Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Pedro Povoa"
We found (19) results for your search.Abstract
Crit Care Sci. 2023;35(4):394-401
DOI 10.5935/2965-2774.20230170-pt
To investigate the impact of delirium severity in critically ill COVID-19 patients and its association with outcomes.
This prospective cohort study was performed in two tertiary intensive care units in Rio de Janeiro, Brazil. COVID-19 patients were evaluated daily during the first 7 days of intensive care unit stay using the Richmond Agitation Sedation Scale, Confusion Assessment Method for Intensive Care Unit (CAM-ICU) and Confusion Method Assessment for Intensive Care Unit-7 (CAM-ICU-7). Delirium severity was correlated with outcomes and one-year mortality.
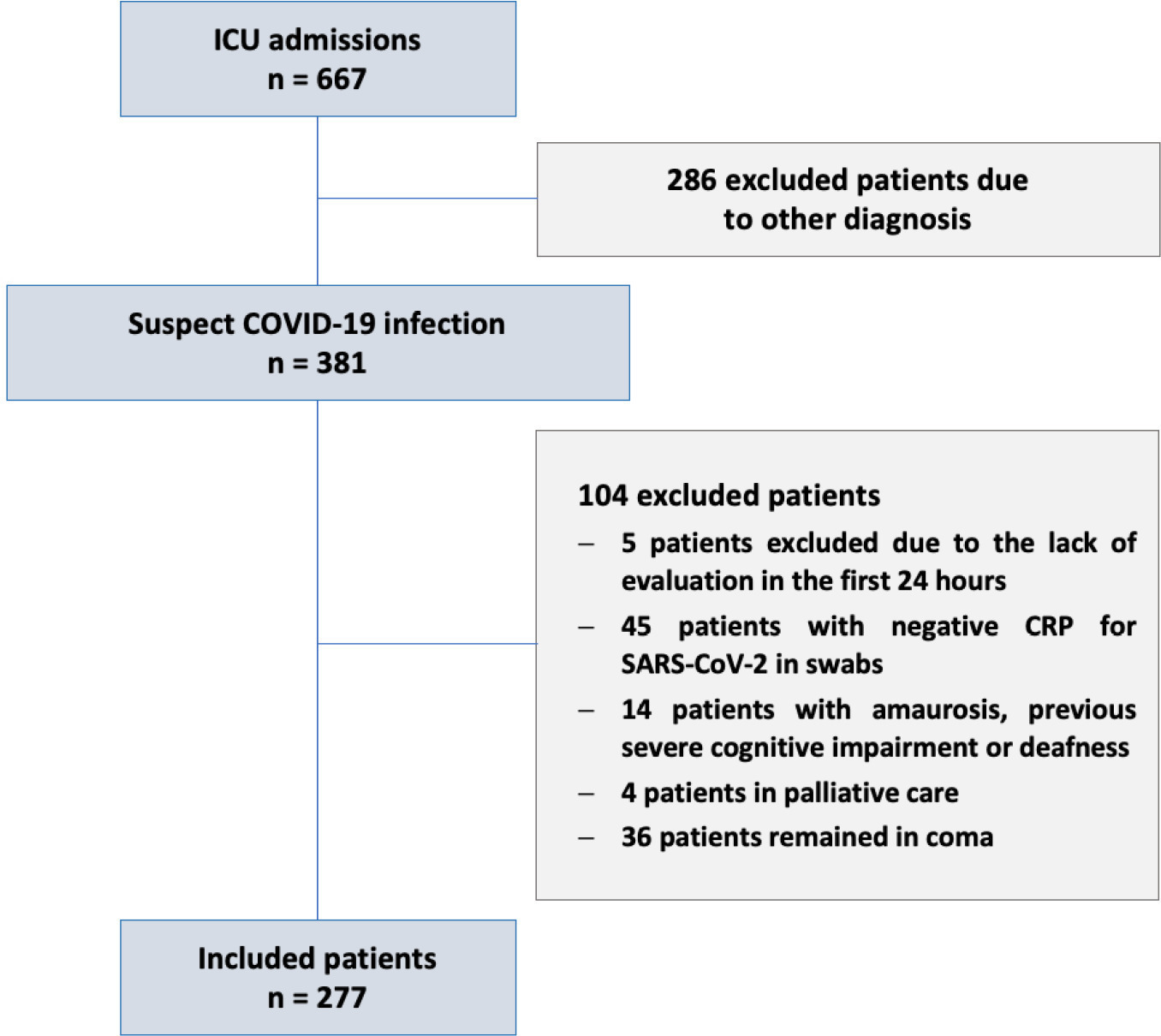
Among the 277 COVID-19 patients included, delirium occurred in 101 (36.5%) during the first 7 days of intensive care unit stay, and it was associated with a higher length of intensive care unit stay in days (IQR 13 [7 - 25] versus 6 [4 - 12]; p < 0.001), higher hospital mortality (25.74% versus 5.11%; p < 0.001) and additional higher one-year mortality (5.3% versus 0.6%, p < 0.001). Delirium was classified by CAM-ICU-7 in terms of severity, and higher scores were associated with higher in-hospital mortality (17.86% versus 34.38% versus 38.46%, 95%CI, p value < 0.001). Severe delirium was associated with a higher risk of progression to coma (OR 7.1; 95%CI 1.9 - 31.0; p = 0.005) and to mechanical ventilation (OR 11.09; 95%CI 2.8 - 58.5; p = 0.002) in the multivariate analysis, adjusted by severity and frailty.
In patients admitted with COVID-19 in the intensive care unit, delirium was an independent risk factor for the worst prognosis, including mortality. The delirium severity assessed by the CAM-ICU-7 during the first week in the intensive care unit was associated with poor outcomes, including progression to coma and to mechanical ventilation.
Abstract
Crit Care Sci. 2023;35(4):394-401
DOI 10.5935/2965-2774.20230170-pt
