
You searched for:"Alejandro Risso Vazquez"
We found (4) results for your search.-
Original Article
Prognostic value of ventricular diastolic dysfunction in patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):333-339
Abstract
Original ArticlePrognostic value of ventricular diastolic dysfunction in patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):333-339
DOI 10.5935/0103-507X.20150057
Views0See moreABSTRACT
Objectives:
To evaluate the prevalence of myocardial dysfunction and its prognostic value in patients with severe sepsis and septic shock.
Methods:
Adult septic patients admitted to an intensive care unit were prospectively studied using transthoracic echocardiography within the first 48 hours after admission and thereafter on the 7th-10th days. Echocardiographic variables of biventricular function, including the E/e’ ratio, were compared between survivors and non-survivors.
Results:
A total of 99 echocardiograms (53 at admission and 46 between days 7 – 10) were performed on 53 patients with a mean age of 74 (SD 13) years. Systolic and diastolic dysfunction was present in 14 (26%) and 42 (83%) patients, respectively, and both types of dysfunction were present in 12 (23%) patients. The E/e’ ratio, an index of diastolic dysfunction, was the best predictor of hospital mortality according to the area under the ROC curve (0.71) and was an independent predictor of outcome, as determined by multivariate analysis (OR = 1.36 [1.05 – 1.76], p = 0.02).
Conclusion:
In septic patients admitted to an intensive care unit, echocardiographic systolic dysfunction is not associated with increased mortality. In contrast, diastolic dysfunction is an independent predictor of outcome.
Views0

Abstract
Original ArticlePrognostic value of ventricular diastolic dysfunction in patients with severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(4):333-339
DOI 10.5935/0103-507X.20150057
Views0See moreABSTRACT
Objectives:
To evaluate the prevalence of myocardial dysfunction and its prognostic value in patients with severe sepsis and septic shock.
Methods:
Adult septic patients admitted to an intensive care unit were prospectively studied using transthoracic echocardiography within the first 48 hours after admission and thereafter on the 7th-10th days. Echocardiographic variables of biventricular function, including the E/e’ ratio, were compared between survivors and non-survivors.
Results:
A total of 99 echocardiograms (53 at admission and 46 between days 7 – 10) were performed on 53 patients with a mean age of 74 (SD 13) years. Systolic and diastolic dysfunction was present in 14 (26%) and 42 (83%) patients, respectively, and both types of dysfunction were present in 12 (23%) patients. The E/e’ ratio, an index of diastolic dysfunction, was the best predictor of hospital mortality according to the area under the ROC curve (0.71) and was an independent predictor of outcome, as determined by multivariate analysis (OR = 1.36 [1.05 – 1.76], p = 0.02).
Conclusion:
In septic patients admitted to an intensive care unit, echocardiographic systolic dysfunction is not associated with increased mortality. In contrast, diastolic dysfunction is an independent predictor of outcome.
-
Original Articles
Augmented renal clearance in critically ill patients: incidence, associated factors and effects on vancomycin treatment
Rev Bras Ter Intensiva. 2014;26(1):13-20
Abstract
Original ArticlesAugmented renal clearance in critically ill patients: incidence, associated factors and effects on vancomycin treatment
Rev Bras Ter Intensiva. 2014;26(1):13-20
DOI 10.5935/0103-507X.20140003
Views8Objective:
An augmented renal clearance has been described in some groups of critically ill patients, and it might induce sub-optimal concentrations of drugs eliminated by glomerular filtration, mainly antibiotics. Studies on its occurrence and determinants are lacking. Our goals were to determine the incidence and associated factors of augmented renal clearance and the effects on vancomycin concentrations and dosing in a series of intensive care unit patients.
Methods:
We prospectively studied 363 patients admitted during 1 year to a clinical-surgical intensive care unit. Patients with serum creatinine >1.3mg/dL were excluded. Creatinine clearance was calculated from a 24-hour urine collection. Patients were grouped according to the presence of augmented renal clearance (creatinine clearance >120mL/min/1.73m2), and possible risk factors were analyzed with bivariate and logistic regression analysis. In patients treated with vancomycin, dosage and plasma concentrations were registered.
Results:
Augmented renal clearance was present in 103 patients (28%); they were younger (48±15 versus 65±17 years, p<0.0001), had more frequent obstetric (16 versus 7%, p=0.0006) and trauma admissions (10 versus 3%, p=0.016) and fewer comorbidities. The only independent determinants for the development of augmented renal clearance were age (OR 0.95; p<0.0001; 95%CI 0.93-0.96) and absence of diabetes (OR 0.34; p=0.03; 95%CI 0.12-0.92). Twelve of the 46 patients who received vancomycin had augmented renal clearance and despite higher doses, had lower concentrations.
