Mortality Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2007;19(4):414-420
DOI 10.1590/S0103-507X2007000400002
BACKGROUND AND OBJECTIVES: To determine the prevalence of intensive care unit (ICU)-acquired infections and the risk factors for these infections, identify the predominant infecting organisms, and evaluate the relationship between ICU-acquired infection and mortality. METHODS: A 1-day point prevalence study. Sixteen ICU of the State of Rio Grande do Sul-Brazil, excluding coronary care and pediatric units. All patients < 12 yrs occupying an ICU bed over a 24-hour period. The 16 ICU provided 174 case reports. Main outcomes: rates of ICU-acquired infection, resistance patterns of microbiological isolates, and potential risks factors for ICU-acquired infection and death. RESULTS: A total of 122 patients (71%) was infected and 51 (29%) had ICU-acquired infection. Pneumonia (58.2%), lower tract respiratory infection (22.9%), urinary tract infection (18%) were the most frequents types of ICU infection. Most frequently microorganisms reported were staphylococcus aureus (42% [64% resistant to oxacilin]) and pseudomonas aeruginosa (31%). Six risk factors for ICU acquired infection were identified: urinary catheterization, central vascular line, tracheal intubation for prolonged time (> 4 days), chronic disease and increased length of ICU stay (> 30 days). The risks factors associated with death were age, APACHE II, organ dysfunction, and tracheal intubation with or without mechanical ventilation. CONCLUSIONS: ICU-acquired infection is common and often associated with microbiological isolates of resistant organisms. This study may serve as an epidemiological reference to help the discussion of regional infection control policies.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):414-420
DOI 10.1590/S0103-507X2007000400002
BACKGROUND AND OBJECTIVES: To determine the prevalence of intensive care unit (ICU)-acquired infections and the risk factors for these infections, identify the predominant infecting organisms, and evaluate the relationship between ICU-acquired infection and mortality. METHODS: A 1-day point prevalence study. Sixteen ICU of the State of Rio Grande do Sul-Brazil, excluding coronary care and pediatric units. All patients < 12 yrs occupying an ICU bed over a 24-hour period. The 16 ICU provided 174 case reports. Main outcomes: rates of ICU-acquired infection, resistance patterns of microbiological isolates, and potential risks factors for ICU-acquired infection and death. RESULTS: A total of 122 patients (71%) was infected and 51 (29%) had ICU-acquired infection. Pneumonia (58.2%), lower tract respiratory infection (22.9%), urinary tract infection (18%) were the most frequents types of ICU infection. Most frequently microorganisms reported were staphylococcus aureus (42% [64% resistant to oxacilin]) and pseudomonas aeruginosa (31%). Six risk factors for ICU acquired infection were identified: urinary catheterization, central vascular line, tracheal intubation for prolonged time (> 4 days), chronic disease and increased length of ICU stay (> 30 days). The risks factors associated with death were age, APACHE II, organ dysfunction, and tracheal intubation with or without mechanical ventilation. CONCLUSIONS: ICU-acquired infection is common and often associated with microbiological isolates of resistant organisms. This study may serve as an epidemiological reference to help the discussion of regional infection control policies.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):304-309
DOI 10.1590/S0103-507X2007000300006
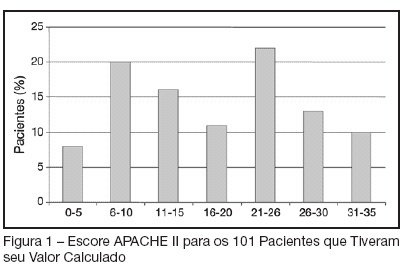
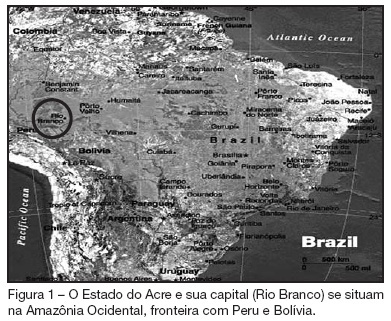
BACKGROUND AND OBJECTIVES: The intensive care Medicine was initiated in the State of the Acre in 1998. The aim of the present study was to establish clinical-epidemiological characteristics of adults and aged interned in a public intensive care unit (ICU) in the Amazon. METHODS: In 2004, a prospective study evaluated patients interned through the application of a questionnaire containing socioeconomics variables, invasive procedures, mechanical ventilation, nutritional support, surgical interventions and dialitic treatment. The gravity was established by APACHE II applied after 24 hours of internment. The follow up continued until the final destination in the unit: discharge or death. The statistical analysis used program SPSS, considering differences significant when p < 0.05. RESULTS: A total of 79 patients were assessed; 67.1% men; 59.5% white; 59.5% married; 50.4% came from other hospitals; 41.8% from the interior and 13.9% from others States and country (Bolivia) in frontier. The age varied from 20 to 104 (53.3 ± 18.6) years old; 30 (36.1%) aged (60 y old or more); 35 (44.3%) in surgical treatment; the median APACHE II was 18.4 ± 9.1. The stay in the UCI was of 10.2 ± 9.6 days; death occurred in 30 (38%) patients. Association between mortality and dialitic treatment, clinical indication, mechanical ventilation, vasoactive therapy, number of surgical interventions, hypoalbuminemia, lymphocytopenia and gravity was observed. CONCLUSIONS: The admission of severely ill patients coming from all over the State of Acre and frontier regions reflects the lack of ICU beds in the region.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):304-309
DOI 10.1590/S0103-507X2007000300006
BACKGROUND AND OBJECTIVES: The intensive care Medicine was initiated in the State of the Acre in 1998. The aim of the present study was to establish clinical-epidemiological characteristics of adults and aged interned in a public intensive care unit (ICU) in the Amazon. METHODS: In 2004, a prospective study evaluated patients interned through the application of a questionnaire containing socioeconomics variables, invasive procedures, mechanical ventilation, nutritional support, surgical interventions and dialitic treatment. The gravity was established by APACHE II applied after 24 hours of internment. The follow up continued until the final destination in the unit: discharge or death. The statistical analysis used program SPSS, considering differences significant when p < 0.05. RESULTS: A total of 79 patients were assessed; 67.1% men; 59.5% white; 59.5% married; 50.4% came from other hospitals; 41.8% from the interior and 13.9% from others States and country (Bolivia) in frontier. The age varied from 20 to 104 (53.3 ± 18.6) years old; 30 (36.1%) aged (60 y old or more); 35 (44.3%) in surgical treatment; the median APACHE II was 18.4 ± 9.1. The stay in the UCI was of 10.2 ± 9.6 days; death occurred in 30 (38%) patients. Association between mortality and dialitic treatment, clinical indication, mechanical ventilation, vasoactive therapy, number of surgical interventions, hypoalbuminemia, lymphocytopenia and gravity was observed. CONCLUSIONS: The admission of severely ill patients coming from all over the State of Acre and frontier regions reflects the lack of ICU beds in the region.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):327-330
DOI 10.1590/S0103-507X2007000300010
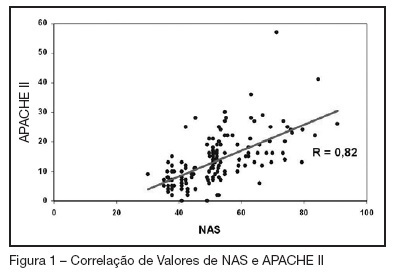
BACKGROUND AND OBJECTIVES: Searching the literature, we found no studies which correlate the NAS (Nursing Activities Score), who determines the real time of nursing evaluation and patient care, with mortality for prognostic index. The objectives this study were to know the values of the NAS score at ours service, try to find correlations between this values and the APACHE II index and to analyze the mortality rates with NAS scores. METHODS: This is a prospective ICU inpatient study from July to November/2005. Our data's of the APACHE II score were recorded from the QuaTI system study. Qui-square test or equivalent was done to compare the proportions. For the analyses we utilized the EPI-INFO-6 software. RESULTS: The sample was 148 patients, mean age of 55.5 years with 59.4% males. The mean hospitalization time were 9.1 days, mortality rate of 29.7%, mean NAS score of 51.5% and mean APACHE II score of 13.4. There were a positive correlation ship between NAS and APACHE II index (R = 0.82). Selecting only the patients with NAS more than 51 we found that 41 in 83 died and 42 in 83 survived. Those whose NAS were under 51, only 3 in 65 died and 62 in 65 survived (p < 0.005), identifying an statistically significant group. CONCLUSIONS: In this study the mean value of NAS were 51.5%. There were good correlation with the APACHE II index and we shown that the mortality rate was high in the higher NAS values.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):327-330
DOI 10.1590/S0103-507X2007000300010
