Você pesquisou por y - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(1):96-101
DOI 10.5935/0103-507X.20210010
To evaluate changes in the characteristics of in-hospital cardiac arrest after the implementation of a Rapid Response Team.
This was a prospective observational study of in-hospital cardiac arrest that occurred from January 2013 to December 2017. The exclusion criterion was in-hospital cardiac arrest in the intensive care unit, emergency room or operating room. The Rapid Response Team was implemented in July 2014 in the study hospital. Patients were classified into two groups: a Pre-Rapid Response Team (in-hospital cardiac arrest before Rapid Response Team implementation) and a Post-Rapid Response Team (in-hospital cardiac arrest after Rapid Response Team implementation). Patients were followed until hospital discharge or death.
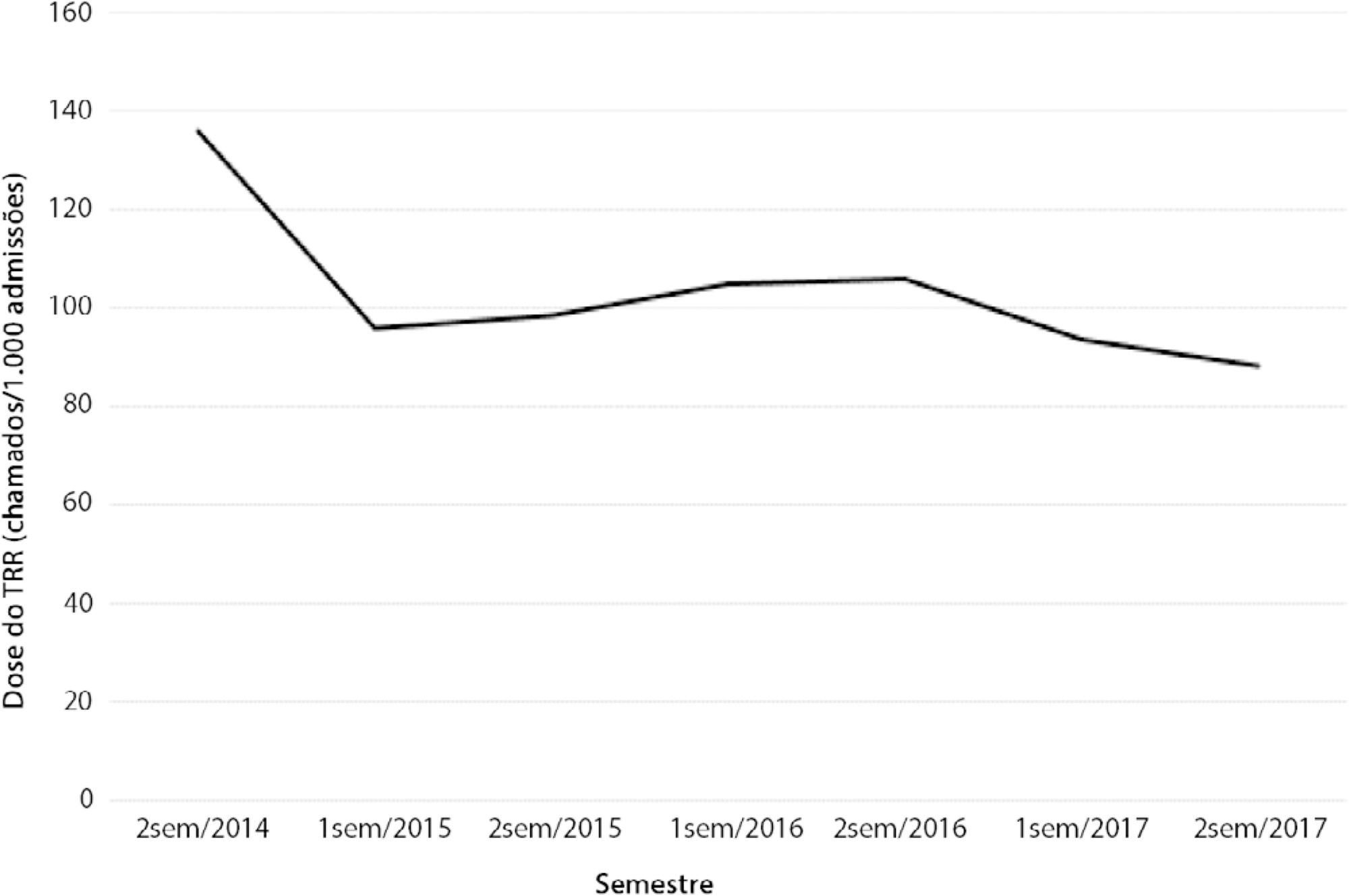
We had a total of 308 cardiac arrests (64.6 ± 15.2 years, 60.3% men, 13.9% with initial shockable rhythm). There was a decrease from 4.2 to 2.5 in-hospital cardiac arrest/1000 admissions after implementation of the Rapid Response Team, and we had approximately 124 calls/1000 admissions. Pre-Rapid Response Team cardiac arrest was associated with more hypoxia (29.4 versus 14.3%; p = 0.006) and an altered respiratory rate (14.7 versus 4.2%; p = 0.004) compared with post-Rapid Response Team cardiac arrest. Cardiac arrest due to hypoxia was more common before Rapid Response Team implementation (61.2 versus 38.1%, p < 0.001). In multivariate analysis, return of spontaneous circulation was associated with shockable rhythm (OR 2.97; IC95% 1.04 - 8.43) and witnessed cardiac arrest (OR 2.52; IC95% 1.39 - 4.59) but not with Rapid Response Team implementation (OR 1.40; IC95% 0.70 - 2.81) or premonitory signs (OR 0.71; IC95% 0.39 - 1.28). In multivariate analysis, in-hospital mortality was associated with non-shockable rhythm (OR 5.34; IC95% 2.28 - 12.53) and age (OR 1.03; IC95% 1.01 - 1.05) but not with Rapid Response Team implementation (OR 0.89; IC95% 0.40 - 2.02).