Conclusions:
In this cohort of critically ill patients, augmented renal clearance was a common finding. Age and absence of diabetes were the only independent determinants. Therefore, younger and previously healthy patients might require larger vancomycin dosing.
Keywords:CreatinineMetabolic clearance rateSepsis/drug therapyVancomycin/pharmacokineticsVancomycin/therapeutic useSee moreViews8Abstract
Original ArticlesAugmented renal clearance in critically ill patients: incidence, associated factors and effects on vancomycin treatment
Rev Bras Ter Intensiva. 2014;26(1):13-20
DOI 10.5935/0103-507X.20140003
Views8Objective:
An augmented renal clearance has been described in some groups of critically ill patients, and it might induce sub-optimal concentrations of drugs eliminated by glomerular filtration, mainly antibiotics. Studies on its occurrence and determinants are lacking. Our goals were to determine the incidence and associated factors of augmented renal clearance and the effects on vancomycin concentrations and dosing in a series of intensive care unit patients.
Methods:
We prospectively studied 363 patients admitted during 1 year to a clinical-surgical intensive care unit. Patients with serum creatinine >1.3mg/dL were excluded. Creatinine clearance was calculated from a 24-hour urine collection. Patients were grouped according to the presence of augmented renal clearance (creatinine clearance >120mL/min/1.73m2), and possible risk factors were analyzed with bivariate and logistic regression analysis. In patients treated with vancomycin, dosage and plasma concentrations were registered.
Results:
Augmented renal clearance was present in 103 patients (28%); they were younger (48±15 versus 65±17 years, p<0.0001), had more frequent obstetric (16 versus 7%, p=0.0006) and trauma admissions (10 versus 3%, p=0.016) and fewer comorbidities. The only independent determinants for the development of augmented renal clearance were age (OR 0.95; p<0.0001; 95%CI 0.93-0.96) and absence of diabetes (OR 0.34; p=0.03; 95%CI 0.12-0.92). Twelve of the 46 patients who received vancomycin had augmented renal clearance and despite higher doses, had lower concentrations.
