Você pesquisou por y?yr=2008 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2008;20(3):267-277
DOI 10.1590/S0103-507X2008000300010
The present review discusses the hemodynamic and immune-modulatory effects of hypertonic saline in experimental shock and in patients with sepsis. We comment on the mechanisms of action of hypertonic saline, calling upon data in hemorrhagic and septic shock. Specific actions of hypertonic saline applicable to severe sepsis and septic shock are highlighted. Data available support potential benefits of hypertonic saline infusion in various aspects of the pathophysiology of sepsis, including tissue hypoperfusion, decreased oxygen consumption, endothelial dysfunction, cardiac depression, and the presence of a broad array of pro-inflammatory cytokines and various oxidant species. A therapy that simultaneously blocks the damaging components of sepsis will have an impact on the management of sepsis. Proper designed prospective studies may prove a beneficial role for hypertonic saline solution in the future.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):267-277
DOI 10.1590/S0103-507X2008000300010
The present review discusses the hemodynamic and immune-modulatory effects of hypertonic saline in experimental shock and in patients with sepsis. We comment on the mechanisms of action of hypertonic saline, calling upon data in hemorrhagic and septic shock. Specific actions of hypertonic saline applicable to severe sepsis and septic shock are highlighted. Data available support potential benefits of hypertonic saline infusion in various aspects of the pathophysiology of sepsis, including tissue hypoperfusion, decreased oxygen consumption, endothelial dysfunction, cardiac depression, and the presence of a broad array of pro-inflammatory cytokines and various oxidant species. A therapy that simultaneously blocks the damaging components of sepsis will have an impact on the management of sepsis. Proper designed prospective studies may prove a beneficial role for hypertonic saline solution in the future.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):278-285
DOI 10.1590/S0103-507X2008000300011
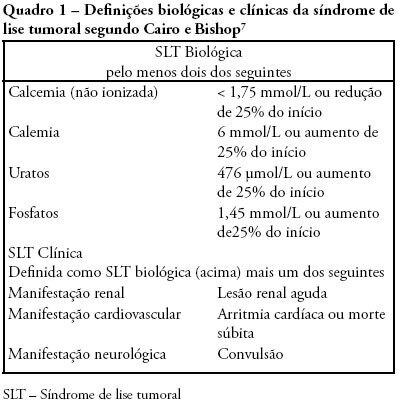
Tumor lysis syndrome is characterized by the massive destruction of malignant cells and the release in the extra-cellular space of their content. While Tumor lysis syndrome may occur spontaneously before treatment, it usually develops shortly after the initiation of cytotoxic chemotherapy. These metabolites can overwhelm the homeostatic mechanisms with development of hyperuricaemia, hyperkalaemia, hyperphosphataemia, and hypocalcaemia. These biological manifestations may lead to clinical manifestations including, acute kidney injury, seizure, or sudden death that require intensive care. Since clinical tumor lysis syndrome is associated with a poor prognosis both prevention of tumor lysis syndrome and prevention of clinical consequences of tumor lysis syndrome are mandatory. The objective of this review is to describe pathophysiological mechanisms, biological and clinical manifestations of tumor Lysis syndrome, and to provide upto-date guidelines to ensure prevention of tumor lysis syndrome. Review of selected studies on tumor lysis syndrome published at the PubMed database www.pubmed.gov during the last 20 years. Additional references were retrieved from the studies initially selected. Tumor lysis syndrome is a frequent and life-threatening complication of the newly diagnosed malignancies. Preventive measures, including hydration, uricolytic agents, eviction of factors predisposing to acute kidney injury and, in the more severe patients, on prophylactic renal replacement therapy, are required to prevent or limit clinical consequences of Tumor lysis syndrome. However optimal timing and modalities of prevention remains unknown and may be modified by the changing spectrum of patients at risk of tumor lysis syndrome. Development and validation of risk based strategies is required to limit the high morbidity and mortality of this complication.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):278-285
DOI 10.1590/S0103-507X2008000300011
Tumor lysis syndrome is characterized by the massive destruction of malignant cells and the release in the extra-cellular space of their content. While Tumor lysis syndrome may occur spontaneously before treatment, it usually develops shortly after the initiation of cytotoxic chemotherapy. These metabolites can overwhelm the homeostatic mechanisms with development of hyperuricaemia, hyperkalaemia, hyperphosphataemia, and hypocalcaemia. These biological manifestations may lead to clinical manifestations including, acute kidney injury, seizure, or sudden death that require intensive care. Since clinical tumor lysis syndrome is associated with a poor prognosis both prevention of tumor lysis syndrome and prevention of clinical consequences