitude of functional capacity loss between younger (60 to 79 years) and older elderly individuals (≥ 80 years old) during the first 6 months after discharge from the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):293-302
DOI 10.5935/0103-507X.20170055
To compare the functional capacity of younger elderly individuals (60 to 79 years old) with that of older elderly individuals (≥ 80 years old) during the first 6 months after discharge from the intensive care unit.
A multicenter prospective cohort study was conducted, in which data on intensive care unit admission and outcomes after hospital discharge (immediate post-discharge, after 3 months and after 6 months) were collected. Muscle strength was evaluated through the protocol of the Medical Research Council and dynamometry (handgrip); the ability to perform activities of daily life and functional independence were assessed by the Barthel index and the usual level of physical activity (International Physical Activity Questionnaire); and quality of life was assessed by the 12-Item Short-Form Health Survey Version 2.
Among the 253 patients included, 167 were younger elderly (between 61 and 79 years old), and 86 were older elderly (≥ 80 years old). During the sixth month of evaluation, the older elderlies presented a higher need for a caregiver (69.0% versus 49, 5%, p = 0.002). Functional capacity prior to intensive care unit admission and in the third month after discharge was lower in older elderlies than in younger ones (Barthel prior to the intensive care unit: 73.0 ± 30.0 versus 86.5 ± 22.6; p <0.001, Barthel in the third month: 63.5 ± 34.0 versus 71.5 ± 35.5, p = 0.03), as was the usual level of physical activity (International Physical Activity Questionnaire in the third month: active/very active 3.4% versus 18.3%, no physical activity 64.4% versus 39.7%, p < 0.001, and International Physical Activity Questionnaire in the sixth month: active/very active 5.8% versus 20.8%, no physical activity 69.2% versus 43.4%, p = 0.005). Older elderlies had lower muscle strength when assessed according to handgrip in both the dominant (14.5 ± 7.7 versus 19.9 ± 9.6, p = 0.008) and non-dominant limb (13.1 ± 6.7 versus 17.5 ± 9.1, p = 0.02). There were no differences in functional capacity loss or reported quality of life between the age groups.
Although there were great functional capacity losses after discharge from the intensive care unit in both age groups, there was no difference in the magnitude of functional capacity loss between younger (60 to 79 years) and older elderly individuals (≥ 80 years old) during the first 6 months after discharge from the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):300-302
DOI 10.5935/0103-507X.20220029-en
Abstract
Rev Bras Ter Intensiva. 2022;34(2):300-302
DOI 10.5935/0103-507X.20220029-en
Abstract
Rev Bras Ter Intensiva. 2020;32(2):308-311
DOI 10.5935/0103-507X.20200033
The disease pandemic caused by the novel coronavirus has triggered significant changes in the medical decision-making process relating to critically ill patients. Admissions to intensive care units have suddenly increased, but many of these patients do not present with clinical manifestations related to the viral infection but rather exacerbation of preexisting diseases. In this context, we must prevent intuitive decision-making and insecurity from leading us to exhaust the available critical-care beds before they are truly necessary, while still recognizing the importance of rapid decision-making in emergency situations. One of the best ways to achieve this goal may be by practicing metacognition and establishing ways for regular feedback to be provided to professionals engaged in inherently rapid decision-making processes.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):308-311
DOI 10.5935/0103-507X.20200033
The disease pandemic caused by the novel coronavirus has triggered significant changes in the medical decision-making process relating to critically ill patients. Admissions to intensive care units have suddenly increased, but many of these patients do not present with clinical manifestations related to the viral infection but rather exacerbation of preexisting diseases. In this context, we must prevent intuitive decision-making and insecurity from leading us to exhaust the available critical-care beds before they are truly necessary, while still recognizing the importance of rapid decision-making in emergency situations. One of the best ways to achieve this goal may be by practicing metacognition and establishing ways for regular feedback to be provided to professionals engaged in inherently rapid decision-making processes.