Mortality Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2010;22(4):327-332
DOI 10.1590/S0103-507X2010000400003
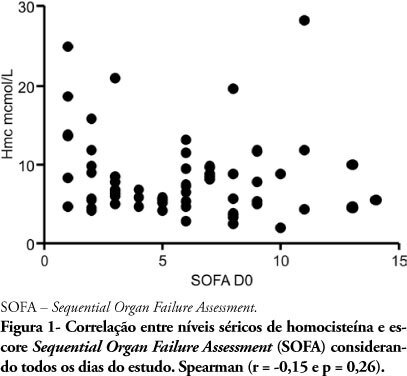
OBJECTIVE: Homocysteine and sepsis are both associated with inflammation and endothelial activation. Therefore this study was aimed to evaluate if the plasma homocystein level is related with the septic patient clinical severity. METHODS: Severe sepsis or septic shock patients, with less than 48 hours from organ dysfunction start, were admitted to this prospective observational study. Homocysteine levels were determined by the time of study admission and then on the Days 3, 7 and 14. The homocysteine association with the Sequential Organ Failure Assessment (SOFA) score was evaluated using the Sperman test, and its association with mortality using the Mann-Whitney test. A p<0.05 value was considered statistically significant. RESULTS: Twenty one patients were enrolled, and 60 blood samples were collected to measure total homocysteine [median 6.92 (5.27 - 9.74 μmol/L)]. The Sperman correlation test showed no association between homocysteine and SOFA ( r=0.15 and p=0.26). Also no correlation was found for the homocysteine level by the study admission time and the difference between the Day 3 SOFA score versus by study admission (deltaSOFA) (r=0.04 and p=0.87). Homocysteine variation between the Day 3 and the study admission (deltaHmc) and SOFA score variation in the same period were not correlated (r=-0.11 and p=0.66). Homocysteine by the study admission was not correlated with death in intensive care unit rate (p= 0.46) or in-hospital death rate (p = 0.13). This was also true for deltaHmc (p=0.12 and p=0.99, respectively). CONCLUSION: Baseline homocysteine levels and its variations within the first dysfunction days were not related with septic patients' worsened organ function parameters or mortality.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):327-332
DOI 10.1590/S0103-507X2010000400003
OBJECTIVE: Homocysteine and sepsis are both associated with inflammation and endothelial activation. Therefore this study was aimed to evaluate if the plasma homocystein level is related with the septic patient clinical severity. METHODS: Severe sepsis or septic shock patients, with less than 48 hours from organ dysfunction start, were admitted to this prospective observational study. Homocysteine levels were determined by the time of study admission and then on the Days 3, 7 and 14. The homocysteine association with the Sequential Organ Failure Assessment (SOFA) score was evaluated using the Sperman test, and its association with mortality using the Mann-Whitney test. A p<0.05 value was considered statistically significant. RESULTS: Twenty one patients were enrolled, and 60 blood samples were collected to measure total homocysteine [median 6.92 (5.27 - 9.74 μmol/L)]. The Sperman correlation test showed no association between homocysteine and SOFA ( r=0.15 and p=0.26). Also no correlation was found for the homocysteine level by the study admission time and the difference between the Day 3 SOFA score versus by study admission (deltaSOFA) (r=0.04 and p=0.87). Homocysteine variation between the Day 3 and the study admission (deltaHmc) and SOFA score variation in the same period were not correlated (r=-0.11 and p=0.66). Homocysteine by the study admission was not correlated with death in intensive care unit rate (p= 0.46) or in-hospital death rate (p = 0.13). This was also true for deltaHmc (p=0.12 and p=0.99, respectively). CONCLUSION: Baseline homocysteine levels and its variations within the first dysfunction days were not related with septic patients' worsened organ function parameters or mortality.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):220-228
DOI 10.1590/S0103-507X2010000300002
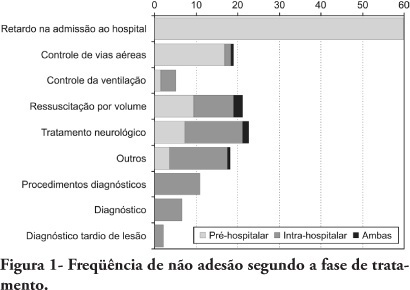
OBJECTIVES: To evaluate patients treated for traumatic injuries and to identify adherence to guidelines recommendations of treatment and association with death. The recommendations adopted were defined by the committee on trauma of the American College of Surgeons in advanced trauma life support. METHODS: Retrospective cohort study conducted at a teaching hospital. The study population was victims of trauma > 12 years of age with injury severity scores > 16 who were treated between January 1997 and December 2001. Data collection was divided into three phases: pre-hospital, in-hospital, and post-mortem. The data collected were analyzed using EPI INFO. RESULTS: We analyzed 207 patients, 147 blunt trauma victims (71%) and 60 (29%) penetrating trauma victims. Trauma victims had a 40.1% mortality rate. We identified 221 non adherence events that occurred in 137 patients. We found a mean of 1.61 non adherence per patient, and it occurred less frequently in survivors (1.4) than in non-survivors (1.9; p=0.033). According to the trauma score and injury severity score methodology, 54.2% of deaths were considered potentially preventable. Non adherence occurred 1.77 times more frequently in those considered potentially preventable deaths compared to other non-survivors (95% CI: 1.12-2.77; p=0.012), and 92.9% of the multiple non adherence occurred in the first group (p=0.029). CONCLUSIONS: Non adherence occurred more frequently in patients with potentially preventable deaths. Non adherence to guidelines recommendations can be considered a contributing factor to death in trauma victims and can lead to an increase in the number of potentially preventable deaths.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):220-228