Conclusions:
In this cohort of critically ill patients, augmented renal clearance was a common finding. Age and absence of diabetes were the only independent determinants. Therefore, younger and previously healthy patients might require larger vancomycin dosing.
Keywords:CreatinineMetabolic clearance rateSepsis/drug therapyVancomycin/pharmacokineticsVancomycin/therapeutic useSee more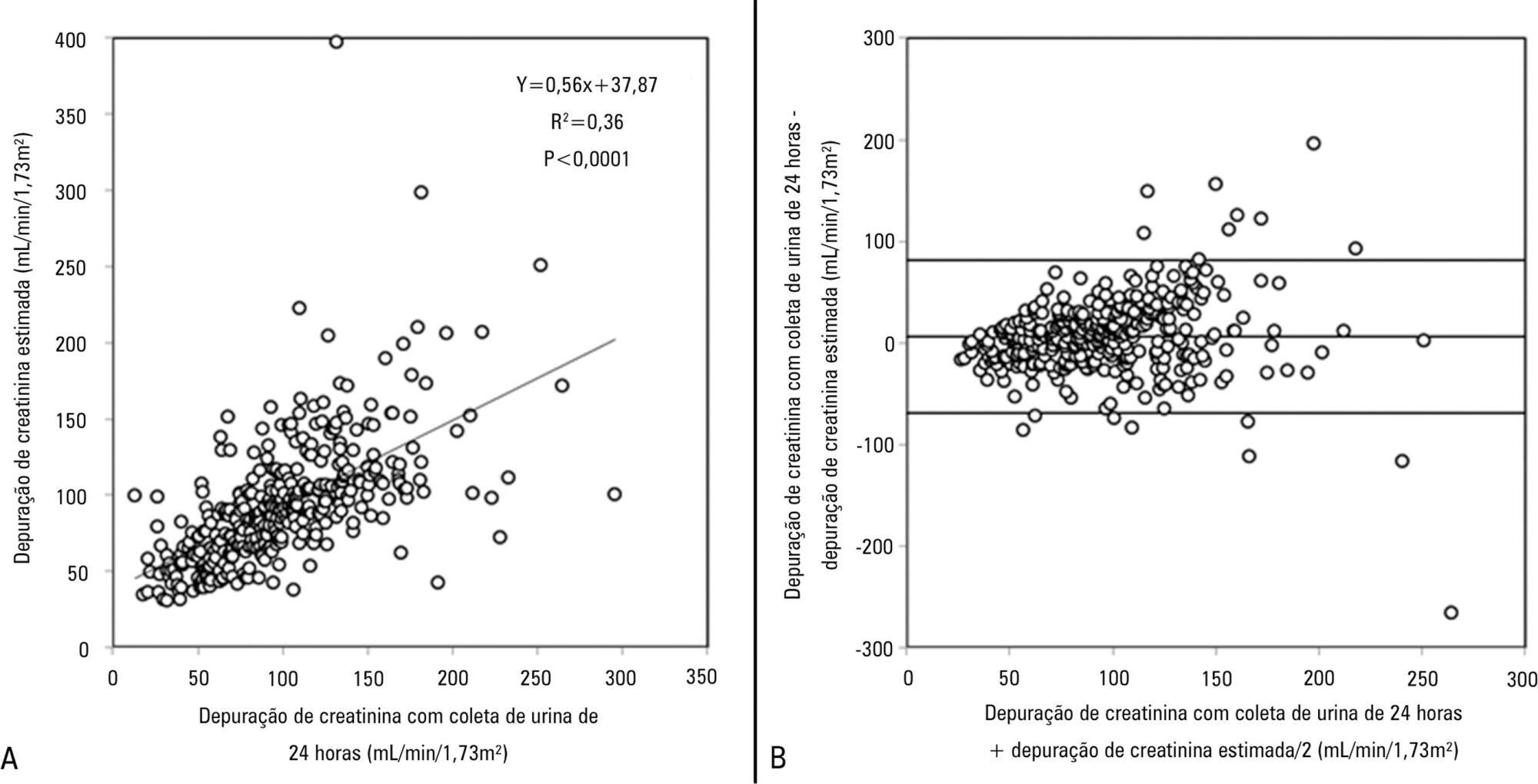
-
Original Articles
Urinary strong ion difference is a major determinant of plasma chloride concentration changes in postoperative patients
Rev Bras Ter Intensiva. 2013;25(3):197-204
Abstract
Original ArticlesUrinary strong ion difference is a major determinant of plasma chloride concentration changes in postoperative patients
Rev Bras Ter Intensiva. 2013;25(3):197-204
DOI 10.5935/0103-507X.20130035
Views1See moreOBJECTIVE:
To show that alterations in the plasma chloride concentration ([Cl–]plasma) during the postoperative period are largely dependent on the urinary strong ion difference ([SID]urine=[Na+]urine+[K+]urine-[Cl-]urine) and not on differences in fluid therapy.
METHODS:
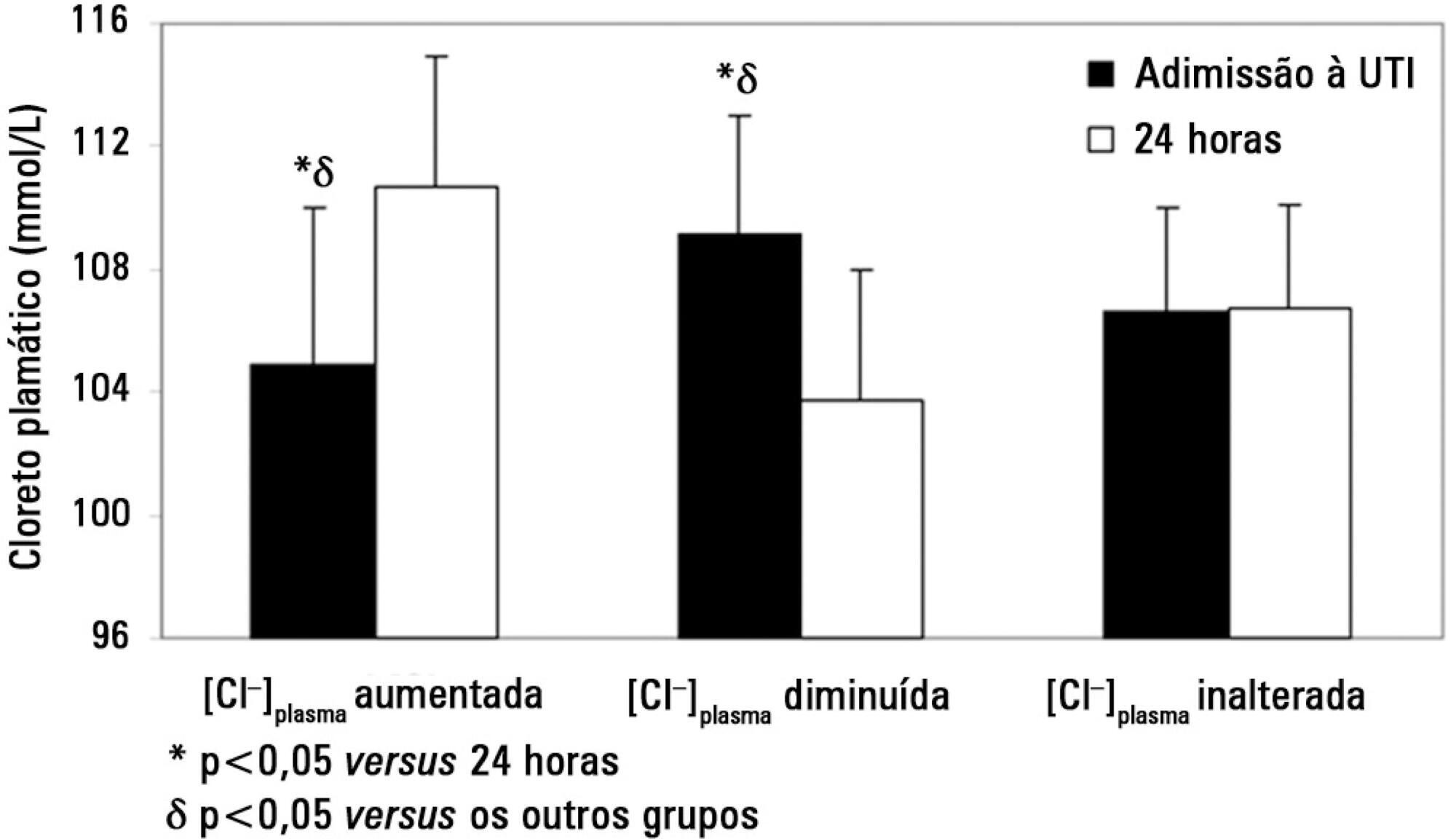
Measurements were performed at intensive care unit admission and 24 hours later in a total of 148 postoperative patients. Patients were assigned into one of three groups according to the change in [Cl–]plasma at the 24 hours time point: increased [Cl–]plasma (n=39), decreased [Cl–]plasma (n=56) or unchanged [Cl–]plasma (n=53).
RESULTS:
On admission, the increased [Cl–]plasma group had a lower [Cl–]plasma (105±5 versus 109±4 and 106±3mmol/L, p<0.05), a higher plasma anion gap concentration ([AG]plasma) and a higher strong ion gap concentration ([SIG]). After 24 hours, the increased [Cl–]plasma group showed a higher [Cl–]plasma (111±4 versus 104±4 and 107±3mmol/L, p<0.05) and lower [AG]plasma and [SIG]. The volume and [SID] of administered fluids were similar between groups except that the [SID]urine was higher (38±37 versus 18±22 and 23±18mmol/L, p<0.05) in the increased [Cl–]plasma group at the 24 hours time point. A multiple linear regression analysis showed that the [Cl–]plasma on admission and [SID]urine were independent predictors of the variation in [Cl–]plasma 24 hours later.