Even though Rapid Response Team implementation is associated with a reduction in in-hospital cardiac arrest, it was not associated with the mortality of in-hospital cardiac arrest victims. A significant decrease in cardiac arrests due to respiratory causes was noted after Rapid Response Team implementation.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):96-101
DOI 10.5935/0103-507X.20210010
To evaluate changes in the characteristics of in-hospital cardiac arrest after the implementation of a Rapid Response Team.
This was a prospective observational study of in-hospital cardiac arrest that occurred from January 2013 to December 2017. The exclusion criterion was in-hospital cardiac arrest in the intensive care unit, emergency room or operating room. The Rapid Response Team was implemented in July 2014 in the study hospital. Patients were classified into two groups: a Pre-Rapid Response Team (in-hospital cardiac arrest before Rapid Response Team implementation) and a Post-Rapid Response Team (in-hospital cardiac arrest after Rapid Response Team implementation). Patients were followed until hospital discharge or death.
We had a total of 308 cardiac arrests (64.6 ± 15.2 years, 60.3% men, 13.9% with initial shockable rhythm). There was a decrease from 4.2 to 2.5 in-hospital cardiac arrest/1000 admissions after implementation of the Rapid Response Team, and we had approximately 124 calls/1000 admissions. Pre-Rapid Response Team cardiac arrest was associated with more hypoxia (29.4 versus 14.3%; p = 0.006) and an altered respiratory rate (14.7 versus 4.2%; p = 0.004) compared with post-Rapid Response Team cardiac arrest. Cardiac arrest due to hypoxia was more common before Rapid Response Team implementation (61.2 versus 38.1%, p < 0.001). In multivariate analysis, return of spontaneous circulation was associated with shockable rhythm (OR 2.97; IC95% 1.04 - 8.43) and witnessed cardiac arrest (OR 2.52; IC95% 1.39 - 4.59) but not with Rapid Response Team implementation (OR 1.40; IC95% 0.70 - 2.81) or premonitory signs (OR 0.71; IC95% 0.39 - 1.28). In multivariate analysis, in-hospital mortality was associated with non-shockable rhythm (OR 5.34; IC95% 2.28 - 12.53) and age (OR 1.03; IC95% 1.01 - 1.05) but not with Rapid Response Team implementation (OR 0.89; IC95% 0.40 - 2.02).