BACKGROUND AND OBJECTIVES: Searching the literature, we found no studies which correlate the NAS (Nursing Activities Score), who determines the real time of nursing evaluation and patient care, with mortality for prognostic index. The objectives this study were to know the values of the NAS score at ours service, try to find correlations between this values and the APACHE II index and to analyze the mortality rates with NAS scores. METHODS: This is a prospective ICU inpatient study from July to November/2005. Our data's of the APACHE II score were recorded from the QuaTI system study. Qui-square test or equivalent was done to compare the proportions. For the analyses we utilized the EPI-INFO-6 software. RESULTS: The sample was 148 patients, mean age of 55.5 years with 59.4% males. The mean hospitalization time were 9.1 days, mortality rate of 29.7%, mean NAS score of 51.5% and mean APACHE II score of 13.4. There were a positive correlation ship between NAS and APACHE II index (R = 0.82). Selecting only the patients with NAS more than 51 we found that 41 in 83 died and 42 in 83 survived. Those whose NAS were under 51, only 3 in 65 died and 62 in 65 survived (p < 0.005), identifying an statistically significant group. CONCLUSIONS: In this study the mean value of NAS were 51.5%. There were good correlation with the APACHE II index and we shown that the mortality rate was high in the higher NAS values.
Abstract
Rev Bras Ter Intensiva. 2007;19(1):98-106
DOI 10.1590/S0103-507X2007000100013
BACKGROUND AND OBJECTIVES: Present a critical review of traumatic brain injury (TBI) in children and adolescents, focusing on severe TBI, the mortality and the factors related with poor outcome. CONTENTS: It was made a systematic review in MEDLINE, SciElo e Lilacs, with the key words: traumatic brain injury, craniocerebral trauma, children and mortality. The most important articles related in the Guidelines of Brain Trauma Foundation (2000 e 2003) were selected too. TBI is one of the most important causes of mortality and morbidity in children and adolescents, and morbidity in children and adolescents. The mortality variation was between 10% and 55%, depending of the patients select criteria, trauma severity and units where the studies were made. The children mortality was, in general, lower than that found in adults and the most important factors related with an increased mortality were: Glasgow Coma Score, hypotension, cerebral swelling and lower cerebral perfusion press. Severe TBI endpoint treatment is to correct the secondary brain lesions related factors. CONCLUSIONS: The factors related with better outcomes in children with severe TBI are still obscures, despite the large number of studies, large numbers of studies. Many of these factors can be avoided or correct by aggressive fluid resuscitation, surgery treatment, monitoration and adequate intensive care.
Abstract
Rev Bras Ter Intensiva. 2007;19(1):98-106
DOI 10.1590/S0103-507X2007000100013
BACKGROUND AND OBJECTIVES: Present a critical review of traumatic brain injury (TBI) in children and adolescents, focusing on severe TBI, the mortality and the factors related with poor outcome. CONTENTS: It was made a systematic review in MEDLINE, SciElo e Lilacs, with the key words: traumatic brain injury, craniocerebral trauma, children and mortality. The most important articles related in the Guidelines of Brain Trauma Foundation (2000 e 2003) were selected too. TBI is one of the most important causes of mortality and morbidity in children and adolescents, and morbidity in children and adolescents. The mortality variation was between 10% and 55%, depending of the patients select criteria, trauma severity and units where the studies were made. The children mortality was, in general, lower than that found in adults and the most important factors related with an increased mortality were: Glasgow Coma Score, hypotension, cerebral swelling and lower cerebral perfusion press. Severe TBI endpoint treatment is to correct the secondary brain lesions related factors. CONCLUSIONS: The factors related with better outcomes in children with severe TBI are still obscures, despite the large number of studies, large numbers of studies. Many of these factors can be avoided or correct by aggressive fluid resuscitation, surgery treatment, monitoration and adequate intensive care.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)