DOI 10.1590/S0103-507X2010000300002
OBJECTIVES: To evaluate patients treated for traumatic injuries and to identify adherence to guidelines recommendations of treatment and association with death. The recommendations adopted were defined by the committee on trauma of the American College of Surgeons in advanced trauma life support. METHODS: Retrospective cohort study conducted at a teaching hospital. The study population was victims of trauma > 12 years of age with injury severity scores > 16 who were treated between January 1997 and December 2001. Data collection was divided into three phases: pre-hospital, in-hospital, and post-mortem. The data collected were analyzed using EPI INFO. RESULTS: We analyzed 207 patients, 147 blunt trauma victims (71%) and 60 (29%) penetrating trauma victims. Trauma victims had a 40.1% mortality rate. We identified 221 non adherence events that occurred in 137 patients. We found a mean of 1.61 non adherence per patient, and it occurred less frequently in survivors (1.4) than in non-survivors (1.9; p=0.033). According to the trauma score and injury severity score methodology, 54.2% of deaths were considered potentially preventable. Non adherence occurred 1.77 times more frequently in those considered potentially preventable deaths compared to other non-survivors (95% CI: 1.12-2.77; p=0.012), and 92.9% of the multiple non adherence occurred in the first group (p=0.029). CONCLUSIONS: Non adherence occurred more frequently in patients with potentially preventable deaths. Non adherence to guidelines recommendations can be considered a contributing factor to death in trauma victims and can lead to an increase in the number of potentially preventable deaths.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):236-244
DOI 10.1590/S0103-507X2010000300004
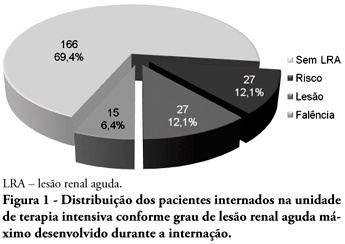
OBJECTIVES: Critically ill cancer patients are at increased risk for acute kidney injury, but studies on these patients are scarce and were all single centered conducted in specialized intensive care units. The objective was to evaluate the characteristics and outcomes in a prospective cohort of cancer patients admitted to several intensive care units with acute kidney injury. METHODS: Prospective multicenter cohort study conducted in intensive care units from 28 hospitals in Brazil over a two-month period. Univariate and multivariate logistic regression were used to identify factors associated with hospital mortality. RESULTS: Out of all 717 intensive care unit admissions, 87 (12%) had acute kidney injury and 36% of them received renal replacement therapy. Kidney injury developed more frequently in patients with hematological malignancies than in patients with solid tumors (26% vs. 11%, P=0.003). Ischemia/shock (76%) and sepsis (67%) were the main contributing factor for and kidney injury was multifactorial in 79% of the patients. Hospital mortality was 71%. General and renal-specific severity-of-illness scores were inaccurate in predicting outcomes for these patients. In a multivariate analysis, length of hospital stay prior to intensive care unit, acute organ dysfunctions, need for mechanical ventilation and a poor performance status were associated with increased mortality. Moreover, cancer-related characteristics were not associated with outcomes. CONCLUSIONS: The present study demonstrates that intensive care units admission and advanced life-support should be considered in selected critically ill cancer patients with kidney injury.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):236-244
DOI 10.1590/S0103-507X2010000300004
