
You searched for:"Fabio Holanda Lacerda"
We found (7) results for your search.-
Clinical Report
Prospective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
- ,
- Israel Silva Maia
 ,
, - Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini , [ … ],
- Fernando Godinho Zampieri
Abstract
Clinical ReportProspective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
Crit Care Sci. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini ,
- Júlia Souza Oliveira,
- Erica Regina Ribeiro Sady ,
- Letícia Galvão Barbante,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel,
- Lucas Petri Damiani ,
- Karina Leal Negrelli,
- Tamiris Abait Miranda,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira,
- Glauco Adrieno Westphal ,
- Ruthy Perotto Fernandes,
- Cássio Luis Zandonai ,
- Mariangela Pimentel Pincelli ,
- Rodrigo Cruvinel Figueiredo,
- Cíntia Loss Sartori Bustamante,
- Luiz Fernando Norbin,
- Emerson Boschi ,
- Rafael Lessa,
- Marcelo Pereira Romano ,
- Mieko Cláudia Miura ,
- Meton Soares de Alencar Filho ,
- Vicente Cés de Souza Dantas ,
- Priscilla Alves Barreto,
- Mauro Esteves Hernandes ,
- Cintia Magalhães Carvalho Grion ,
- Alexandre Sanches Laranjeira,
- Ana Luiza Mezzaroba ,
- Marina Bahl ,
- Ana Carolina Starke ,
- Rodrigo Santos Biondi ,
- Felipe Dal-Pizzol ,
- Eliana Bernadete Caser,
- Marlus Muri Thompson,
- Andrea Allegrini Padial,
- Viviane Cordeiro Veiga ,
- Rodrigo Thot Leite,
- Gustavo Araújo,
- Mário Guimarães,
- Priscilla de Aquino Martins ,
- Fábio Holanda Lacerda ,
- Conrado Roberto Hoffmann Filho ,
- Livia Melro ,
- Eduardo Pacheco,
- Gustavo Adolfo Ospina-Táscon ,
- Juliana Carvalho Ferreira ,
- Fabricio Jocundo Calado Freires ,
- Flávia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
- Fernando Godinho Zampieri
Views75ABSTRACT
Background:
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
Objective:
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
Methods:
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
Outcomes:
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
Conclusion:
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Keywords:Extracorporeal membrane oxygenationPneumoniaPositive pressure respirationRespiration, artificialRespiratory distress syndromeVentilator-induced lung injurySee moreViews75

Abstract
Clinical ReportProspective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
Crit Care Sci. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini ,
- Júlia Souza Oliveira,
- Erica Regina Ribeiro Sady ,
- Letícia Galvão Barbante,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel,
- Lucas Petri Damiani ,
- Karina Leal Negrelli,
- Tamiris Abait Miranda,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira,
- Glauco Adrieno Westphal ,
- Ruthy Perotto Fernandes,
- Cássio Luis Zandonai ,