To investigate the impact of delirium severity in critically ill COVID-19 patients and its association with outcomes.
This prospective cohort study was performed in two tertiary intensive care units in Rio de Janeiro, Brazil. COVID-19 patients were evaluated daily during the first 7 days of intensive care unit stay using the Richmond Agitation Sedation Scale, Confusion Assessment Method for Intensive Care Unit (CAM-ICU) and Confusion Method Assessment for Intensive Care Unit-7 (CAM-ICU-7). Delirium severity was correlated with outcomes and one-year mortality.
Among the 277 COVID-19 patients included, delirium occurred in 101 (36.5%) during the first 7 days of intensive care unit stay, and it was associated with a higher length of intensive care unit stay in days (IQR 13 [7 - 25] versus 6 [4 - 12]; p < 0.001), higher hospital mortality (25.74% versus 5.11%; p < 0.001) and additional higher one-year mortality (5.3% versus 0.6%, p < 0.001). Delirium was classified by CAM-ICU-7 in terms of severity, and higher scores were associated with higher in-hospital mortality (17.86% versus 34.38% versus 38.46%, 95%CI, p value < 0.001). Severe delirium was associated with a higher risk of progression to coma (OR 7.1; 95%CI 1.9 - 31.0; p = 0.005) and to mechanical ventilation (OR 11.09; 95%CI 2.8 - 58.5; p = 0.002) in the multivariate analysis, adjusted by severity and frailty.
In patients admitted with COVID-19 in the intensive care unit, delirium was an independent risk factor for the worst prognosis, including mortality. The delirium severity assessed by the CAM-ICU-7 during the first week in the intensive care unit was associated with poor outcomes, including progression to coma and to mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):4-8
DOI 10.5935/0103-507X.20170002
Abstract
Rev Bras Ter Intensiva. 2017;29(1):4-8
DOI 10.5935/0103-507X.20170002
Abstract
Rev Bras Ter Intensiva. 2022;34(4):433-442
DOI 10.5935/0103-507X.20210037-en
To analyze and compare COVID-19 patient characteristics, clinical management and outcomes between the peak and plateau periods of the first pandemic wave in Portugal.