Even though Rapid Response Team implementation is associated with a reduction in in-hospital cardiac arrest, it was not associated with the mortality of in-hospital cardiac arrest victims. A significant decrease in cardiac arrests due to respiratory causes was noted after Rapid Response Team implementation.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):96-103
DOI 10.1590/S0103-507X2009000100014
This article intends to review literature on high frequency oscillatory ventilation and describe its main clinical applications for children and neonates. Articles from the last 15 years were selected using MedLine and SciElo databases. The following key words were used: high frequency oscillatory ventilation, mechanical ventilation, acute respiratory distress syndrome, children, and new-born. The review describes high frequency oscillatory ventilation in children with acute respiratory distress syndrome, air leak syndrome, and obstructive lung disease. Respiratory distress syndrome, bronchopulmonary dysplasia, intracranial hemorrhage, periventricular leukomalacia, and air leak syndrome were reviewed in neonates. Transition from conventional mechanical ventilation to high frequency ventilation and its adjustments relating to oxygenation, CO2 elimination, chest radiography, suctioning, sedatives and use of neuromuscular blocking agents were described. Weaning and complications were also reported. For children, high frequency oscillatory ventilation is a therapeutic option, particularly in acute respiratory distress syndrome, and should be used as early as possible. It may be also useful in the air leak syndrome and obstructive pulmonary disease. Evidence that, in neonates, high frequency oscillatory ventilation is superior to conventional mechanical ventilation is lacking. However there is evidence that better results are only achieved with this ventilatory mode to manage the air leak syndrome.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):96-103
DOI 10.1590/S0103-507X2009000100014
This article intends to review literature on high frequency oscillatory ventilation and describe its main clinical applications for children and neonates. Articles from the last 15 years were selected using MedLine and SciElo databases. The following key words were used: high frequency oscillatory ventilation, mechanical ventilation, acute respiratory distress syndrome, children, and new-born. The review describes high frequency oscillatory ventilation in children with acute respiratory distress syndrome, air leak syndrome, and obstructive lung disease. Respiratory distress syndrome, bronchopulmonary dysplasia, intracranial hemorrhage, periventricular leukomalacia, and air leak syndrome were reviewed in neonates. Transition from conventional mechanical ventilation to high frequency ventilation and its adjustments relating to oxygenation, CO2 elimination, chest radiography, suctioning, sedatives and use of neuromuscular blocking agents were described. Weaning and complications were also reported. For children, high frequency oscillatory ventilation is a therapeutic option, particularly in acute respiratory distress syndrome, and should be used as early as possible. It may be also useful in the air leak syndrome and obstructive pulmonary disease. Evidence that, in neonates, high frequency oscillatory ventilation is superior to conventional mechanical ventilation is lacking. However there is evidence that better results are only achieved with this ventilatory mode to manage the air leak syndrome.
Abstract
Rev Bras Ter Intensiva. 2010;22(1):96-98
DOI 10.1590/S0103-507X2010000100016
A case of Chryseobacterium indologenes infection is reported, identified in an invasive mechanic ventilation patient's tracheal aspiration material. Epidemiological, microbiological, and intensive care unit therapy aspects are discussed. The patient was a 30 years-old male, admitted with idiopathic medullary aplasia and febrile neutropenia, referred to the intensive care unit with severe bronchopneumonia and sepsis of pulmonary origin. Most of the previously reported Chryseobacterium indologenes infection cases were associated with severe diseases and polymicrobial infections which could make difficult interpreting antimicrobial therapy options against this agent.
Abstract
Rev Bras Ter Intensiva. 2010;22(1):96-98
DOI 10.1590/S0103-507X2010000100016
A case of Chryseobacterium indologenes infection is reported, identified in an invasive mechanic ventilation patient's tracheal aspiration material. Epidemiological, microbiological, and intensive care unit therapy aspects are discussed. The patient was a 30 years-old male, admitted with idiopathic medullary aplasia and febrile neutropenia, referred to the intensive care unit with severe bronchopneumonia and sepsis of pulmonary origin. Most of the previously reported Chryseobacterium indologenes infection cases were associated with severe diseases and polymicrobial infections which could make difficult interpreting antimicrobial therapy options against this agent.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):96-101
DOI 10.5935/0103-507X.20150018
Abstract
Rev Bras Ter Intensiva. 2015;27(2):96-101
DOI 10.5935/0103-507X.20150018
Abstract
Rev Bras Ter Intensiva. 2016;28(1):96-96
DOI 10.5935/0103-507X.20160018
Abstract
Rev Bras Ter Intensiva. 2016;28(1):96-96
DOI 10.5935/0103-507X.20160018
Abstract
Rev Bras Ter Intensiva. 2017;29(1):96-104
DOI 10.5935/0103-507X.20170014
To review the literature on the effects of expiratory rib cage compression on ventilatory mechanics, airway clearance, and oxygen and hemodynamic indices in mechanically ventilated adults.
Systematic review with meta-analysis of randomized clinical trials in the databases MEDLINE (via PubMed), EMBASE, Cochrane CENTRAL, PEDro, and LILACS. Studies on adult patients hospitalized in intensive care units and under mechanical ventilation that analyzed the effects of expiratory rib cage compression with respect to a control group (without expiratory rib cage compression) and evaluated the outcomes static and dynamic compliance, sputum volume, systolic blood pressure, diastolic blood pressure, mean arterial pressure, heart rate, peripheral oxygen saturation, and ratio of arterial oxygen partial pressure to fraction of inspired oxygen were included. Experimental studies with animals and those with incomplete data were excluded.