OBJECTIVES: Critically ill cancer patients are at increased risk for acute kidney injury, but studies on these patients are scarce and were all single centered conducted in specialized intensive care units. The objective was to evaluate the characteristics and outcomes in a prospective cohort of cancer patients admitted to several intensive care units with acute kidney injury. METHODS: Prospective multicenter cohort study conducted in intensive care units from 28 hospitals in Brazil over a two-month period. Univariate and multivariate logistic regression were used to identify factors associated with hospital mortality. RESULTS: Out of all 717 intensive care unit admissions, 87 (12%) had acute kidney injury and 36% of them received renal replacement therapy. Kidney injury developed more frequently in patients with hematological malignancies than in patients with solid tumors (26% vs. 11%, P=0.003). Ischemia/shock (76%) and sepsis (67%) were the main contributing factor for and kidney injury was multifactorial in 79% of the patients. Hospital mortality was 71%. General and renal-specific severity-of-illness scores were inaccurate in predicting outcomes for these patients. In a multivariate analysis, length of hospital stay prior to intensive care unit, acute organ dysfunctions, need for mechanical ventilation and a poor performance status were associated with increased mortality. Moreover, cancer-related characteristics were not associated with outcomes. CONCLUSIONS: The present study demonstrates that intensive care units admission and advanced life-support should be considered in selected critically ill cancer patients with kidney injury.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):250-256
DOI 10.1590/S0103-507X2010000300006
OBJECTIVE: The intensive care unit is synonymous of high severity, and its mortality rates are between 5.4 and 33%. With the development of new technologies, a patient can be maintained for long time in the unit, causing high costs, psychological and moral for all involved. This study aimed to evaluate the risk factors for mortality and prolonged length of stay in an adult intensive care unit. METHODS: The study included all patients consecutively admitted to the adult medical/surgical intensive care unit of Hospital das Clínicas da Universidade Estadual de Campinas, for six months. We collected data such as sex, age, diagnosis, personal history, APACHE II score, days of invasive mechanical ventilation orotracheal reintubation, tracheostomy, days of hospitalization in the intensive care unit and discharge or death in the intensive care unit. RESULTS: Were included in the study 401 patients; 59.6% men and 40.4% women, age 53.8±18.0. The mean intensive care unit stay was 8.2±10.8 days, with a mortality rate of 13.5%. Significant data for mortality and prolonged length of stay in intensive care unit (p <0.0001), were: APACHE II>11, OT-Re and tracheostomy. CONCLUSION: The mortality and prolonged length of stay in intensive care unit intensive care unit as risk factors were: APACHE>11, orotracheal reintubation and tracheostomy.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):250-256
DOI 10.1590/S0103-507X2010000300006
OBJECTIVE: The intensive care unit is synonymous of high severity, and its mortality rates are between 5.4 and 33%. With the development of new technologies, a patient can be maintained for long time in the unit, causing high costs, psychological and moral for all involved. This study aimed to evaluate the risk factors for mortality and prolonged length of stay in an adult intensive care unit. METHODS: The study included all patients consecutively admitted to the adult medical/surgical intensive care unit of Hospital das Clínicas da Universidade Estadual de Campinas, for six months. We collected data such as sex, age, diagnosis, personal history, APACHE II score, days of invasive mechanical ventilation orotracheal reintubation, tracheostomy, days of hospitalization in the intensive care unit and discharge or death in the intensive care unit. RESULTS: Were included in the study 401 patients; 59.6% men and 40.4% women, age 53.8±18.0. The mean intensive care unit stay was 8.2±10.8 days, with a mortality rate of 13.5%. Significant data for mortality and prolonged length of stay in intensive care unit (p <0.0001), were: APACHE II>11, OT-Re and tracheostomy. CONCLUSION: The mortality and prolonged length of stay in intensive care unit intensive care unit as risk factors were: APACHE>11, orotracheal reintubation and tracheostomy.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):166-174
DOI 10.1590/S0103-507X2010000200011
OBJECTIVES: Acute kidney injury is characterized by sudden and generally revertible renal function impairment involving inability to maintain homeostasis. In pediatrics, the main causes of acute kidney injury are sepsis, use of nephrotoxic drugs and renal ischemia in critically ill patients. The incidence of acute kidney injury in these patients ranges from 20 to 30%, resulting in increased morbid-mortality, a 40 to 90% rate. This study aimed to evaluate the incidence of acute kidney injury in intensive care unit patients, to categorize the severity of the acute kidney injury according to the Pediatric Risk, Injury, Failure, Loss, End-Stage (pRIFLE), examine the relationship between the acute kidney injury and severity using the Pediatric Index of Mortality (PIM) and to analyze outcome predictors. METHODS: A prospective study of the patients admitted to the intensive care unit of Hospital Infantil Joana de Gusmão - Florianópolis / SC - Brazil was conducted between July 2008 and January 2009. Were evaluated daily the urine output and serum creatinine, and the patients were categorized according to the pRIFLE criteria. RESULTS: During the follow-up period, 235 children were admitted. The incidence of acute kidney injury was 30.6%, and the maximal pRIFLE score during hospitalization was 12.1% for R, 12.1% for I and 6.4% for F. The mortality rate was 12.3%. The patients who developed acute kidney injury had a ten times bigger risk of death versus the not exposed patients. CONCLUSIONS: Acute kidney injury is frequent in critically ill patients. Early diagnosis and prompt and appropriate therapy for each clinical aspect may change this condition's course and severity, and reduce the patients' morbidity and mortality.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):166-174
DOI 10.1590/S0103-507X2010000200011
OBJECTIVES: Acute kidney injury is characterized by sudden and generally revertible renal function impairment involving inability to maintain homeostasis. In pediatrics, the main causes of acute kidney injury are sepsis, use of nephrotoxic drugs and renal ischemia in critically ill patients. The incidence of acute kidney injury in these patients ranges from 20 to 30%, resulting in increased morbid-mortality, a 40 to 90% rate. This study aimed to evaluate the incidence of acute kidney injury in intensive care unit patients, to categorize the severity of the acute kidney injury according to the Pediatric Risk, Injury, Failure, Loss, End-Stage (pRIFLE), examine the relationship between the acute kidney injury and severity using the Pediatric Index of Mortality (PIM) and to analyze outcome predictors. METHODS: A prospective study of the patients admitted to the intensive care unit of Hospital Infantil Joana de Gusmão - Florianópolis / SC - Brazil was conducted between July 2008 and January 2009. Were evaluated daily the urine output and serum creatinine, and the patients were categorized according to the pRIFLE criteria. RESULTS: During the follow-up period, 235 children were admitted. The incidence of acute kidney injury was 30.6%, and the maximal pRIFLE score during hospitalization was 12.1% for R, 12.1% for I and 6.4% for F. The mortality rate was 12.3%. The patients who developed acute kidney injury had a ten times bigger risk of death versus the not exposed patients. CONCLUSIONS: Acute kidney injury is frequent in critically ill patients. Early diagnosis and prompt and appropriate therapy for each clinical aspect may change this condition's course and severity, and reduce the patients' morbidity and mortality.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):112-117
DOI 10.1590/S0103-507X2010000200003
OBJECTIVES: Communication issues between healthcare professionals in intensive care units may be related to critically ill patients’ increased mortality. This study aimed to evaluate if communication issues involving assistant physicians and routine intensive care unit physicians would impact critically ill patients’ morbidity and mortality. METHODS: This was a cohort study that included non-consecutive patients admitted to the intensive care unit for 18 months. The patients were categorized in 3 groups according to their assistant doctors’ versus routine doctors communication uses: DC - daily communication during the stay (>75% of the days); EC - eventual communication (25 to 75% of the days); RC - rare communication (< 25% of the days). Demographic data, severity scores, reason for admission to the intensive care unit and interventions were recorded. The consequences of the medical professionals communication failures (delayed procedures, diagnostic tests, antibiotics, ventilatory weaning, vasopressors) and medical prescriptions inadequacies (no bed head elevation, no stress ulceration and deep venous thrombosis drug prophylaxis), and their relationship with the patients outcomes were analyzed. RESULTS: 792 patients were included, and categorized as follows: DC (n=529); EC (n=187) and RC (n=76). The mortality was increased in the RC patients group (26.3%) versus the remainder groups (DC = 13.6% and EC = 17.1%; p<0.05). A multivariate analysis showed that delayed antibiotics [RR 1.83 (CI95%: 1.36 -2.25)], delayed ventilatory weaning [RR 1.63 (CI95%: 1.25-2.04)] and no deep venous thrombosis prophylaxis [RR 1.98 (CI95%: 1.43 - 3.12)] contributed independently for the increased mortality. CONCLUSION: The failure in the assistant and routine intensive care doctors communication may increase the patients’ mortality, particularly due to delayed antibiotics and ventilation weaning, and lack of deep venous thrombosis prophylaxis prescription.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):112-117
DOI 10.1590/S0103-507X2010000200003
OBJECTIVES: Communication issues between healthcare professionals in intensive care units may be related to critically ill patients’ increased mortality. This study aimed to evaluate if communication issues involving assistant physicians and routine intensive care unit physicians would impact critically ill patients’ morbidity and mortality. METHODS: This was a cohort study that included non-consecutive patients admitted to the intensive care unit for 18 months. The patients were categorized in 3 groups according to their assistant doctors’ versus routine doctors communication uses: DC - daily communication during the stay (>75% of the days); EC - eventual communication (25 to 75% of the days); RC - rare communication (< 25% of the days). Demographic data, severity scores, reason for admission to the intensive care unit and interventions were recorded. The consequences of the medical professionals communication failures (delayed procedures, diagnostic tests, antibiotics, ventilatory weaning, vasopressors) and medical prescriptions inadequacies (no bed head elevation, no stress ulceration and deep venous thrombosis drug prophylaxis), and their relationship with the patients outcomes were analyzed. RESULTS: 792 patients were included, and categorized as follows: DC (n=529); EC (n=187) and RC (n=76). The mortality was increased in the RC patients group (26.3%) versus the remainder groups (DC = 13.6% and EC = 17.1%; p<0.05). A multivariate analysis showed that delayed antibiotics [RR 1.83 (CI95%: 1.36 -2.25)], delayed ventilatory weaning [RR 1.63 (CI95%: 1.25-2.04)] and no deep venous thrombosis prophylaxis [RR 1.98 (CI95%: 1.43 - 3.12)] contributed independently for the increased mortality. CONCLUSION: The failure in the assistant and routine intensive care doctors communication may increase the patients’ mortality, particularly due to delayed antibiotics and ventilation weaning, and lack of deep venous thrombosis prophylaxis prescription.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):133-137
DOI 10.1590/S0103-507X2010000200006
STUDY OBJECTIVE: Obese patients seem to have worse outcomes and more complications during intensive care unit (ICU) stay. This study describes the clinical course, complications and prognostic factors of obese patients admitted to an intensive care unit compared to a control group of nonobese patients. DESIGN: Retrospective observational study. SETTING: A 10-bed adult intensive care unit in a university-affiliated hospital. METHODS: All patients admitted to the intensive care unit over 52 months (April 01/2005 to November 30/2008) were included. Obese patients were defined as those with a body mass index (BMI) ≥ 30 Kg/M2. Demographic and intensive care unit related data were also collected. An clinical and demographical matching group of eutrophic patients selected from the data base as comparator for mortality and morbidity outcomes. The Mann-Whitney test was used for numeric data comparisons and the Chi Square test for categorical data comparisons. RESULTS: Two hundred nineteen patients were included. The obese group (n=73) was compared to the eutrophic group (n= 146). Most of this group BMI ranged between 30 - 35 Kg/M2. Only ten patients had body mass index ≥40 Kg/M2. Significant differences between the obese and eutrophic groups were observed in median APACHE II score (16 versus 12, respectively; p<0.05) and median intensive care unit length of stay (7 versus 5 days respectively; p<0,05). No significant differences were seen regarding risk of death, mortality rate, mechanical ventilation needs, days free of mechanical ventilation and tracheostomy rates. The observed mortality was higher than the APACHE II-predicted for both groups, but the larger differences were seen for morbid obese patients (BMI ≥40 Kg/M2). CONCLUSIONS: Obesity did not increase the mortality rate, but improved intensive care unit length of stay. The current prognostic scoring systems do not include BMI, possibly underestimating the risk of death, and other quality of care indexes in obese patients. New studies could be useful to clarify how body mass index impacts the mortality rate.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):133-137
DOI 10.1590/S0103-507X2010000200006
STUDY OBJECTIVE: Obese patients seem to have worse outcomes and more complications during intensive care unit (ICU) stay. This study describes the clinical course, complications and prognostic factors of obese patients admitted to an intensive care unit compared to a control group of nonobese patients. DESIGN: Retrospective observational study. SETTING: A 10-bed adult intensive care unit in a university-affiliated hospital. METHODS: All patients admitted to the intensive care unit over 52 months (April 01/2005 to November 30/2008) were included. Obese patients were defined as those with a body mass index (BMI) ≥ 30 Kg/M2. Demographic and intensive care unit related data were also collected. An clinical and demographical matching group of eutrophic patients selected from the data base as comparator for mortality and morbidity outcomes. The Mann-Whitney test was used for numeric data comparisons and the Chi Square test for categorical data comparisons. RESULTS: Two hundred nineteen patients were included. The obese group (n=73) was compared to the eutrophic group (n= 146). Most of this group BMI ranged between 30 - 35 Kg/M2. Only ten patients had body mass index ≥40 Kg/M2. Significant differences between the obese and eutrophic groups were observed in median APACHE II score (16 versus 12, respectively; p<0.05) and median intensive care unit length of stay (7 versus 5 days respectively; p<0,05). No significant differences were seen regarding risk of death, mortality rate, mechanical ventilation needs, days free of mechanical ventilation and tracheostomy rates. The observed mortality was higher than the APACHE II-predicted for both groups, but the larger differences were seen for morbid obese patients (BMI ≥40 Kg/M2). CONCLUSIONS: Obesity did not increase the mortality rate, but improved intensive care unit length of stay. The current prognostic scoring systems do not include BMI, possibly underestimating the risk of death, and other quality of care indexes in obese patients. New studies could be useful to clarify how body mass index impacts the mortality rate.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):138-143
DOI 10.1590/S0103-507X2010000200007
BACKGROUND: The elderly population is increasing all over the world. The need of intensive care by the elderly is also increasing. There is a lack of studies investigating the risk factors for death among critically ill elderly patients. This study aims to investigate the factors associated with death in a population of critically ill elderly patients admitted to an intensive care unit in Brazil. METHODS: This is a retrospective cohort study including all elderly patients (>60 years) admitted to an intensive care unit in Fortaleza, Brazil, from January to December 2007. A comparison between survivors and nonsurvivors was done and the risk factors for death were investigated through univariate and multivariate analysis. RESULTS: A total of 84 patients were included, with an average age of 73 ± 7.6 years; 59% were female. Mortality was 62.8%. The main cause of death was multiple organ dysfunction (42.3%), followed by septic shock (36.5%) and cardiogenic shock (9.7%). Complications during intensive care unit ICU stay associated with death were respiratory failure (OR=61, p<0.001), acute kidney injury (OR=23, p<0.001), sepsis (OR=12, p<0.001), metabolic acidosis (OR=17, p<0.001), anemia (OR=8.6, p<0.005), coagulation disturbance (OR=5.9, p<0.001) and atrial fibrillation (OR=4.8, p<0.041). Independent risk factors for death were age (OR=1.15, p<0.005), coma (OR=7.51, p<0.003), hypotension (OR=21.75, p=0.003), respiratory failure (OR=9.93, p<0.0001) and acute kidney injury (OR=16.28, p<0.014). CONCLUSION: Mortality is high among critically ill elderly patients. Factors associated with death were age, coma, hypotension, respiratory failure and acute kidney injury.
Abstract
Rev Bras Ter Intensiva. 2010;22(2):138-143
DOI 10.1590/S0103-507X2010000200007
BACKGROUND: The elderly population is increasing all over the world. The need of intensive care by the elderly is also increasing. There is a lack of studies investigating the risk factors for death among critically ill elderly patients. This study aims to investigate the factors associated with death in a population of critically ill elderly patients admitted to an intensive care unit in Brazil. METHODS: This is a retrospective cohort study including all elderly patients (>60 years) admitted to an intensive care unit in Fortaleza, Brazil, from January to December 2007. A comparison between survivors and nonsurvivors was done and the risk factors for death were investigated through univariate and multivariate analysis. RESULTS: A total of 84 patients were included, with an average age of 73 ± 7.6 years; 59% were female. Mortality was 62.8%. The main cause of death was multiple organ dysfunction (42.3%), followed by septic shock (36.5%) and cardiogenic shock (9.7%). Complications during intensive care unit ICU stay associated with death were respiratory failure (OR=61, p<0.001), acute kidney injury (OR=23, p<0.001), sepsis (OR=12, p<0.001), metabolic acidosis (OR=17, p<0.001), anemia (OR=8.6, p<0.005), coagulation disturbance (OR=5.9, p<0.001) and atrial fibrillation (OR=4.8, p<0.041). Independent risk factors for death were age (OR=1.15, p<0.005), coma (OR=7.51, p<0.003), hypotension (OR=21.75, p=0.003), respiratory failure (OR=9.93, p<0.0001) and acute kidney injury (OR=16.28, p<0.014). CONCLUSION: Mortality is high among critically ill elderly patients. Factors associated with death were age, coma, hypotension, respiratory failure and acute kidney injury.