of tumor lysis syndrome are mandatory. The objective of this review is to describe pathophysiological mechanisms, biological and clinical manifestations of tumor Lysis syndrome, and to provide upto-date guidelines to ensure prevention of tumor lysis syndrome. Review of selected studies on tumor lysis syndrome published at the PubMed database www.pubmed.gov during the last 20 years. Additional references were retrieved from the studies initially selected. Tumor lysis syndrome is a frequent and life-threatening complication of the newly diagnosed malignancies. Preventive measures, including hydration, uricolytic agents, eviction of factors predisposing to acute kidney injury and, in the more severe patients, on prophylactic renal replacement therapy, are required to prevent or limit clinical consequences of Tumor lysis syndrome. However optimal timing and modalities of prevention remains unknown and may be modified by the changing spectrum of patients at risk of tumor lysis syndrome. Development and validation of risk based strategies is required to limit the high morbidity and mortality of this complication.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):286-295
DOI 10.1590/S0103-507X2008000300012
Considering the importance and the difficulties inherent to nutritional state assessment, as well as the results interpretation and the inexistence of specific and validated guidelines related to applied methods to the severely ill patient, the present revision aims to contribute to the analysis and recommendation of efficient methods, which are suitable to use and reliable in terms of interpretation in the context of the severely ill patient. The presence of edema and unspecific alterations in the plasmatic concentrations of proteins; altered anthropometrics variables reflecting more the rearrangement of the total body water than the nutritional state changes; inconclusive studies with electric bioimpedance; absence of data related to the application of the global subjective assessment to severely ill patients; altered biochemical markers as a consequence of the metabolic changes that, among others, indicate several method limitations to these patients. Notwithstanding the lack of studies to validate the various methods, recommendations based on clinical evidences, observation and physiopathology alterations are available. Independent from the methods, clinical observation by the health staff at all stages is mandatory. It is crucial to dedicate more efforts to identify methods and their specificity to detection, risk assessment or monitoring.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):286-295
DOI 10.1590/S0103-507X2008000300012
Considering the importance and the difficulties inherent to nutritional state assessment, as well as the results interpretation and the inexistence of specific and validated guidelines related to applied methods to the severely ill patient, the present revision aims to contribute to the analysis and recommendation of efficient methods, which are suitable to use and reliable in terms of interpretation in the context of the severely ill patient. The presence of edema and unspecific alterations in the plasmatic concentrations of proteins; altered anthropometrics variables reflecting more the rearrangement of the total body water than the nutritional state changes; inconclusive studies with electric bioimpedance; absence of data related to the application of the global subjective assessment to severely ill patients; altered biochemical markers as a consequence of the metabolic changes that, among others, indicate several method limitations to these patients. Notwithstanding the lack of studies to validate the various methods, recommendations based on clinical evidences, observation and physiopathology alterations are available. Independent from the methods, clinical observation by the health staff at all stages is mandatory. It is crucial to dedicate more efforts to identify methods and their specificity to detection, risk assessment or monitoring.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):296-304
DOI 10.1590/S0103-507X2008000300013
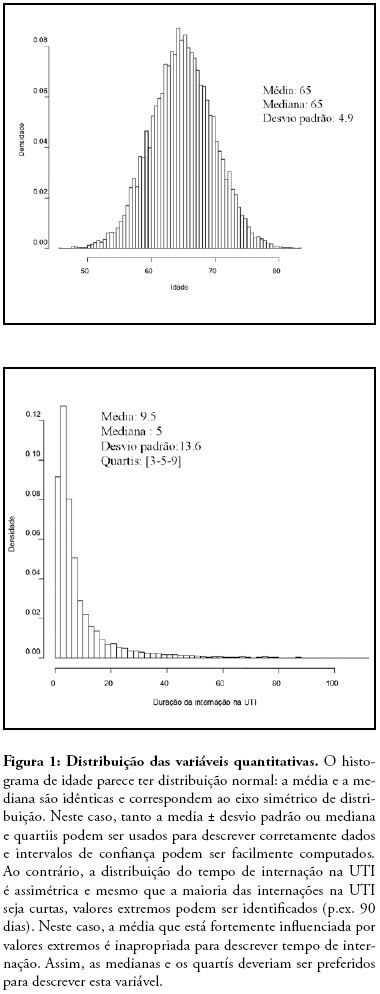
The sources of intensive care-related information and the means of communication increase rapidly. We presented here an overview of what should be done to collect high quality database. In a second part, the principle of the choice of the research question, the outcome, the explanatory variables and the statistical methods to address the question are overviewed, emphasizing major and frequent pitfalls which should be avoided.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):296-304
DOI 10.1590/S0103-507X2008000300013