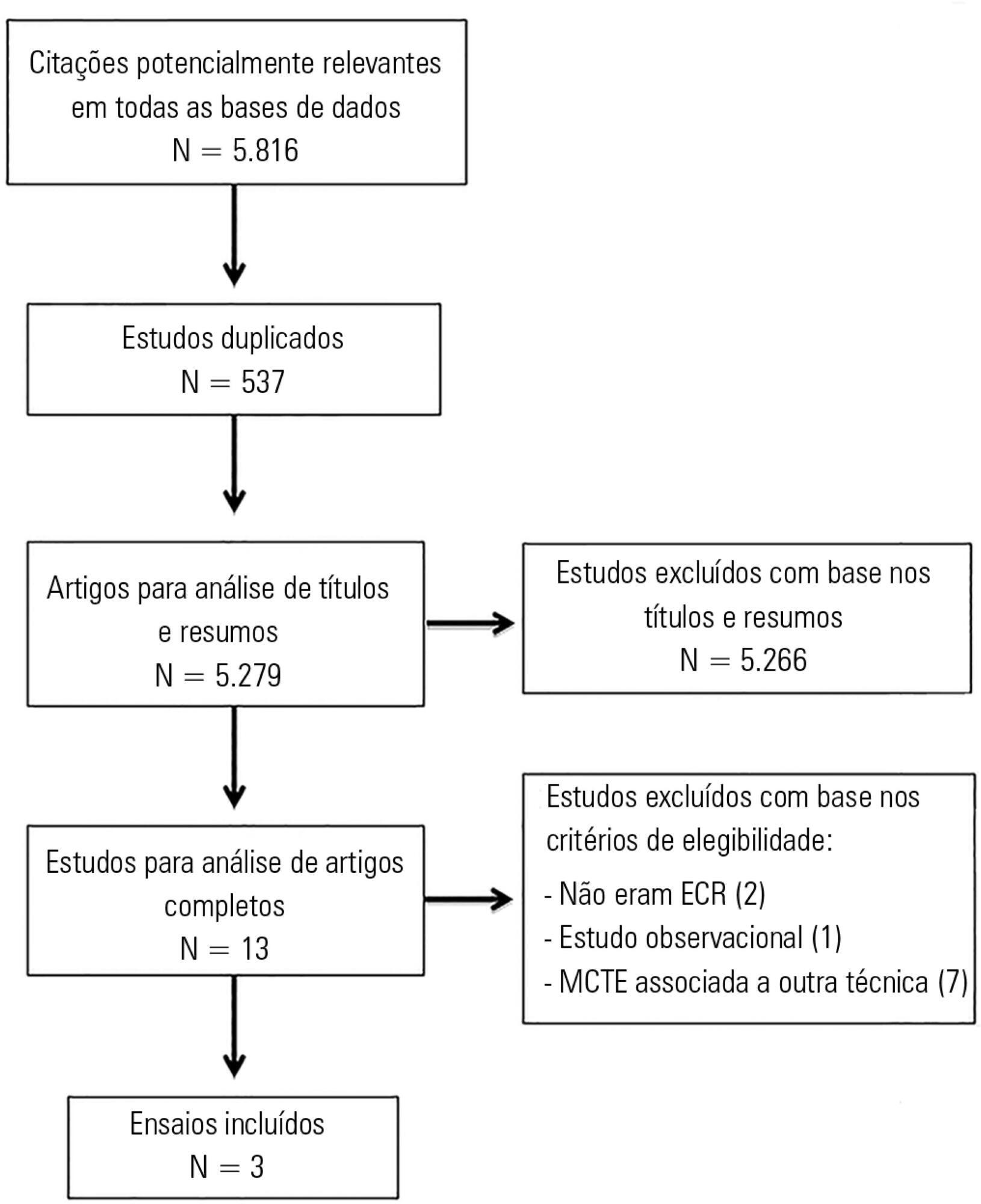
The search strategy produced 5,816 studies, of which only three randomized crossover trials were included, totaling 93 patients. With respect to the outcome of heart rate, values were reduced in the expiratory rib cage compression group compared with the control group [-2.81 bpm (95% confidence interval [95%CI]: -4.73 to 0.89; I2: 0%)]. Regarding dynamic compliance, there was no significant difference between groups [-0.58mL/cmH2O (95%CI: -2.98 to 1.82; I2: 1%)]. Regarding the variables systolic blood pressure and diastolic blood pressure, significant differences were found after descriptive evaluation. However, there was no difference between groups regarding the variables secretion volume, static compliance, ratio of arterial oxygen partial pressure to fraction of inspired oxygen, and peripheral oxygen saturation.