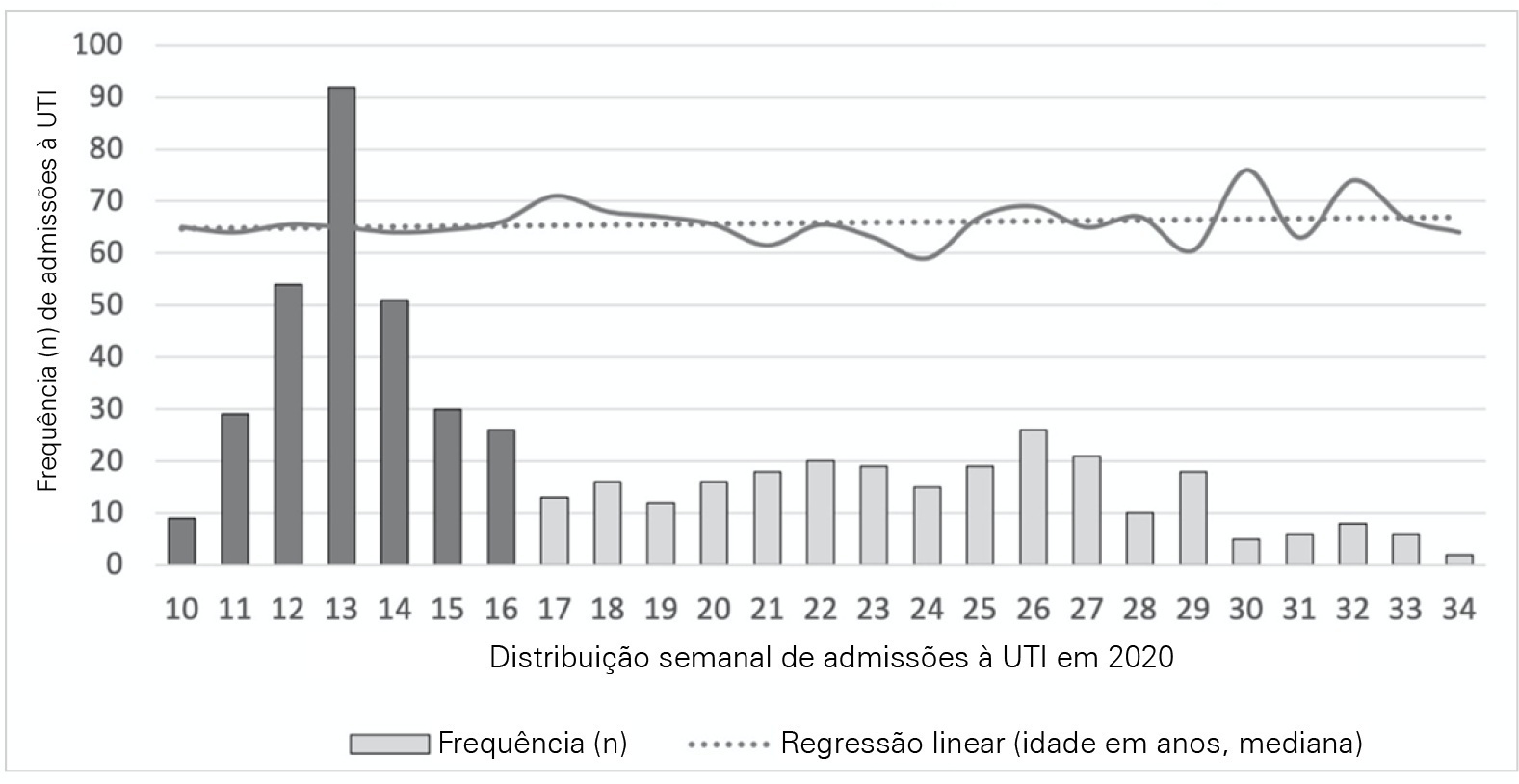
This was a multicentric ambispective cohort study including consecutive severe COVID-19 patients between March and August 2020 from 16 Portuguese intensive care units. The peak and plateau periods, respectively, weeks 10 - 16 and 17 - 34, were defined.