- Mariangela Pimentel Pincelli ,
- Rodrigo Cruvinel Figueiredo,
- Cíntia Loss Sartori Bustamante,
- Luiz Fernando Norbin,
- Emerson Boschi ,
- Rafael Lessa,
- Marcelo Pereira Romano ,
- Mieko Cláudia Miura ,
- Meton Soares de Alencar Filho ,
- Vicente Cés de Souza Dantas ,
- Priscilla Alves Barreto,
- Mauro Esteves Hernandes ,
- Cintia Magalhães Carvalho Grion ,
- Alexandre Sanches Laranjeira,
- Ana Luiza Mezzaroba ,
- Marina Bahl ,
- Ana Carolina Starke ,
- Rodrigo Santos Biondi ,
- Felipe Dal-Pizzol ,
- Eliana Bernadete Caser,
- Marlus Muri Thompson,
- Andrea Allegrini Padial,
- Viviane Cordeiro Veiga ,
- Rodrigo Thot Leite,
- Gustavo Araújo,
- Mário Guimarães,
- Priscilla de Aquino Martins ,
- Fábio Holanda Lacerda ,
- Conrado Roberto Hoffmann Filho ,
- Livia Melro ,
- Eduardo Pacheco,
- Gustavo Adolfo Ospina-Táscon ,
- Juliana Carvalho Ferreira ,
- Fabricio Jocundo Calado Freires ,
- Flávia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
- Fernando Godinho Zampieri
Views75ABSTRACT
Background:
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
Objective:
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
Methods:
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
Outcomes:
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
Conclusion:
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Keywords:Extracorporeal membrane oxygenationPneumoniaPositive pressure respirationRespiration, artificialRespiratory distress syndromeVentilator-induced lung injurySee more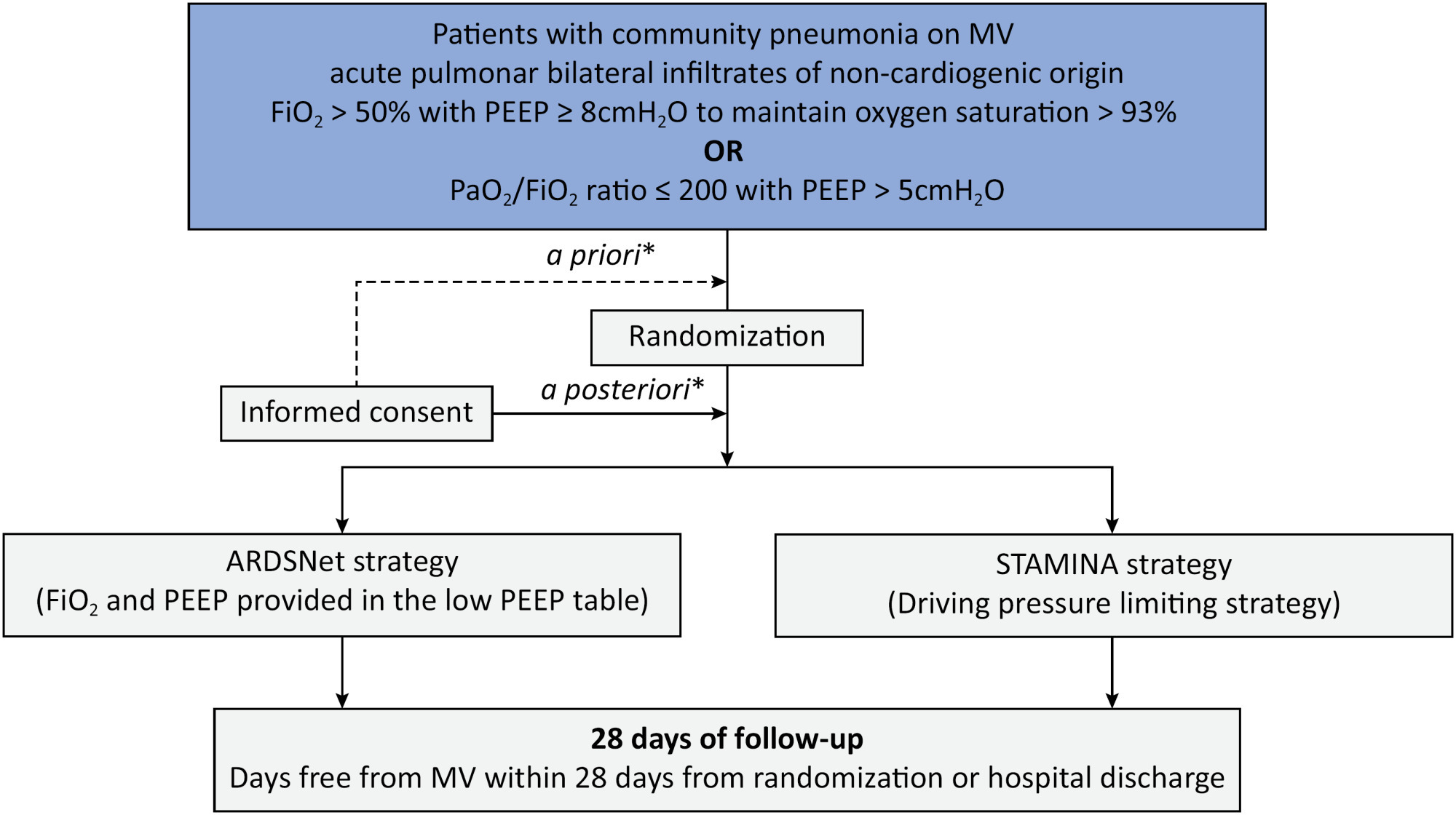
-
Letter to the Editor
Endotracheal intubation in COVID-19 patients in Brazil: a nationwide survey
- Pedro Vitale Mendes ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fábio Holanda Lacerda ,
- João Gabriel Rosa Ramos ,
- Leandro Utino Taniguchi
Abstract
Letter to the EditorEndotracheal intubation in COVID-19 patients in Brazil: a nationwide survey
Rev Bras Ter Intensiva. 2022;34(1):202-204
DOI 10.5935/0103-507X.20220015-en
- Pedro Vitale Mendes ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fábio Holanda Lacerda ,
- João Gabriel Rosa Ramos ,
- Leandro Utino Taniguchi
Views2To the Editor Endotracheal intubation is a life-saving procedure in acute respiratory distress syndrome. However, complications such as hypoxia, hypotension and cardiovascular collapse may occur in almost 40% of the procedures in the intensive care unit (ICU).() Evidence regarding the best practice of endotracheal intubation in this context is scarce, and most data have been […]See moreViews2Abstract
Letter to the EditorEndotracheal intubation in COVID-19 patients in Brazil: a nationwide survey
Rev Bras Ter Intensiva. 2022;34(1):202-204
DOI 10.5935/0103-507X.20220015-en
- Pedro Vitale Mendes ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fábio Holanda Lacerda ,