There is a lack of evidence to support the use of expiratory rib cage compression in routine care, given that the literature on this topic offers low methodological quality and is inconclusive.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):96-104
DOI 10.5935/0103-507X.20170014
To review the literature on the effects of expiratory rib cage compression on ventilatory mechanics, airway clearance, and oxygen and hemodynamic indices in mechanically ventilated adults.
Systematic review with meta-analysis of randomized clinical trials in the databases MEDLINE (via PubMed), EMBASE, Cochrane CENTRAL, PEDro, and LILACS. Studies on adult patients hospitalized in intensive care units and under mechanical ventilation that analyzed the effects of expiratory rib cage compression with respect to a control group (without expiratory rib cage compression) and evaluated the outcomes static and dynamic compliance, sputum volume, systolic blood pressure, diastolic blood pressure, mean arterial pressure, heart rate, peripheral oxygen saturation, and ratio of arterial oxygen partial pressure to fraction of inspired oxygen were included. Experimental studies with animals and those with incomplete data were excluded.
The search strategy produced 5,816 studies, of which only three randomized crossover trials were included, totaling 93 patients. With respect to the outcome of heart rate, values were reduced in the expiratory rib cage compression group compared with the control group [-2.81 bpm (95% confidence interval [95%CI]: -4.73 to 0.89; I2: 0%)]. Regarding dynamic compliance, there was no significant difference between groups [-0.58mL/cmH2O (95%CI: -2.98 to 1.82; I2: 1%)]. Regarding the variables systolic blood pressure and diastolic blood pressure, significant differences were found after descriptive evaluation. However, there was no difference between groups regarding the variables secretion volume, static compliance, ratio of arterial oxygen partial pressure to fraction of inspired oxygen, and peripheral oxygen saturation.
There is a lack of evidence to support the use of expiratory rib cage compression in routine care, given that the literature on this topic offers low methodological quality and is inconclusive.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):97-99
DOI 10.5935/0103-507X.20160021
Abstract
Rev Bras Ter Intensiva. 2016;28(2):97-99
DOI 10.5935/0103-507X.20160021
Abstract
Rev Bras Ter Intensiva. 2012;24(1):97-105
DOI 10.1590/S0103-507X2012000100015
This article reviews the literature, organizes the major findings, and generates the best evidence-based recommendations on nutrition therapy for head trauma patients. Despite recent advances in head trauma diagnosis and therapy, the mortality associated with this condition remains high. Few therapeutic interventions have been proven to effectively improve this condition. Head trauma causes multiple metabolic and electrolytic disorders; it is characterized by a hypermetabolic state that is associated with intensive catabolism, leading to specific nutritional needs. The current literature lacks specific guidelines for nutrition therapy in severe head trauma patients, although a substantial amount of data has been reported and relevant issues are currently being studied; these data may allow better nutrition therapy guidelines for these patients. In addition to a well-trained multi-disciplinary team, the following recommendations appear to improve outcomes: introducing nutrition therapy early; preferred enteral administration; appropriate energy intake; formulations that are tailored to specific patients, including appropriate nutrients; and strict electrolytic and metabolic monitoring. Understanding the pathophysiology and the consequences of therapy is fundamental.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):97-105
DOI 10.1590/S0103-507X2012000100015
This article reviews the literature, organizes the major findings, and generates the best evidence-based recommendations on nutrition therapy for head trauma patients. Despite recent advances in head trauma diagnosis and therapy, the mortality associated with this condition remains high. Few therapeutic interventions have been proven to effectively improve this condition. Head trauma causes multiple metabolic and electrolytic disorders; it is characterized by a hypermetabolic state that is associated with intensive catabolism, leading to specific nutritional needs. The current literature lacks specific guidelines for nutrition therapy in severe head trauma patients, although a substantial amount of data has been reported and relevant issues are currently being studied; these data may allow better nutrition therapy guidelines for these patients. In addition to a well-trained multi-disciplinary team, the following recommendations appear to improve outcomes: introducing nutrition therapy early; preferred enteral administration; appropriate energy intake; formulations that are tailored to specific patients, including appropriate nutrients; and strict electrolytic and metabolic monitoring. Understanding the pathophysiology and the consequences of therapy is fundamental.