The sources of intensive care-related information and the means of communication increase rapidly. We presented here an overview of what should be done to collect high quality database. In a second part, the principle of the choice of the research question, the outcome, the explanatory variables and the statistical methods to address the question are overviewed, emphasizing major and frequent pitfalls which should be avoided.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):305-312
DOI 10.1590/S0103-507X2008000300014
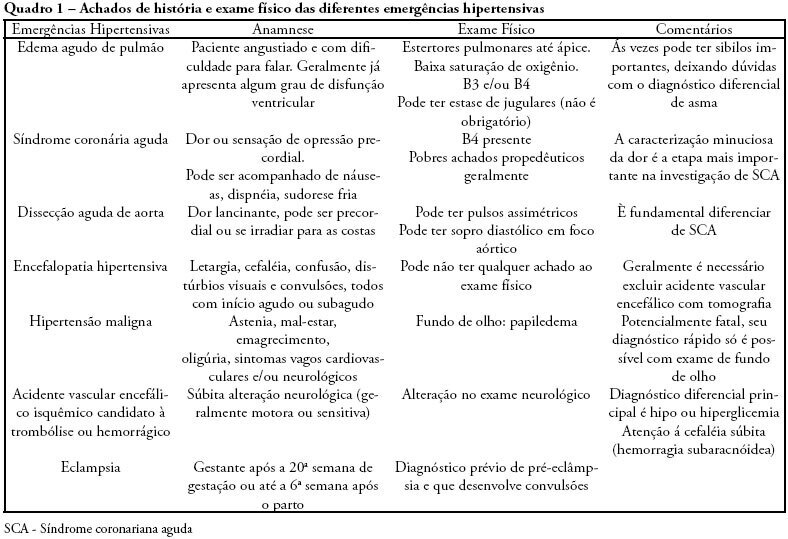
Emergencies and hypertensive crises are clinical situations which may represent more than 25% of all medical emergency care. Considering such high prevalence, physicians should be prepared to correctly identify these crises and differentiate between urgent and emergent hypertension. Approximately 3% of all visits to emergency rooms are due to significant elevation of blood pressure. Across the spectrum of blood systemic arterial pressure, hypertensive emergency is the most critical clinical situation, thus requiring special attention and care. Such patients present with high blood pressure and signs of acute specific target organ damage (such as acute myocardial infarction, unstable angina, acute pulmonary edema, eclampsia, and stroke). Key elements of diagnosis and specific treatment for the different presentations of hypertensive emergency will be reviewed in this article. The MedLine and PubMed databases were searched for pertinent abstracts, using the key words "hypertensive crises" and "hypertensive emergencies". Additional references were obtained from review articles. Available English language clinical trials, retrospective studies and review articles were identified, reviewed and summarized in a simple and practical way. The hypertensive crisis is a clinical situation characterized by acute elevation of blood pressure followed by clinical signs and symptoms. These signs and symptoms may be mild (headache, dizziness, tinnitus) or severe (dyspnea, chest pain, coma or death). If the patient presents with mild symptoms, but without acute specific target organ damage, diagnosis is hypertensive urgency. However, if severe signs and symptoms and acute specific target organ damage are present, then the patient is experiencing a hypertensive emergency. Some patients arrive at the emergency rooms with high blood pressure, but without any other sign or symptom. In these cases, they usually are not taking their medications correctly. Therefore, this is not a hypertensive crisis, but rather non-controlled chronic hypertension. This type of distinction is important for those working in emergency rooms and intensive care unit. Correct diagnosis must be made to assure the most appropriate treatment.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):305-312
DOI 10.1590/S0103-507X2008000300014
Emergencies and hypertensive crises are clinical situations which may represent more than 25% of all medical emergency care. Considering such high prevalence, physicians should be prepared to correctly identify these crises and differentiate between urgent and emergent hypertension. Approximately 3% of all visits to emergency rooms are due to significant elevation of blood pressure. Across the spectrum of blood systemic arterial pressure, hypertensive emergency is the most critical clinical situation, thus requiring special attention and care. Such patients present with high blood pressure and signs of acute specific target organ damage (such as acute myocardial infarction, unstable angina, acute pulmonary edema, eclampsia, and stroke). Key elements of diagnosis and specific treatment for the different presentations of hypertensive emergency will be reviewed in this article. The MedLine and PubMed databases were searched for pertinent abstracts, using the key words "hypertensive crises" and "hypertensive emergencies". Additional references were obtained from review articles. Available English language clinical trials, retrospective studies and review articles were identified, reviewed and summarized in a simple and practical way. The hypertensive crisis is a clinical situation characterized by acute elevation of blood pressure followed by clinical signs and symptoms. These signs and symptoms may be mild (headache, dizziness, tinnitus) or severe (dyspnea, chest pain, coma or death). If the patient presents with mild symptoms, but without acute specific target organ damage, diagnosis is hypertensive urgency. However, if severe signs and symptoms and acute specific target organ damage are present, then the patient is experiencing a hypertensive emergency. Some patients arrive at the emergency rooms with high blood pressure, but without any other sign or symptom. In these cases, they usually are not taking their medications correctly. Therefore, this is not a hypertensive crisis, but rather non-controlled chronic hypertension. This type of distinction is important for those working in emergency rooms and intensive care unit. Correct diagnosis must be made to assure the most appropriate treatment.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):313-317