CONCLUSIONS:
Changes in [Cl–]plasma during the first postoperative day were largely related to [SID]urine and [Cl–]plasma on admission and not to the characteristics of the infused fluids. Therefore, decreasing [SID]urine could be a major mechanism for preventing the development of salineinduced hyperchloremia.
Views1Abstract
Original ArticlesUrinary strong ion difference is a major determinant of plasma chloride concentration changes in postoperative patients
Rev Bras Ter Intensiva. 2013;25(3):197-204
DOI 10.5935/0103-507X.20130035
Views1See moreOBJECTIVE:
To show that alterations in the plasma chloride concentration ([Cl–]plasma) during the postoperative period are largely dependent on the urinary strong ion difference ([SID]urine=[Na+]urine+[K+]urine-[Cl-]urine) and not on differences in fluid therapy.
METHODS:
Measurements were performed at intensive care unit admission and 24 hours later in a total of 148 postoperative patients. Patients were assigned into one of three groups according to the change in [Cl–]plasma at the 24 hours time point: increased [Cl–]plasma (n=39), decreased [Cl–]plasma (n=56) or unchanged [Cl–]plasma (n=53).
RESULTS:
On admission, the increased [Cl–]plasma group had a lower [Cl–]plasma (105±5 versus 109±4 and 106±3mmol/L, p<0.05), a higher plasma anion gap concentration ([AG]plasma) and a higher strong ion gap concentration ([SIG]). After 24 hours, the increased [Cl–]plasma group showed a higher [Cl–]plasma (111±4 versus 104±4 and 107±3mmol/L, p<0.05) and lower [AG]plasma and [SIG]. The volume and [SID] of administered fluids were similar between groups except that the [SID]urine was higher (38±37 versus 18±22 and 23±18mmol/L, p<0.05) in the increased [Cl–]plasma group at the 24 hours time point. A multiple linear regression analysis showed that the [Cl–]plasma on admission and [SID]urine were independent predictors of the variation in [Cl–]plasma 24 hours later.
CONCLUSIONS:
Changes in [Cl–]plasma during the first postoperative day were largely related to [SID]urine and [Cl–]plasma on admission and not to the characteristics of the infused fluids. Therefore, decreasing [SID]urine could be a major mechanism for preventing the development of salineinduced hyperchloremia.
-
Fluids in the postoperative period: effects of lack of adjustment to body weight
Rev Bras Ter Intensiva. 2011;23(2):170-175
Abstract
Fluids in the postoperative period: effects of lack of adjustment to body weight
Rev Bras Ter Intensiva. 2011;23(2):170-175
DOI 10.1590/S0103-507X2011000200009
Views0See moreOBJECTIVE: To compare the differences in fluid and electrolyte balance in patients with low and high weight in the first postoperative day. METHODS: Over a period of 18 months, we prospectively evaluated 150 patients in the first 24 hours after surgery, in a university-affiliated hospital intensive care unit. Patients with low weight (< 60 kg) and high body weight (> 90 Kg) were compared in terms of fluid intake and output. RESULTS: No significant differences were observed in the volume (4334 ± 1097 vs. 4644 ± 1957 ml/24 h) and composition of the fluids administered (481 ± 187 vs. 586 ± 288 mEq [Na+]administered/24 h). The 24 h urine output was similar (2474 ± 1597 vs.2208 ± 678 ml/24 h) but low weight group showed higher electrolyte elimination (296 ± 195 vs.192 ± 117 mEq [Na+]urine /24 h, p = 0.0246). When the administered fluids were adjusted for body weight, the volume and amount of electrolytes of fluids administered were higher in the low weight group (79 ± 21 vs. 47 ± 22 ml/kg/24 h, p < 0.0001 and 8.8 ± 3.4 vs. 5.8 ± 3.3 mEq [Na+]administered/kg/24 h, p = 0.017, respectively). This group also showed higher urine output and electrolyte elimination (45 ± 28 vs. 22 ± 7 ml/kg/24 h, p = 0.0002 and 5.3 ± 3.5 vs. 1.8 ± 1.2 mEq [Na+]urine/kg/24 h, p < 0.0001, respectively). CONCLUSIONS: The lack of adjustment of the fluid therapy to body weight determined that low weight patients received more fluid than high weight patients according to their body weight. This fluid overload could be compensated by increased urine output and electrolyte elimination.
Views0Abstract
Fluids in the postoperative period: effects of lack of adjustment to body weight
Rev Bras Ter Intensiva. 2011;23(2):170-175
DOI 10.1590/S0103-507X2011000200009
Views0See moreOBJECTIVE: To compare the differences in fluid and electrolyte balance in patients with low and high weight in the first postoperative day. METHODS: Over a period of 18 months, we prospectively evaluated 150 patients in the first 24 hours after surgery, in a university-affiliated hospital intensive care unit. Patients with low weight (< 60 kg) and high body weight (> 90 Kg) were compared in terms of fluid intake and output. RESULTS: No significant differences were observed in the volume (4334 ± 1097 vs. 4644 ± 1957 ml/24 h) and composition of the fluids administered (481 ± 187 vs. 586 ± 288 mEq [Na+]administered/24 h). The 24 h urine output was similar (2474 ± 1597 vs.2208 ± 678 ml/24 h) but low weight group showed higher electrolyte elimination (296 ± 195 vs.192 ± 117 mEq [Na+]urine /24 h, p = 0.0246). When the administered fluids were adjusted for body weight, the volume and amount of electrolytes of fluids administered were higher in the low weight group (79 ± 21 vs. 47 ± 22 ml/kg/24 h, p < 0.0001 and 8.8 ± 3.4 vs. 5.8 ± 3.3 mEq [Na+]administered/kg/24 h, p = 0.017, respectively). This group also showed higher urine output and electrolyte elimination (45 ± 28 vs. 22 ± 7 ml/kg/24 h, p = 0.0002 and 5.3 ± 3.5 vs. 1.8 ± 1.2 mEq [Na+]urine/kg/24 h, p < 0.0001, respectively). CONCLUSIONS: The lack of adjustment of the fluid therapy to body weight determined that low weight patients received more fluid than high weight patients according to their body weight. This fluid overload could be compensated by increased urine output and electrolyte elimination.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness ICU Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis