Subarachnoid hemorrhage Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(3):311-319
DOI 10.5935/2965-2774.20230119-es
To determine the prevalence of sonographic vasospasm and delayed ischemic deficit in patients with aneurysmal subarachnoid hemorrhage, to evaluate the correlation between different tomographic scales and these complications, and to study prognostic factors in this group of patients.
This was a prospective study of patients admitted to the intensive care unit with a diagnosis of aneurysmal subarachnoid hemorrhage. The prevalence of sonographic vasospasm and radiological delayed cerebral ischemia was analyzed, as was the correlation between different tomographic scales and these complications.
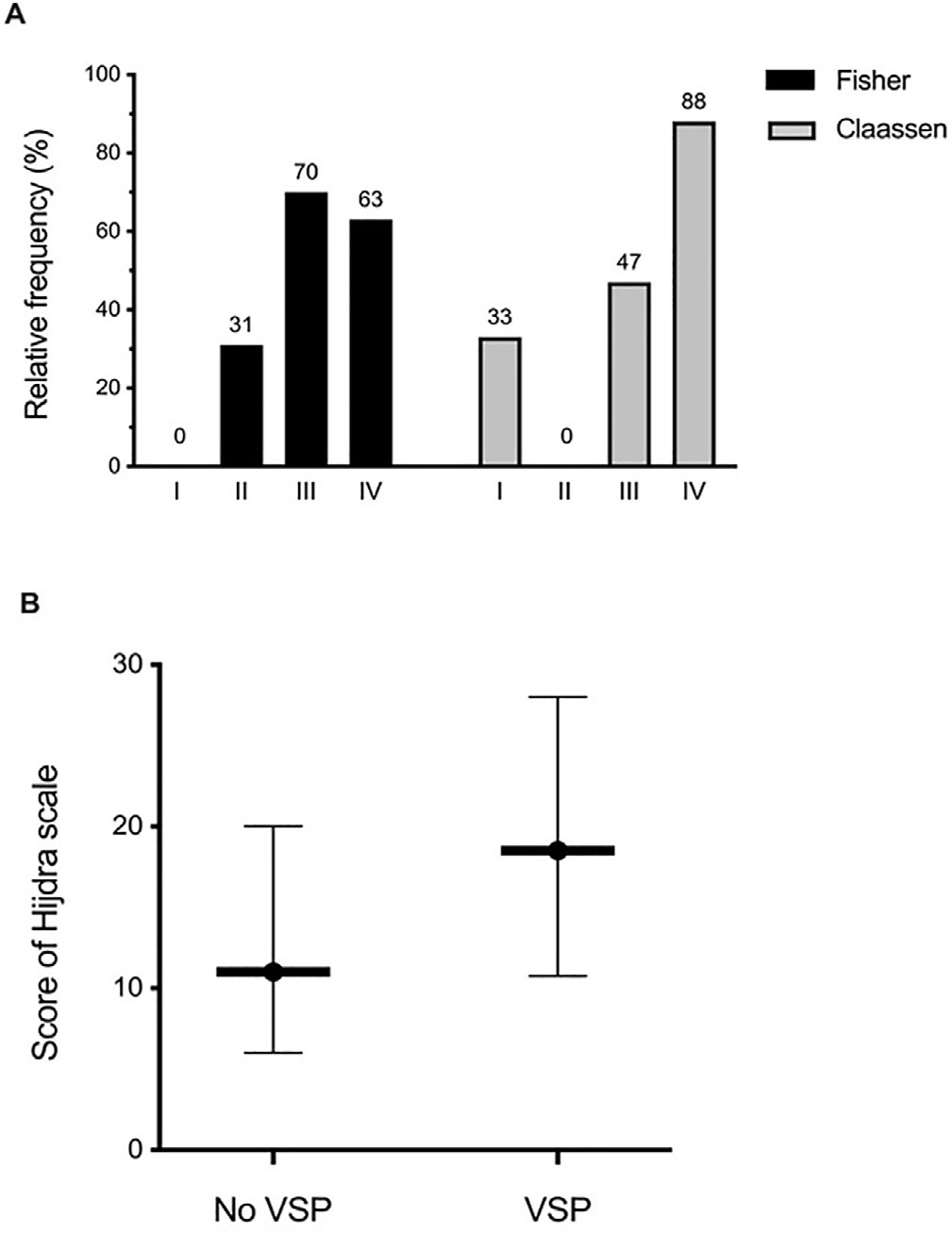
A total of 57 patients were studied. Sixty percent of the patients developed sonographic vasospasm, which was significantly associated with delayed cerebral ischemia and mortality. The Claassen and Hijdra scales were better correlated with the development of cerebral vasospasm (areas under the curve of 0.78 and 0.68) than was Fisher’s scale (0.62). Thirty-two patients (56.1%) developed cerebral infarction on CT; the significantly associated factors were poor clinical grade at admission (p = 0.04), sonographic vasospasm (p = 0.008) and severity of vasospasm (p = 0.015). Only the semiquantitative Hijdra scale was significantly correlated with the development of radiological delayed cerebral ischemia (p = 0.009). The patients who presented cerebral infarction had worse neurological evolution and higher mortality.
This is the first study in our environment on the subject. The Claassen and Hijdra tomographic scales showed better prognostic performance than the Fisher scale for the development of cerebral vasospasm. The finding of sonographic vasospasm could be a noninvasive criterion for the early detection of delayed cerebral ischemia and neurological deterioration in patients with aneurysmal subarachnoid hemorrhage.
Abstract
Crit Care Sci. 2023;35(3):311-319
DOI 10.5935/2965-2774.20230119-es
To determine the prevalence of sonographic vasospasm and delayed ischemic deficit in patients with aneurysmal subarachnoid hemorrhage, to evaluate the correlation between different tomographic scales and these complications, and to study prognostic factors in this group of patients.
This was a prospective study of patients admitted to the intensive care unit with a diagnosis of aneurysmal subarachnoid hemorrhage. The prevalence of sonographic vasospasm and radiological delayed cerebral ischemia was analyzed, as was the correlation between different tomographic scales and these complications.
A total of 57 patients were studied. Sixty percent of the patients developed sonographic vasospasm, which was significantly associated with delayed cerebral ischemia and mortality. The Claassen and Hijdra scales were better correlated with the development of cerebral vasospasm (areas under the curve of 0.78 and 0.68) than was Fisher’s scale (0.62). Thirty-two patients (56.1%) developed cerebral infarction on CT; the significantly associated factors were poor clinical grade at admission (p = 0.04), sonographic vasospasm (p = 0.008) and severity of vasospasm (p = 0.015). Only the semiquantitative Hijdra scale was significantly correlated with the development of radiological delayed cerebral ischemia (p = 0.009). The patients who presented cerebral infarction had worse neurological evolution and higher mortality.
This is the first study in our environment on the subject. The Claassen and Hijdra tomographic scales showed better prognostic performance than the Fisher scale for the development of cerebral vasospasm. The finding of sonographic vasospasm could be a noninvasive criterion for the early detection of delayed cerebral ischemia and neurological deterioration in patients with aneurysmal subarachnoid hemorrhage.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):197-201
Abstract
Rev Bras Ter Intensiva. 2022;34(1):197-201
Abstract
Rev Bras Ter Intensiva. 2020;32(4):592-602
DOI 10.5935/0103-507X.20200097
To systematically review the current evidence on the efficacy of milrinone in the treatment of cerebral vasospasm after subarachnoid hemorrhage.
The Pubmed®, Cochrane and Embase databases were screened for articles published from April 2001 to February 2019. Two independent reviewers performed the methodological quality screening and data extraction of the studies.
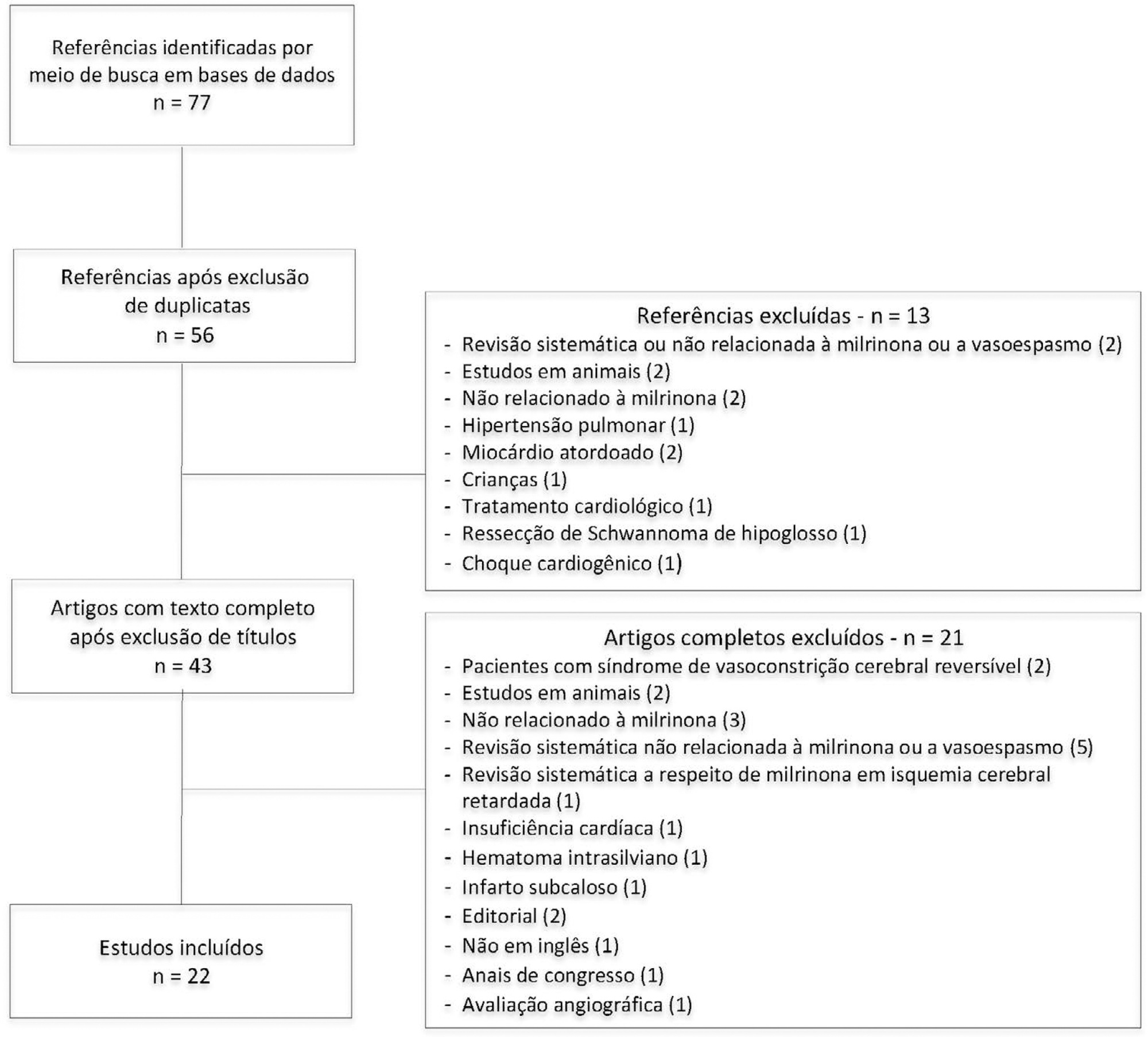
Twenty-two studies were found to be relevant, and only one of these was a randomized control trial. Studies showed marked heterogeneity and weaknesses in key methodological criteria. Most patients presented with moderate to severe vasospasm. Angiography was the main method of diagnosing vasospasm. Intra-arterial administration of milrinone was performed in three studies, intravenous administration was performed in nine studies, and both routes of administration in six studies; the intrathecal route was used in two studies, the cisternal route in one study and endovascular administration in one study. The side effects of milrinone were described in six studies. Twenty-one studies indicated resolution of vasospasm.
The current evidence indicates that milrinone may have a role in treatment of vasospasm after aneurysmal subarachnoid hemorrhage. However, only one randomized control trial was performed, with a low quality level. Our findings indicate the need for future randomized control trials with patient-centered outcomes to provide definitive recommendations.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):592-602
DOI 10.5935/0103-507X.20200097
To systematically review the current evidence on the efficacy of milrinone in the treatment of cerebral vasospasm after subarachnoid hemorrhage.
The Pubmed®, Cochrane and Embase databases were screened for articles published from April 2001 to February 2019. Two independent reviewers performed the methodological quality screening and data extraction of the studies.
Twenty-two studies were found to be relevant, and only one of these was a randomized control trial. Studies showed marked heterogeneity and weaknesses in key methodological criteria. Most patients presented with moderate to severe vasospasm. Angiography was the main method of diagnosing vasospasm. Intra-arterial administration of milrinone was performed in three studies, intravenous administration was performed in nine studies, and both routes of administration in six studies; the intrathecal route was used in two studies, the cisternal route in one study and endovascular administration in one study. The side effects of milrinone were described in six studies. Twenty-one studies indicated resolution of vasospasm.
The current evidence indicates that milrinone may have a role in treatment of vasospasm after aneurysmal subarachnoid hemorrhage. However, only one randomized control trial was performed, with a low quality level. Our findings indicate the need for future randomized control trials with patient-centered outcomes to provide definitive recommendations.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):21-27
DOI 10.5935/0103-507X.20180003
To evaluate the relationships of brain iron and heme with the inflammatory response of the systemic and central nervous systems and to investigate the role of defensive systems against the toxicity of iron and heme in the central nervous system.
We assessed a prospective cohort of patients presenting with intracerebral and subarachnoid hemorrhage. We assayed plasma and cerebrospinal fluid samples for the presence of iron, heme, hemopexin, haptoglobin, enolase, S100-β and cytokines for the first three days following hemorrhagic stroke. We also analyzed the dynamic changes in these components within both fluids and their relationship with early mortality rates.
Hemopexin and haptoglobin concentrations were nearly negligible in the brain after intracerebral and subarachnoid hemorrhage. Cerebrospinal fluid iron and heme concentrations correlated with a pro-inflammatory response in the central nervous system, and plasmatic and cerebrospinal fluid inflammatory profiles on the third day after hemorrhagic stroke were related to early mortality rates. Interleukin 4 levels within the cerebrospinal fluid during the first 24 hours after hemorrhagic stroke were found to be higher in survivors than in non-survivors.
Iron and heme are associated with a pro-inflammatory response in the central nervous system following hemorrhagic stroke, and protections against hemoglobin and heme are lacking within the human brain. Patient inflammatory profiles were associated with a poorer prognosis, and local anti-inflammatory responses appeared to have a protective role.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):21-27
DOI 10.5935/0103-507X.20180003
To evaluate the relationships of brain iron and heme with the inflammatory response of the systemic and central nervous systems and to investigate the role of defensive systems against the toxicity of iron and heme in the central nervous system.
We assessed a prospective cohort of patients presenting with intracerebral and subarachnoid hemorrhage. We assayed plasma and cerebrospinal fluid samples for the presence of iron, heme, hemopexin, haptoglobin, enolase, S100-β and cytokines for the first three days following hemorrhagic stroke. We also analyzed the dynamic changes in these components within both fluids and their relationship with early mortality rates.
Hemopexin and haptoglobin concentrations were nearly negligible in the brain after intracerebral and subarachnoid hemorrhage. Cerebrospinal fluid iron and heme concentrations correlated with a pro-inflammatory response in the central nervous system, and plasmatic and cerebrospinal fluid inflammatory profiles on the third day after hemorrhagic stroke were related to early mortality rates. Interleukin 4 levels within the cerebrospinal fluid during the first 24 hours after hemorrhagic stroke were found to be higher in survivors than in non-survivors.
Iron and heme are associated with a pro-inflammatory response in the central nervous system following hemorrhagic stroke, and protections against hemoglobin and heme are lacking within the human brain. Patient inflammatory profiles were associated with a poorer prognosis, and local anti-inflammatory responses appeared to have a protective role.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):141-146
DOI 10.5935/0103-507X.20160028
To compare the clinical evolution of perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage.
The study was conducted retrospectively in a tertiary hospital center in the north region of Portugal. Included patients had no identifiable cause for subarachnoid hemorrhage. Several epidemiologic, clinical and imaging aspects were statistically analyzed, taking into account the differences in perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage.
Sixty-two patients met the inclusion criteria (46.8% - perimesencephalic subarachnoid hemorrhage; 53.2% - non-perimesencephalic subarachnoid hemorrhage). Demographic and clinical background characteristics were similar in both groups. Complications were more frequent in patients with non-perimesencephalic subarachnoid hemorrhage - 84.8% of the patients had at least one complication versus 48.3% in perimesencephalic subarachnoid hemorrhage. Vasospasm, infection and hydrocephaly were the most common complications (each was detected more frequently in the non-perimesencephalic subarachnoid hemorrhage group than in perimesencephalic subarachnoid hemorrhage group). Two patients died, both had a non-perimesencephalic subarachnoid hemorrhage. The median inpatient time was longer in the non-perimesencephalic subarachnoid hemorrhage group (21 versus 14 days). No incidents of rebleeding were reported during the follow-up period (mean time of 15 ± 10.3 months).
Perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage are two different entities that have different clinical outcomes, namely in terms of complication rate and median inpatient time. The management of these patients should respect this difference to improve treatment and optimize health care resources.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):141-146
DOI 10.5935/0103-507X.20160028
To compare the clinical evolution of perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage.
The study was conducted retrospectively in a tertiary hospital center in the north region of Portugal. Included patients had no identifiable cause for subarachnoid hemorrhage. Several epidemiologic, clinical and imaging aspects were statistically analyzed, taking into account the differences in perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage.
Sixty-two patients met the inclusion criteria (46.8% - perimesencephalic subarachnoid hemorrhage; 53.2% - non-perimesencephalic subarachnoid hemorrhage). Demographic and clinical background characteristics were similar in both groups. Complications were more frequent in patients with non-perimesencephalic subarachnoid hemorrhage - 84.8% of the patients had at least one complication versus 48.3% in perimesencephalic subarachnoid hemorrhage. Vasospasm, infection and hydrocephaly were the most common complications (each was detected more frequently in the non-perimesencephalic subarachnoid hemorrhage group than in perimesencephalic subarachnoid hemorrhage group). Two patients died, both had a non-perimesencephalic subarachnoid hemorrhage. The median inpatient time was longer in the non-perimesencephalic subarachnoid hemorrhage group (21 versus 14 days). No incidents of rebleeding were reported during the follow-up period (mean time of 15 ± 10.3 months).
Perimesencephalic subarachnoid hemorrhage and non-perimesencephalic subarachnoid hemorrhage are two different entities that have different clinical outcomes, namely in terms of complication rate and median inpatient time. The management of these patients should respect this difference to improve treatment and optimize health care resources.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):310-314
DOI 10.1590/S0103-507X2010000300015
Systemic complications are frequent in subarachnoid hemorrhage patients. Among these complications, electrocardiographic abnormalities simulating ischemic cardiomyopathy may occur, possibly associated with myocardial dysfunction. This manuscript aims to report a case of subarachnoid hemorrhage associated with myocardial dysfunction and cardiogenic shock. A 45 years old woman was admitted with subarachnoid hemorrhage and coma, showing Glasgow scale = 7, Hunt-Hess = 5 and Fischer computed tomography classification = 3. On the second day, the patient underwent anterior cerebral communicant artery aneurysm embolization. The clinical evaluation revealed diffuse pulmonary infiltration, dyspnea and hypotension. Additional tests showed electrocardiographic lateral wall repolarization changes and elevated creatine kinase-MB fraction (36U/L). The cardiac index was 2.03 L/minute/m², Vascular systemic resistance was 3728 dynes.sec/cm². The non-responsiveness to volume demonstrated a cardiogenic shock pattern. The ventricular ejection fraction was 39%. The coronariography was normal, showing no obstructive lesions. Six days later the patient was removed from respiratory support and after eight days the dobutamine infusion was discontinued. The ejection fraction recovered up to 65%. Serial transcranial Doppler evaluations did not show vascular spasm. After ten days the patient was discharged from the intensive care unit. Patients with subarachnoid hemorrhage may be complicated with ventricular dysfunction and cardiogenic shock, increasing the cerebral ischemia risk. Diagnosis optimization and hemodynamic stabilization are essential to minimize the risk of cerebral vasospasm and ischemia.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):310-314
DOI 10.1590/S0103-507X2010000300015
Systemic complications are frequent in subarachnoid hemorrhage patients. Among these complications, electrocardiographic abnormalities simulating ischemic cardiomyopathy may occur, possibly associated with myocardial dysfunction. This manuscript aims to report a case of subarachnoid hemorrhage associated with myocardial dysfunction and cardiogenic shock. A 45 years old woman was admitted with subarachnoid hemorrhage and coma, showing Glasgow scale = 7, Hunt-Hess = 5 and Fischer computed tomography classification = 3. On the second day, the patient underwent anterior cerebral communicant artery aneurysm embolization. The clinical evaluation revealed diffuse pulmonary infiltration, dyspnea and hypotension. Additional tests showed electrocardiographic lateral wall repolarization changes and elevated creatine kinase-MB fraction (36U/L). The cardiac index was 2.03 L/minute/m², Vascular systemic resistance was 3728 dynes.sec/cm². The non-responsiveness to volume demonstrated a cardiogenic shock pattern. The ventricular ejection fraction was 39%. The coronariography was normal, showing no obstructive lesions. Six days later the patient was removed from respiratory support and after eight days the dobutamine infusion was discontinued. The ejection fraction recovered up to 65%. Serial transcranial Doppler evaluations did not show vascular spasm. After ten days the patient was discharged from the intensive care unit. Patients with subarachnoid hemorrhage may be complicated with ventricular dysfunction and cardiogenic shock, increasing the cerebral ischemia risk. Diagnosis optimization and hemodynamic stabilization are essential to minimize the risk of cerebral vasospasm and ischemia.