DOI 10.1590/S0103-507X2008000300015
Anesthetic management of patients with severe chronic obstructive pulmonary disease is extensively discussed, due to the high rates of complications in this subtype of patients submitted to medium and high complexity surgical procedures. The objective of this study is to report use of noninvasive positive pressure mechanical ventilation - bilevel positive airway pressure - and spinal anesthesia in a patient with severe chronic obstructive pulmonary disease during total hip arthroplasty. An 81 year old, male patient with severe chronic obstructive pulmonary disease (GOLD 4) was submitted to total hip arthroplasty due to a femoral bone fracture under spinal anestesia and noninvasive positive pressure mechanical ventilation-bilevel positive airway pressure with expiratory pressure of 7 cmH2O, inspiratory pressure of 15 cmH2O and O2 flow of 3 L/min. During the procedure, the patient had one episode of bronchospasm that was promptly reverted pharmacologically with no complications in the postoperative period. The combination of less invasive anesthetic and ventilation techniques is easy to apply and may be useful in the perioperative management of patients with high anesthetic morbidity. Interaction between clinical, surgical and anesthetic teams for these cases is very important to reduce the mortality associated with extensive procedures in severe patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):313-317
DOI 10.1590/S0103-507X2008000300015
Anesthetic management of patients with severe chronic obstructive pulmonary disease is extensively discussed, due to the high rates of complications in this subtype of patients submitted to medium and high complexity surgical procedures. The objective of this study is to report use of noninvasive positive pressure mechanical ventilation - bilevel positive airway pressure - and spinal anesthesia in a patient with severe chronic obstructive pulmonary disease during total hip arthroplasty. An 81 year old, male patient with severe chronic obstructive pulmonary disease (GOLD 4) was submitted to total hip arthroplasty due to a femoral bone fracture under spinal anestesia and noninvasive positive pressure mechanical ventilation-bilevel positive airway pressure with expiratory pressure of 7 cmH2O, inspiratory pressure of 15 cmH2O and O2 flow of 3 L/min. During the procedure, the patient had one episode of bronchospasm that was promptly reverted pharmacologically with no complications in the postoperative period. The combination of less invasive anesthetic and ventilation techniques is easy to apply and may be useful in the perioperative management of patients with high anesthetic morbidity. Interaction between clinical, surgical and anesthetic teams for these cases is very important to reduce the mortality associated with extensive procedures in severe patients.

Abstract
Rev Bras Ter Intensiva. 2008;20(3):318-320
DOI 10.1590/S0103-507X2008000300016
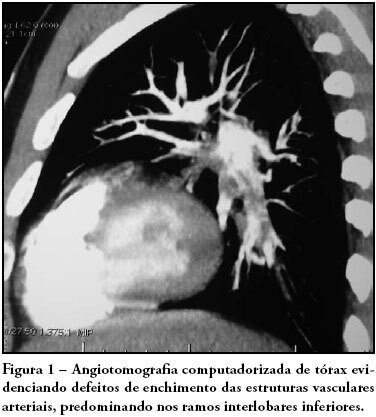
Pulmonary thromboembolism is a major cause of morbidity and mortality of patients undergoing neurosurgical procedures. The purpose of this study was to present a case of intra-arterial pulmonary thrombolysis in recent neurosurgery postoperative period. Male patient, undergoing neurosurgery, presented as a complication on the seventh day of postoperative massive pulmonary embolism with hemodynamic instability and intraarterial pulmonary thrombolysis with alteplase was indicated. Evolution was satisfactory without bleeding complications and patient was discharged. Pulmonary thromboembolism is a high morbidity and mortality condition at neurosurgical postoperative period and thrombolysis should be an alternative therapy in cases refractory to clinical treatment.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):318-320
DOI 10.1590/S0103-507X2008000300016
Pulmonary thromboembolism is a major cause of morbidity and mortality of patients undergoing neurosurgical procedures. The purpose of this study was to present a case of intra-arterial pulmonary thrombolysis in recent neurosurgery postoperative period. Male patient, undergoing neurosurgery, presented as a complication on the seventh day of postoperative massive pulmonary embolism with hemodynamic instability and intraarterial pulmonary thrombolysis with alteplase was indicated. Evolution was satisfactory without bleeding complications and patient was discharged. Pulmonary thromboembolism is a high morbidity and mortality condition at neurosurgical postoperative period and thrombolysis should be an alternative therapy in cases refractory to clinical treatment.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):321-322
DOI 10.1590/S0103-507X2008000300017
Abstract
Rev Bras Ter Intensiva. 2008;20(3):321-322
DOI 10.1590/S0103-507X2008000300017