Five hundred forty-one adult patients with a median age of 65 [57 - 74] years, mostly male (71.2%), were included. There were no significant differences in median age (p = 0.3), Simplified Acute Physiology Score II (40 versus 39; p = 0.8), partial arterial oxygen pressure/fraction of inspired oxygen ratio (139 versus 136; p = 0.6), antibiotic therapy (57% versus 64%; p = 0.2) at admission, or 28-day mortality (24.4% versus 22.8%; p = 0.7) between the peak and plateau periods. During the peak period, patients had fewer comorbidities (1 [0 - 3] versus 2 [0 - 5]; p = 0.002) and presented a higher use of vasopressors (47% versus 36%; p < 0.001) and invasive mechanical ventilation (58.1 versus 49.2%; p < 0.001) at admission, prone positioning (45% versus 36%; p = 0.04), and hydroxychloroquine (59% versus 10%; p < 0.001) and lopinavir/ritonavir (41% versus 10%; p < 0.001) prescriptions. However, a greater use of high-flow nasal cannulas (5% versus 16%, p < 0.001) on admission, remdesivir (0.3% versus 15%; p < 0.001) and corticosteroid (29% versus 52%, p < 0.001) therapy, and a shorter ICU length of stay (12 days versus 8, p < 0.001) were observed during the plateau.
There were significant changes in patient comorbidities, intensive care unit therapies and length of stay between the peak and plateau periods of the first COVID-19 wave.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):433-442
DOI 10.5935/0103-507X.20210037-en
To analyze and compare COVID-19 patient characteristics, clinical management and outcomes between the peak and plateau periods of the first pandemic wave in Portugal.
This was a multicentric ambispective cohort study including consecutive severe COVID-19 patients between March and August 2020 from 16 Portuguese intensive care units. The peak and plateau periods, respectively, weeks 10 - 16 and 17 - 34, were defined.
Five hundred forty-one adult patients with a median age of 65 [57 - 74] years, mostly male (71.2%), were included. There were no significant differences in median age (p = 0.3), Simplified Acute Physiology Score II (40 versus 39; p = 0.8), partial arterial oxygen pressure/fraction of inspired oxygen ratio (139 versus 136; p = 0.6), antibiotic therapy (57% versus 64%; p = 0.2) at admission, or 28-day mortality (24.4% versus 22.8%; p = 0.7) between the peak and plateau periods. During the peak period, patients had fewer comorbidities (1 [0 - 3] versus 2 [0 - 5]; p = 0.002) and presented a higher use of vasopressors (47% versus 36%; p < 0.001) and invasive mechanical ventilation (58.1 versus 49.2%; p < 0.001) at admission, prone positioning (45% versus 36%; p = 0.04), and hydroxychloroquine (59% versus 10%; p < 0.001) and lopinavir/ritonavir (41% versus 10%; p < 0.001) prescriptions. However, a greater use of high-flow nasal cannulas (5% versus 16%, p < 0.001) on admission, remdesivir (0.3% versus 15%; p < 0.001) and corticosteroid (29% versus 52%, p < 0.001) therapy, and a shorter ICU length of stay (12 days versus 8, p < 0.001) were observed during the plateau.
There were significant changes in patient comorbidities, intensive care unit therapies and length of stay between the peak and plateau periods of the first COVID-19 wave.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):453-459
DOI 10.5935/0103-507X.20180062
To determine the performance of soluble urokinase-type plasminogen activator receptor upon intensive care unit discharge to predict post intensive care unit mortality.
A prospective observational cohort study was conducted during a 24-month period in an 8-bed polyvalent intensive care unit. APACHE II, SOFA, C-reactive protein, white cell count and soluble urokinase-type plasminogen activator receptor on the day of intensive care unit discharge were collected from patients who survived intensive care unit admission.
Two hundred and two patients were included in this study, 29 patients (18.6%) of whom died after intensive care unit discharge. Nonsurvivors were older and more seriously ill upon intensive care unit admission with higher severity scores, and nonsurvivors required extended use of vasopressors than did survivors. The area under the receiver operating characteristics curves of SOFA, APACHE II, C-reactive protein, white cell count, and soluble urokinase-type plasminogen activator receptor at intensive care unit discharge as prognostic markers of hospital death were 0.78 (95%CI 0.70 - 0.86); 0.70 (95%CI 0.61 - 0.79); 0.54 (95%CI 0.42 - 0.65); 0.48 (95%CI 0.36 - 0.58); and 0.68 (95%CI 0.58 - 0.78), respectively. SOFA was independently associated with a higher risk of in-hospital mortality (OR 1.673; 95%CI 1.252 - 2.234), 28-day mortality (OR 1.861; 95%CI 1.856 - 2.555) and 90-day mortality (OR 1.584; 95%CI 1.241 - 2.022).
At intensive care unit discharge, soluble urokinase-type plasminogen activator receptor is a poor predictor of post intensive care unit prognosis.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):453-459
DOI 10.5935/0103-507X.20180062
To determine the performance of soluble urokinase-type plasminogen activator receptor upon intensive care unit discharge to predict post intensive care unit mortality.
A prospective observational cohort study was conducted during a 24-month period in an 8-bed polyvalent intensive care unit. APACHE II, SOFA, C-reactive protein, white cell count and soluble urokinase-type plasminogen activator receptor on the day of intensive care unit discharge were collected from patients who survived intensive care unit admission.
Two hundred and two patients were included in this study, 29 patients (18.6%) of whom died after intensive care unit discharge. Nonsurvivors were older and more seriously ill upon intensive care unit admission with higher severity scores, and nonsurvivors required extended use of vasopressors than did survivors. The area under the receiver operating characteristics curves of SOFA, APACHE II, C-reactive protein, white cell count, and soluble urokinase-type plasminogen activator receptor at intensive care unit discharge as prognostic markers of hospital death were 0.78 (95%CI 0.70 - 0.86); 0.70 (95%CI 0.61 - 0.79); 0.54 (95%CI 0.42 - 0.65); 0.48 (95%CI 0.36 - 0.58); and 0.68 (95%CI 0.58 - 0.78), respectively. SOFA was independently associated with a higher risk of in-hospital mortality (OR 1.673; 95%CI 1.252 - 2.234), 28-day mortality (OR 1.861; 95%CI 1.856 - 2.555) and 90-day mortality (OR 1.584; 95%CI 1.241 - 2.022).
At intensive care unit discharge, soluble urokinase-type plasminogen activator receptor is a poor predictor of post intensive care unit prognosis.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):455-461
DOI 10.1590/S0103-507X2011000400010
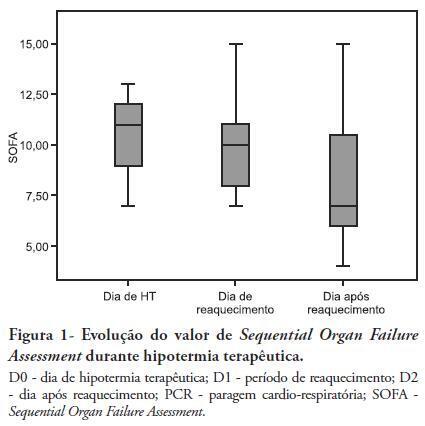
OBJECTIVES: Therapeutic hypothermia following cardiorespiratory arrest has been demonstrated to have cardio- and neuroprotective effects, resulting in improved survival and better neurological outcomes. The objective of this study was to assess the outcomes of patients undergoing therapeutic hypothermia following cardiorespiratory arrest. METHODS: A prospective, 10-month observational study of patients admitted to an intensive care unit and undergoing therapeutic hypothermia after cardiorespiratory arrest was undertaken. Therapeutic hypothermia was induced by cold fluid administration and body surface cooling in patients admitted no more than 12 hours after resuscitation from cardiorespiratory arrest. A target temperature of 33ºC was maintained for 24 hours. RESULTS: Overall, 12 patients were included (median age 64 years, 58% male). Half of the cardiorespiratory arrests were in-hospital. The median first-day Charlson Index, Sequential Organ Failure Assessment (SOFA) and Acute Physiology and Chronic Health Evaluation II scores were of 2.9, 11 and 24.5, respectively. The intensive care unit mortality rate was 42% (N=5). Five of the 7 surviving patients recovered their pre-cardiorespiratory arrest neurological status. Hypothermia was initiated 120 min (median) after recovery of spontaneous circulation. Most patients (75%) required vasopressor support. During the first 3 days after cardiorespiratory arrest and therapeutic hypothermia, a progressive SOFA score decrease (median 11 on day 0, 10 on day 1 and 7 on day 2) was observed. DISCUSSION: In this study, therapeutic hypothermia was applied to all post-cardiorespiratory arrest patients and demonstrated good neurological outcome in surviving patients.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):455-461
DOI 10.1590/S0103-507X2011000400010
OBJECTIVES: Therapeutic hypothermia following cardiorespiratory arrest has been demonstrated to have cardio- and neuroprotective effects, resulting in improved survival and better neurological outcomes. The objective of this study was to assess the outcomes of patients undergoing therapeutic hypothermia following cardiorespiratory arrest. METHODS: A prospective, 10-month observational study of patients admitted to an intensive care unit and undergoing therapeutic hypothermia after cardiorespiratory arrest was undertaken. Therapeutic hypothermia was induced by cold fluid administration and body surface cooling in patients admitted no more than 12 hours after resuscitation from cardiorespiratory arrest. A target temperature of 33ºC was maintained for 24 hours. RESULTS: Overall, 12 patients were included (median age 64 years, 58% male). Half of the cardiorespiratory arrests were in-hospital. The median first-day Charlson Index, Sequential Organ Failure Assessment (SOFA) and Acute Physiology and Chronic Health Evaluation II scores were of 2.9, 11 and 24.5, respectively. The intensive care unit mortality rate was 42% (N=5). Five of the 7 surviving patients recovered their pre-cardiorespiratory arrest neurological status. Hypothermia was initiated 120 min (median) after recovery of spontaneous circulation. Most patients (75%) required vasopressor support. During the first 3 days after cardiorespiratory arrest and therapeutic hypothermia, a progressive SOFA score decrease (median 11 on day 0, 10 on day 1 and 7 on day 2) was observed. DISCUSSION: In this study, therapeutic hypothermia was applied to all post-cardiorespiratory arrest patients and demonstrated good neurological outcome in surviving patients.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):472-482
DOI 10.5935/0103-507X.20160080
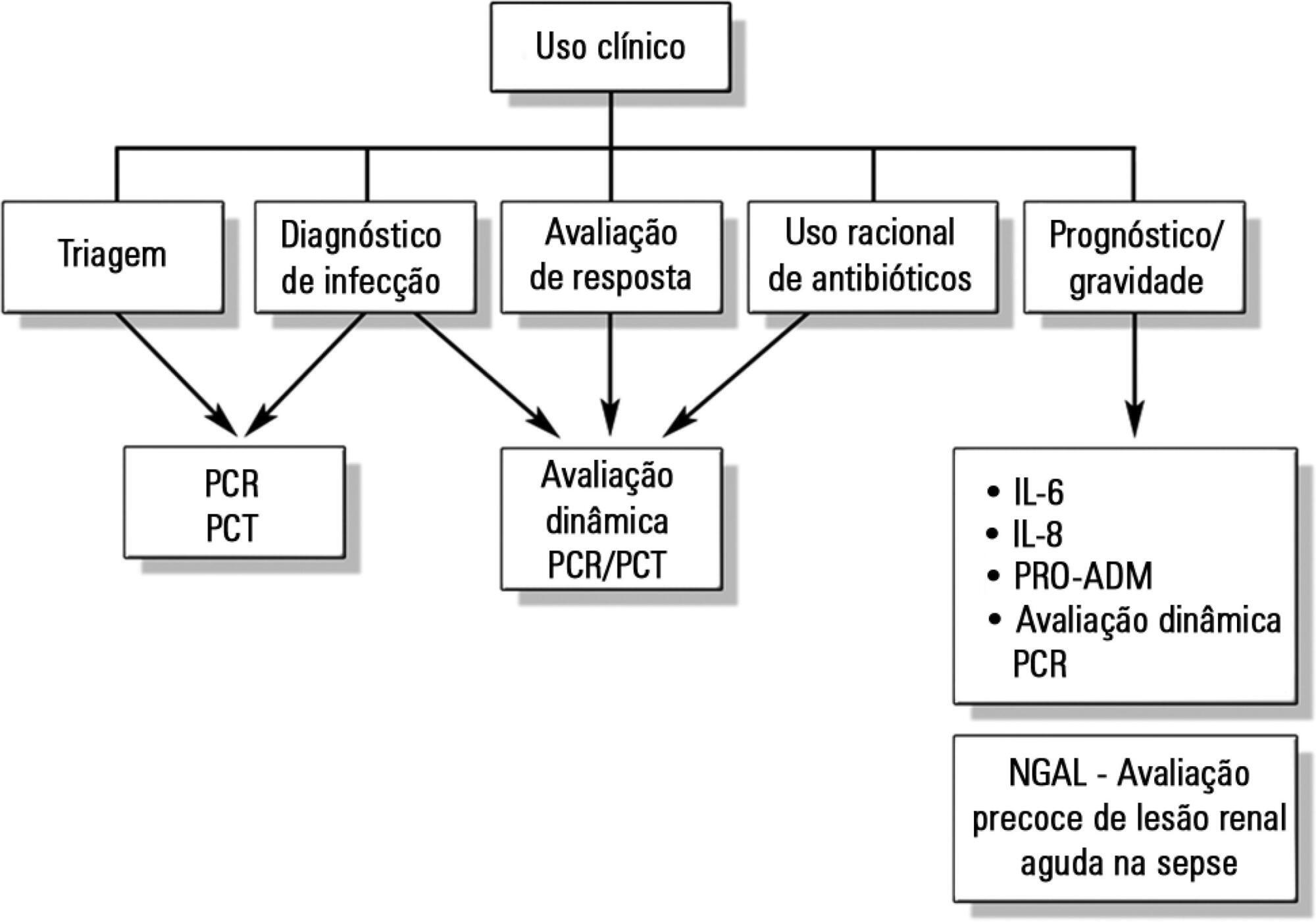
Despite advances in recent years, sepsis is still a leading cause of hospitalization and mortality in infants and children. The presence of biomarkers during the response to an infectious insult makes it possible to use such biomarkers in screening, diagnosis, prognosis (risk stratification), monitoring of therapeutic response, and rational use of antibiotics (for example, the determination of adequate treatment length). Studies of biomarkers in sepsis in children are still relatively scarce. This review addresses the use of biomarkers in sepsis in pediatric patients with emphasis on C-reactive protein, procalcitonin, interleukins 6, 8, and 18, human neutrophil gelatinase, and proadrenomedullin. Assessment of these biomarkers may be useful in the management of pediatric sepsis.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):472-482
DOI 10.5935/0103-507X.20160080
Despite advances in recent years, sepsis is still a leading cause of hospitalization and mortality in infants and children. The presence of biomarkers during the response to an infectious insult makes it possible to use such biomarkers in screening, diagnosis, prognosis (risk stratification), monitoring of therapeutic response, and rational use of antibiotics (for example, the determination of adequate treatment length). Studies of biomarkers in sepsis in children are still relatively scarce. This review addresses the use of biomarkers in sepsis in pediatric patients with emphasis on C-reactive protein, procalcitonin, interleukins 6, 8, and 18, human neutrophil gelatinase, and proadrenomedullin. Assessment of these biomarkers may be useful in the management of pediatric sepsis.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):481-489
DOI 10.5935/0103-507X.20170072
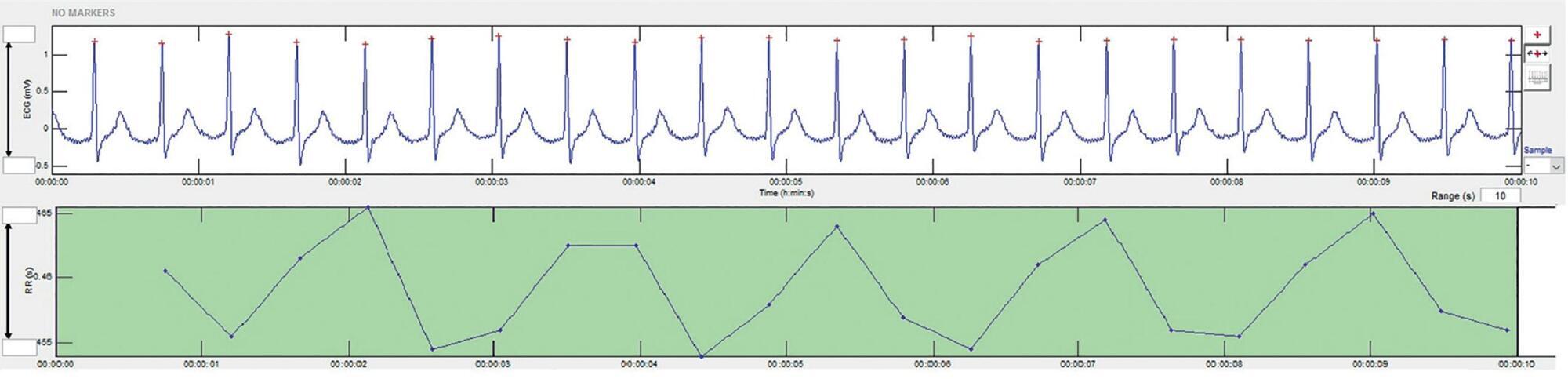
To present a systematic review of the use of autonomic nervous system monitoring as a prognostic tool in intensive care units by assessing heart rate variability.
Literature review of studies published until July 2016 listed in PubMed/Medline and conducted in intensive care units, on autonomic nervous system monitoring, via analysis of heart rate variability as a prognostic tool (mortality study). The following English terms were entered in the search field: ("autonomic nervous system" OR "heart rate variability") AND ("intensive care" OR "critical care" OR "emergency care" OR "ICU") AND ("prognosis" OR "prognoses" OR "mortality").
There was an increased likelihood of death in patients who had a decrease in heart rate variability as analyzed via heart rate variance, cardiac uncoupling, heart rate volatility, integer heart rate variability, standard deviation of NN intervals, root mean square of successive differences, total power, low frequency, very low frequency, low frequency/high frequency ratio, ratio of short-term to long-term fractal exponents, Shannon entropy, multiscale entropy and approximate entropy.
In patients admitted to intensive care units, regardless of the pathology, heart rate variability varies inversely with clinical severity and prognosis.
Abstract
Rev Bras Ter Intensiva. 2017;29(4):481-489
DOI 10.5935/0103-507X.20170072
To present a systematic review of the use of autonomic nervous system monitoring as a prognostic tool in intensive care units by assessing heart rate variability.
Literature review of studies published until July 2016 listed in PubMed/Medline and conducted in intensive care units, on autonomic nervous system monitoring, via analysis of heart rate variability as a prognostic tool (mortality study). The following English terms were entered in the search field: ("autonomic nervous system" OR "heart rate variability") AND ("intensive care" OR "critical care" OR "emergency care" OR "ICU") AND ("prognosis" OR "prognoses" OR "mortality").
There was an increased likelihood of death in patients who had a decrease in heart rate variability as analyzed via heart rate variance, cardiac uncoupling, heart rate volatility, integer heart rate variability, standard deviation of NN intervals, root mean square of successive differences, total power, low frequency, very low frequency, low frequency/high frequency ratio, ratio of short-term to long-term fractal exponents, Shannon entropy, multiscale entropy and approximate entropy.
In patients admitted to intensive care units, regardless of the pathology, heart rate variability varies inversely with clinical severity and prognosis.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):499-506
DOI 10.1590/S0103-507X2011000400016
Community-acquired pneumonia (CAP) is the most common infectious disease requiring admission to intensive care units (ICUs), and achieving an early and precise diagnosis of CAP remains a challenge. Biomarkers play an important role in improving clinical judgment in the emergency room and are adjuvant in evaluating treatment responses. Novel biomarkers, such as cortisol, pro-adrenomedullin and endothelin-1, have been shown to be associated with disease severity and short-term outcomes. This review article focuses on the clinical use of novel biomarkers, severity prediction and treatment monitoring as well as future directions of the field.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):499-506
DOI 10.1590/S0103-507X2011000400016
Community-acquired pneumonia (CAP) is the most common infectious disease requiring admission to intensive care units (ICUs), and achieving an early and precise diagnosis of CAP remains a challenge. Biomarkers play an important role in improving clinical judgment in the emergency room and are adjuvant in evaluating treatment responses. Novel biomarkers, such as cortisol, pro-adrenomedullin and endothelin-1, have been shown to be associated with disease severity and short-term outcomes. This review article focuses on the clinical use of novel biomarkers, severity prediction and treatment monitoring as well as future directions of the field.