- João Gabriel Rosa Ramos ,
- Leandro Utino Taniguchi
Views2To the Editor Endotracheal intubation is a life-saving procedure in acute respiratory distress syndrome. However, complications such as hypoxia, hypotension and cardiovascular collapse may occur in almost 40% of the procedures in the intensive care unit (ICU).() Evidence regarding the best practice of endotracheal intubation in this context is scarce, and most data have been […]See more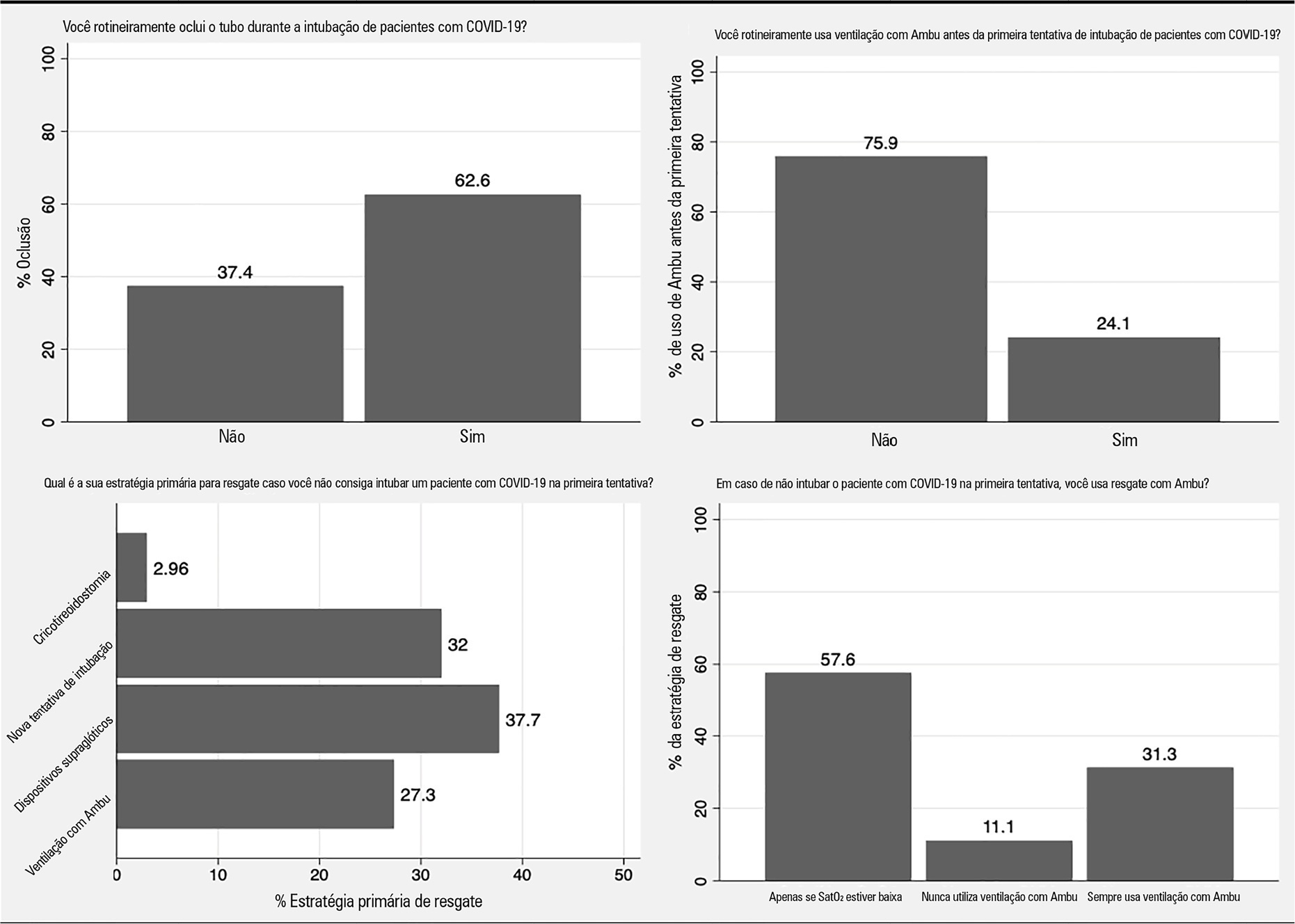
- Pedro Vitale Mendes
-
Original Article
Mechanical ventilation withdrawal as a palliative procedure in a Brazilian intensive care unit
- Fábio Holanda Lacerda ,
- Pedro Garcia Checoli,
- Carla Marchini Dias da Silva,
- Carlos Eduardo Brandão,
- Daniel Neves Forte, [ … ],
- Bruno Adler Maccagnan Pinheiro Besen
Abstract
Original ArticleMechanical ventilation withdrawal as a palliative procedure in a Brazilian intensive care unit
Rev Bras Ter Intensiva. 2020;32(4):528-534
DOI 10.5935/0103-507X.20200090
- Fábio Holanda Lacerda ,
- Pedro Garcia Checoli,
- Carla Marchini Dias da Silva,
- Carlos Eduardo Brandão,
- Daniel Neves Forte,
- Bruno Adler Maccagnan Pinheiro Besen
Views1See moreAbstract
Objective:
To describe the characteristics and outcomes of patients undergoing mechanical ventilation withdrawal and to compare them to mechanically ventilated patients with limitations (withhold or withdrawal) of life-sustaining therapies but who did not undergo mechanical ventilation withdrawal.
Methods:
This was a retrospective cohort study from January 2014 to December 2018 of mechanically ventilated patients with any organ support limitation admitted to a single intensive care unit. We compared patients who underwent mechanical ventilation withdrawal and those who did not regarding intensive care unit and hospital mortality and length of stay in both an unadjusted analysis and a propensity score matched subsample. We also analyzed the time from mechanical ventilation withdrawal to death.
Results:
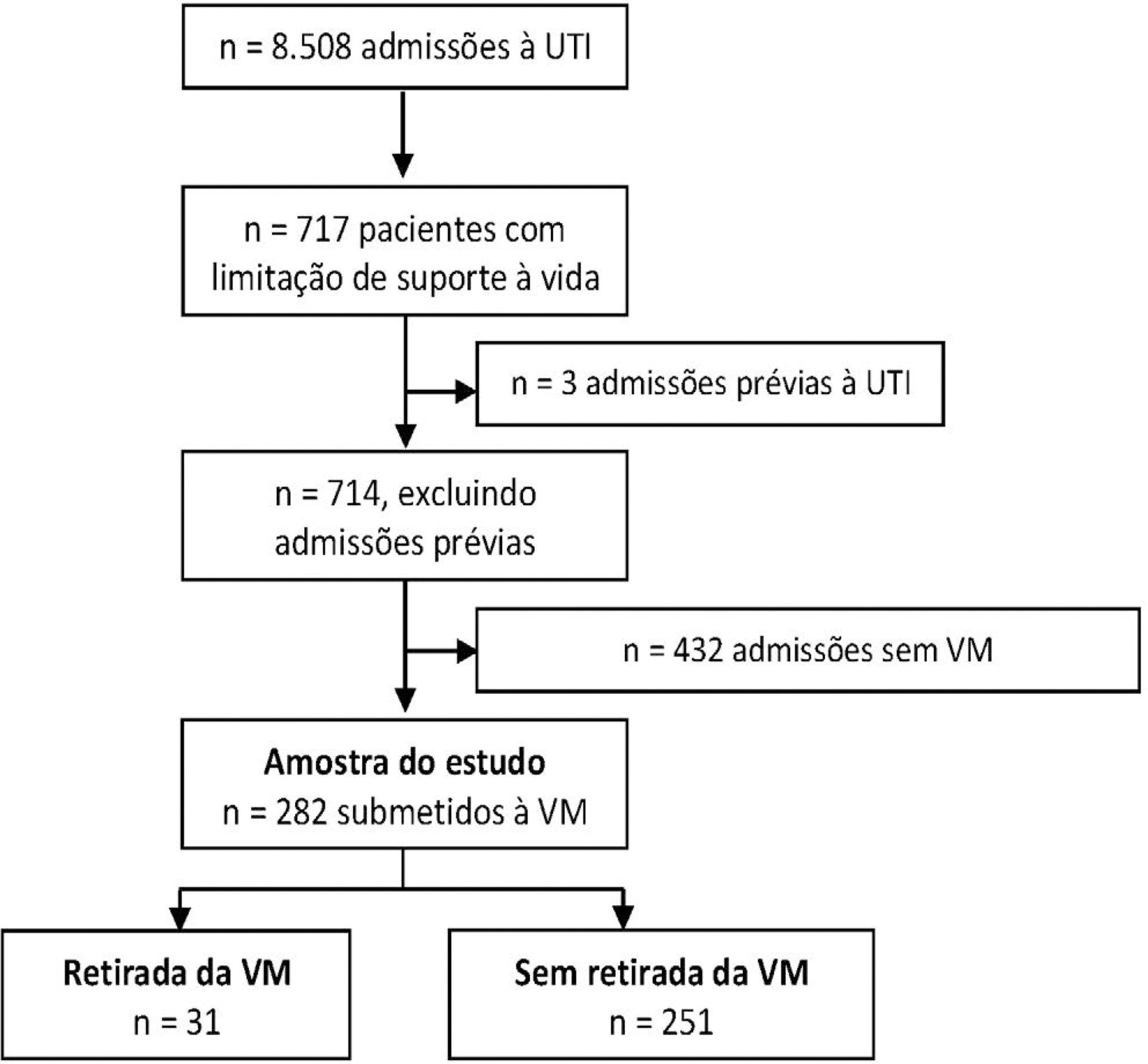
Out of 282 patients with life-sustaining therapy limitations, 31 (11%) underwent mechanical ventilation withdrawal. There was no baseline difference between groups. Intensive care unit and hospital mortality rates were 71% versus 57% and 93% versus 80%, respectively, among patients who underwent mechanical ventilation withdrawal and those who did not. The median intensive care unit length of stay was 7 versus 8 days (p = 0.6), and the hospital length of stay was 9 versus 15 days (p = 0.015). Hospital mortality was not significantly different (25/31; 81% versus 29/31; 93%; p = 0.26) after matching. The median time from mechanical ventilation withdrawal until death was 2 days [0 – 5], and 10/31 (32%) patients died within 24 hours after mechanical ventilation withdrawal.
Conclusion:
In this Brazilian report, mechanical ventilation withdrawal represented 11% of all patients with treatment limitations and was not associated with increased hospital mortality after propensity score matching on relevant covariates.
Views1Abstract
Original ArticleMechanical ventilation withdrawal as a palliative procedure in a Brazilian intensive care unit
Rev Bras Ter Intensiva. 2020;32(4):528-534
DOI 10.5935/0103-507X.20200090
- Fábio Holanda Lacerda ,
- Pedro Garcia Checoli,
- Carla Marchini Dias da Silva,
- Carlos Eduardo Brandão,
- Daniel Neves Forte,
- Bruno Adler Maccagnan Pinheiro Besen
Views1See moreAbstract
Objective:
To describe the characteristics and outcomes of patients undergoing mechanical ventilation withdrawal and to compare them to mechanically ventilated patients with limitations (withhold or withdrawal) of life-sustaining therapies but who did not undergo mechanical ventilation withdrawal.
Methods:
This was a retrospective cohort study from January 2014 to December 2018 of mechanically ventilated patients with any organ support limitation admitted to a single intensive care unit. We compared patients who underwent mechanical ventilation withdrawal and those who did not regarding intensive care unit and hospital mortality and length of stay in both an unadjusted analysis and a propensity score matched subsample. We also analyzed the time from mechanical ventilation withdrawal to death.
Results:
Out of 282 patients with life-sustaining therapy limitations, 31 (11%) underwent mechanical ventilation withdrawal. There was no baseline difference between groups. Intensive care unit and hospital mortality rates were 71% versus 57% and 93% versus 80%, respectively, among patients who underwent mechanical ventilation withdrawal and those who did not. The median intensive care unit length of stay was 7 versus 8 days (p = 0.6), and the hospital length of stay was 9 versus 15 days (p = 0.015). Hospital mortality was not significantly different (25/31; 81% versus 29/31; 93%; p = 0.26) after matching. The median time from mechanical ventilation withdrawal until death was 2 days [0 – 5], and 10/31 (32%) patients died within 24 hours after mechanical ventilation withdrawal.
Conclusion:
In this Brazilian report, mechanical ventilation withdrawal represented 11% of all patients with treatment limitations and was not associated with increased hospital mortality after propensity score matching on relevant covariates.
- Fábio Holanda Lacerda
-
Original Article
Statistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo, [ … ],
- Fernando Godinho Zampieri
Abstract
Original ArticleStatistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
Rev Bras Ter Intensiva. 2020;32(4):493-505
DOI 10.5935/0103-507X.20200081
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo,
- Wilson José Lovato,
- Cristina Prata Amêndola,
- Ary Serpa Neto ,
- Jorge Luiz da Rocha Paranhos,
- Viviane Cordeiro Veiga ,
- Marco Antonio Vieira Guedes,
- Eraldo de Azevedo Lúcio,
- Lúcio Couto Oliveira Júnior,
- Thiago Costa Lisboa,
- Fabio Holanda Lacerda ,
- Tamiris Abait Miranda,
- Israel Silva Maia ,
- Cintia Magalhães Carvalho Grion ,
- Flavia Ribeiro Machado,
- Fernando Godinho Zampieri
Views1See moreAbstract
Objective:
To report the statistical analysis plan (first version) for the Balanced Solutions versus Saline in Intensive Care Study (BaSICS).
Methods:
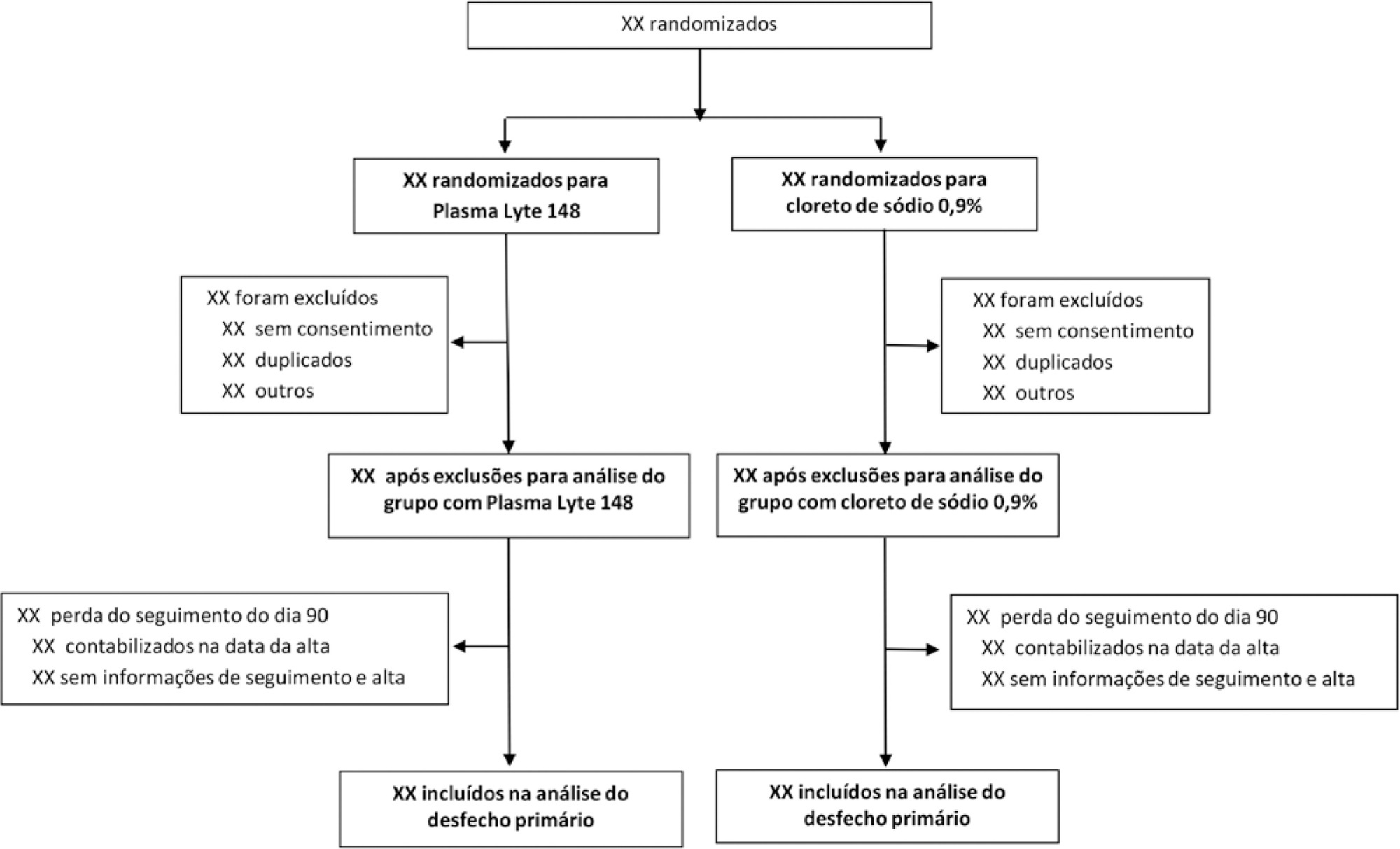
BaSICS is a multicenter factorial randomized controlled trial that will assess the effects of Plasma-Lyte 148 versus 0.9% saline as the fluid of choice in critically ill patients, as well as the effects of a slow (333mL/h) versus rapid (999mL/h) infusion speed during fluid challenges, on important patient outcomes. The fluid type will be blinded for investigators, patients and the analyses. No blinding will be possible for the infusion speed for the investigators, but all analyses will be kept blinded during the analysis procedure.
Results:
BaSICS will have 90-day mortality as its primary endpoint, which will be tested using mixed-effects Cox proportional hazard models, considering sites as a random variable (frailty models) adjusted for age, organ dysfunction and admission type. Important secondary endpoints include renal replacement therapy up to 90 days, acute renal failure, organ dysfunction at days 3 and 7, and mechanical ventilation-free days within 28 days.
Conclusion:
This manuscript provides details on the first version of the statistical analysis plan for the BaSICS trial and will guide the study’s analysis when follow-up is finished.
Views1Abstract
Original ArticleStatistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
Rev Bras Ter Intensiva. 2020;32(4):493-505
DOI 10.5935/0103-507X.20200081
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo,
- Wilson José Lovato,
- Cristina Prata Amêndola,
- Ary Serpa Neto ,
- Jorge Luiz da Rocha Paranhos,
- Viviane Cordeiro Veiga ,
- Marco Antonio Vieira Guedes,
- Eraldo de Azevedo Lúcio,
- Lúcio Couto Oliveira Júnior,
- Thiago Costa Lisboa,
- Fabio Holanda Lacerda ,
- Tamiris Abait Miranda,
- Israel Silva Maia ,
- Cintia Magalhães Carvalho Grion ,
- Flavia Ribeiro Machado,
- Fernando Godinho Zampieri
Views1See moreAbstract
Objective:
To report the statistical analysis plan (first version) for the Balanced Solutions versus Saline in Intensive Care Study (BaSICS).
Methods:
BaSICS is a multicenter factorial randomized controlled trial that will assess the effects of Plasma-Lyte 148 versus 0.9% saline as the fluid of choice in critically ill patients, as well as the effects of a slow (333mL/h) versus rapid (999mL/h) infusion speed during fluid challenges, on important patient outcomes. The fluid type will be blinded for investigators, patients and the analyses. No blinding will be possible for the infusion speed for the investigators, but all analyses will be kept blinded during the analysis procedure.
Results:
BaSICS will have 90-day mortality as its primary endpoint, which will be tested using mixed-effects Cox proportional hazard models, considering sites as a random variable (frailty models) adjusted for age, organ dysfunction and admission type. Important secondary endpoints include renal replacement therapy up to 90 days, acute renal failure, organ dysfunction at days 3 and 7, and mechanical ventilation-free days within 28 days.
Conclusion:
This manuscript provides details on the first version of the statistical analysis plan for the BaSICS trial and will guide the study’s analysis when follow-up is finished.
-
Original Article
Neuromuscular blockade and airway management during endotracheal intubation in Brazilian intensive care units: a national survey
- Pedro Vitale Mendes ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fabio Holanda Lacerda ,
- João Gabriel Rosa Ramos ,
- Leandro Utino Taniguchi
Abstract
Original ArticleNeuromuscular blockade and airway management during endotracheal intubation in Brazilian intensive care units: a national survey
Rev Bras Ter Intensiva. 2020;32(3):433-438
DOI 10.5935/0103-507X.20200073
- Pedro Vitale Mendes ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fabio Holanda Lacerda ,
- João Gabriel Rosa Ramos ,
- Leandro Utino Taniguchi
Views0Abstract
Objective:
To describe the use of neuromuscular blockade as well as other practices among Brazilian physicians in adult intensive care units.
Methods:
An online national survey was designed and administered to Brazilian intensivists. Questions were selected using the Delphi method and assessed physicians’ demographic data, intensive care unit characteristics, practices regarding airway management, use of neuromuscular blockade and sedation during endotracheal intubation in the intensive care unit. As a secondary outcome, we applied a multivariate analysis to evaluate factors associated with the use of neuromuscular blockade.
Results:
Five hundred sixty-five intensivists from all Brazilian regions responded to the questionnaire. The majority of respondents were male (65%), with a mean age of 38 ( 8.4 years, and 58.5% had a board certification in critical care. Only 40.7% of the intensivists reported the use of neuromuscular blockade during all or in more than 75% of endotracheal intubations. In the multivariate analysis, the number of intubations performed monthly and physician specialization in anesthesiology were directly associated with frequent use of neuromuscular blockade. Etomidate and ketamine were more commonly used in the clinical situation of hypotension and shock, while propofol and midazolam were more commonly prescribed in the situation of clinical stability.
Conclusion:
The reported use of neuromuscular blockade was low among intensivists, and sedative drugs were chosen in accordance with patient hemodynamic stability. These results may help the design of future studies regarding airway management in Brazil.
Keywords:Airway managementBrazilHypnotics and sedativesIntensive care unitsIntubationNeuromuscular blockadeSee moreViews0Abstract
Original ArticleNeuromuscular blockade and airway management during endotracheal intubation in Brazilian intensive care units: a national survey
Rev Bras Ter Intensiva. 2020;32(3):433-438
DOI 10.5935/0103-507X.20200073
- Pedro Vitale Mendes ,
- Bruno Adler Maccagnan Pinheiro Besen ,
- Fabio Holanda Lacerda ,
- João Gabriel Rosa Ramos ,
- Leandro Utino Taniguchi
Views0Abstract
Objective:
To describe the use of neuromuscular blockade as well as other practices among Brazilian physicians in adult intensive care units.
Methods:
An online national survey was designed and administered to Brazilian intensivists. Questions were selected using the Delphi method and assessed physicians’ demographic data, intensive care unit characteristics, practices regarding airway management, use of neuromuscular blockade and sedation during endotracheal intubation in the intensive care unit. As a secondary outcome, we applied a multivariate analysis to evaluate factors associated with the use of neuromuscular blockade.
Results:
Five hundred sixty-five intensivists from all Brazilian regions responded to the questionnaire. The majority of respondents were male (65%), with a mean age of 38 ( 8.4 years, and 58.5% had a board certification in critical care. Only 40.7% of the intensivists reported the use of neuromuscular blockade during all or in more than 75% of endotracheal intubations. In the multivariate analysis, the number of intubations performed monthly and physician specialization in anesthesiology were directly associated with frequent use of neuromuscular blockade. Etomidate and ketamine were more commonly used in the clinical situation of hypotension and shock, while propofol and midazolam were more commonly prescribed in the situation of clinical stability.
Conclusion:
The reported use of neuromuscular blockade was low among intensivists, and sedative drugs were chosen in accordance with patient hemodynamic stability. These results may help the design of future studies regarding airway management in Brazil.
Keywords:Airway managementBrazilHypnotics and sedativesIntensive care unitsIntubationNeuromuscular blockadeSee more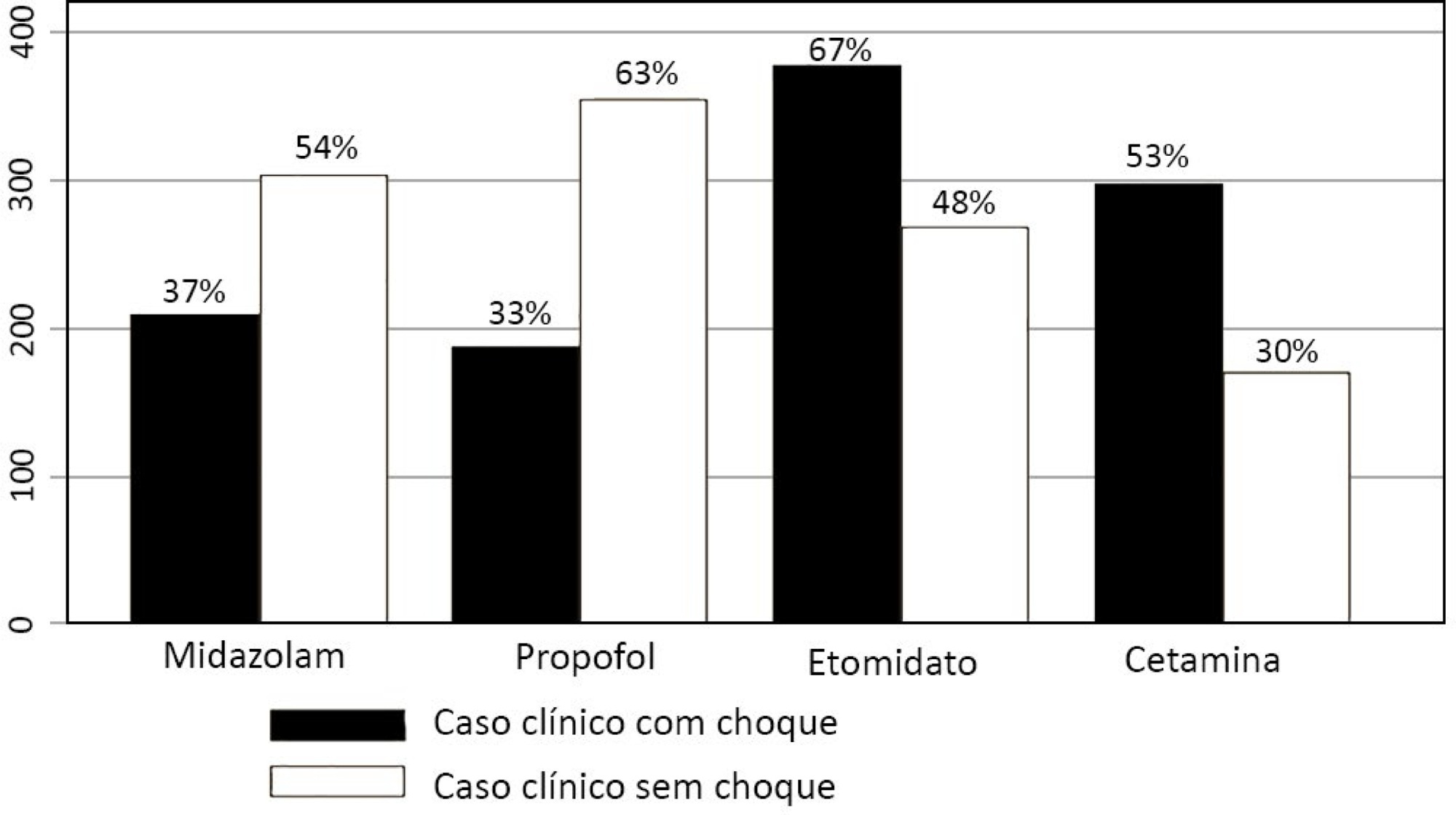
- Pedro Vitale Mendes
-
Original Articles
Pain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza, [ … ],
- Lucas Fernandes de Oliveira
Abstract
Original ArticlesPain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
Rev Bras Ter Intensiva. 2019;31(4):447-455
DOI 10.5935/0103-507X.20190085
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza,
- Eliana Vieira do Nascimento Martins,
- Ana Tarina Alvarez Lopes,
- Carlos Eduardo Brandão,
- Lucas Fernandes de Oliveira
Views1See moreABSTRACT
Objective:
To evaluate the impact of an opioid-sparing pain management protocol on overall opioid consumption and clinical outcomes.
Methods:
This was a single-center, quasi-experimental, retrospective, before and after cohort study. We used an interrupted time series to analyze changes in the levels and trends of the utilization of different analgesics. We used bivariate comparisons in the before and after cohorts as well as logistic regression and quantile regression for adjusted estimates.
Results:
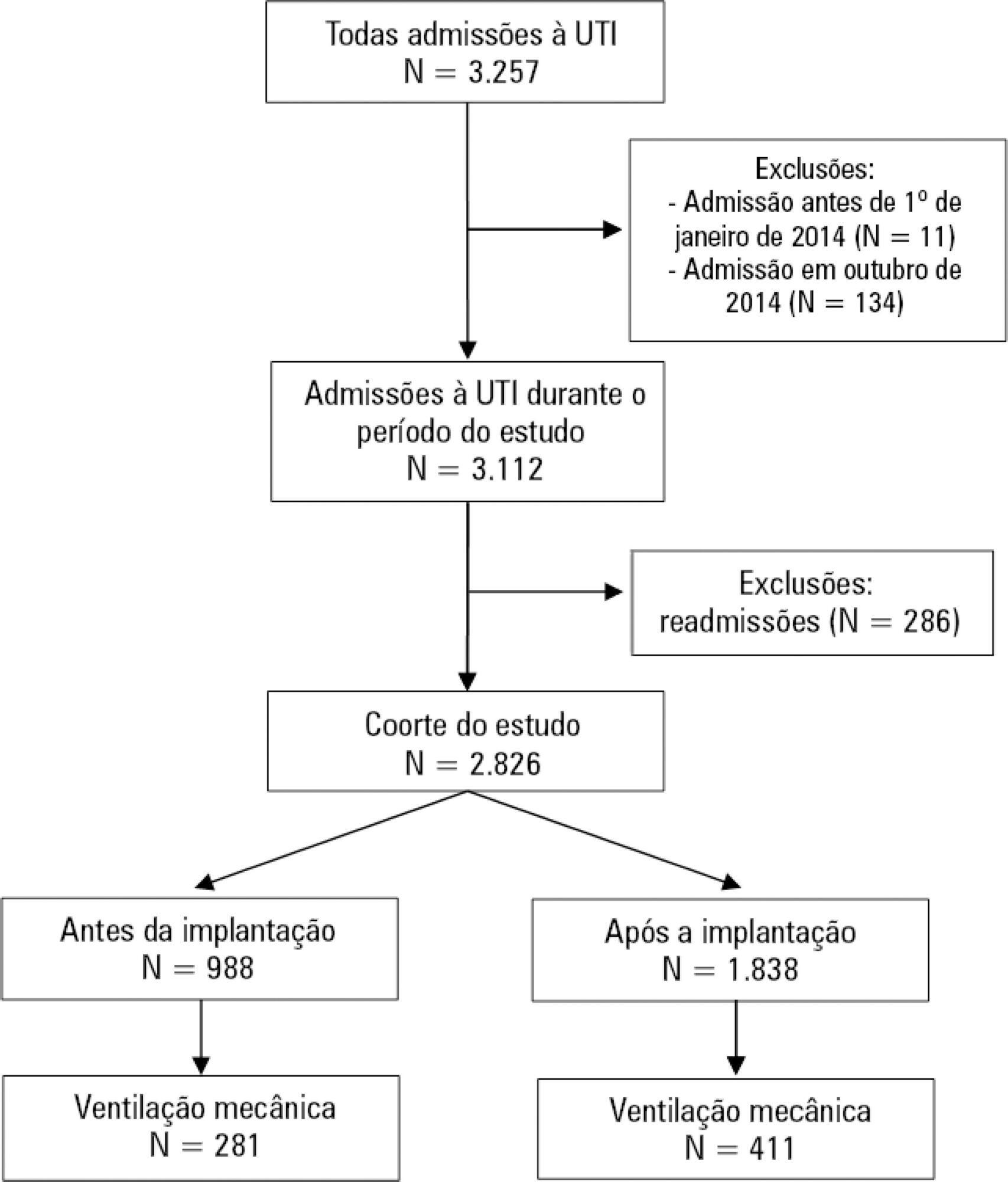
We included 988 patients in the preintervention period and 1,838 in the postintervention period. Fentanyl consumption was slightly increasing before the intervention (β = 16; 95%CI 7 – 25; p = 0.002) but substantially decreased in level with the intervention (β = – 128; 95%CI -195 – -62; p = 0.001) and then progressively decreased (β = – 24; 95%CI -35 – -13; p < 0.001). There was an increasing trend in the utilization of dipyrone. The mechanical ventilation duration was significantly lower (median difference: - 1 day; 95%CI -1 - 0; p < 0.001), especially for patients who were mechanically ventilated for a longer time (50th percentile difference: -0.78; 95%CI -1.51 – -0.05; p = 0.036; 75th percentile difference: -2.23; 95%CI -3.47 – -0.98; p < 0.001).
Conclusion:
A pain management protocol could reduce the intensive care unit consumption of fentanyl. This strategy was associated with a shorter mechanical ventilation duration.
Views1Abstract
Original ArticlesPain management protocol implementation and opioid consumption in critical care: an interrupted time series analysis
Rev Bras Ter Intensiva. 2019;31(4):447-455
DOI 10.5935/0103-507X.20190085
- Bruno Adler Maccagnan Pinheiro Besen ,
- Antonio Paulo Nassar Júnior ,
- Fábio Holanda Lacerda,
- Carla Marchini Dias da Silva,
- Vanessa Tota de Souza,
- Eliana Vieira do Nascimento Martins,
- Ana Tarina Alvarez Lopes,
- Carlos Eduardo Brandão,
- Lucas Fernandes de Oliveira
Views1See moreABSTRACT
Objective:
To evaluate the impact of an opioid-sparing pain management protocol on overall opioid consumption and clinical outcomes.
Methods:
This was a single-center, quasi-experimental, retrospective, before and after cohort study. We used an interrupted time series to analyze changes in the levels and trends of the utilization of different analgesics. We used bivariate comparisons in the before and after cohorts as well as logistic regression and quantile regression for adjusted estimates.
Results:
We included 988 patients in the preintervention period and 1,838 in the postintervention period. Fentanyl consumption was slightly increasing before the intervention (β = 16; 95%CI 7 – 25; p = 0.002) but substantially decreased in level with the intervention (β = – 128; 95%CI -195 – -62; p = 0.001) and then progressively decreased (β = – 24; 95%CI -35 – -13; p < 0.001). There was an increasing trend in the utilization of dipyrone. The mechanical ventilation duration was significantly lower (median difference: - 1 day; 95%CI -1 - 0; p < 0.001), especially for patients who were mechanically ventilated for a longer time (50th percentile difference: -0.78; 95%CI -1.51 – -0.05; p = 0.036; 75th percentile difference: -2.23; 95%CI -3.47 – -0.98; p < 0.001).
Conclusion:
A pain management protocol could reduce the intensive care unit consumption of fentanyl. This strategy was associated with a shorter mechanical ventilation duration.
- Bruno Adler Maccagnan Pinheiro Besen
-
Brief Communication
Intracranial epidural hematoma follow-up using bidimensional ultrasound
Rev Bras Ter Intensiva. 2017;29(2):259-260
Abstract
Brief CommunicationIntracranial epidural hematoma follow-up using bidimensional ultrasound
Rev Bras Ter Intensiva. 2017;29(2):259-260
DOI 10.5935/0103-507X.20170036
Views1Bidimensional encephalic ultrasound can be used to diagnose several types of lesions as epidural hematomas.() To illustrate this use, we present a patient in which an epidural hematoma was monitored through the use of a hemicraniectomy bidimensional ultrasound.A 28-year-old male patient was found unconscious after a fall from a platform. He was promptly given medical […]See moreViews1Abstract
Brief CommunicationIntracranial epidural hematoma follow-up using bidimensional ultrasound
Rev Bras Ter Intensiva. 2017;29(2):259-260
DOI 10.5935/0103-507X.20170036
Views1Bidimensional encephalic ultrasound can be used to diagnose several types of lesions as epidural hematomas.() To illustrate this use, we present a patient in which an epidural hematoma was monitored through the use of a hemicraniectomy bidimensional ultrasound.A 28-year-old male patient was found unconscious after a fall from a platform. He was promptly given medical […]See more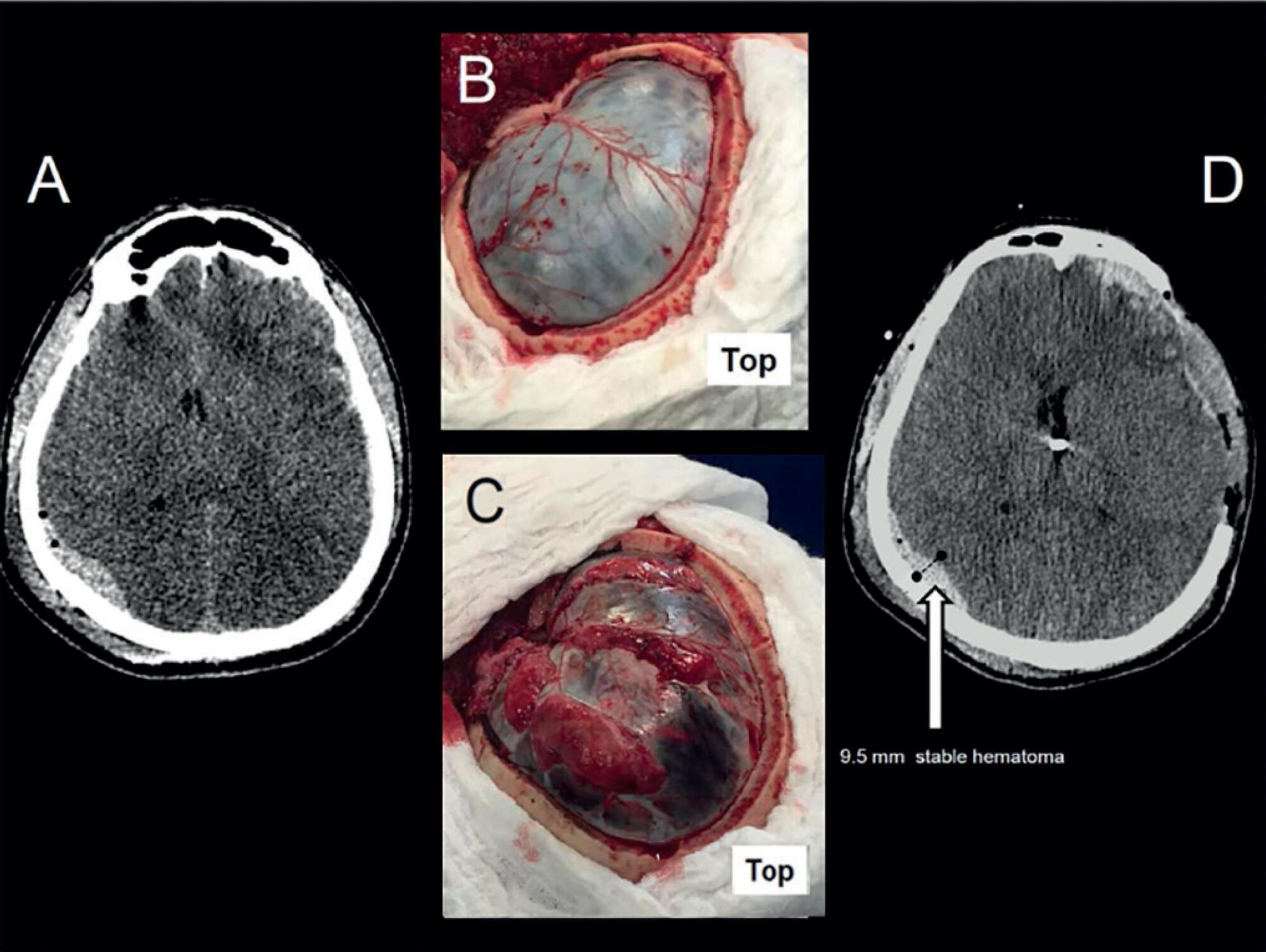
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis