Intensive care units Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2008;20(4):362-369
DOI 10.1590/S0103-507X2008000400008
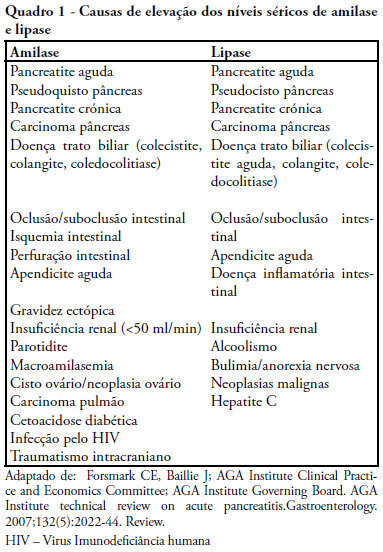
OBJECTIVES: Elevated lipase and amylase are commonly found in patients in intensive care unit without a previously recognized pancreatic illness, constituting a diagnostic and therapeutic challenge. The authors therefore proposed to determine the frequency of asymptomatic high serum lipase in critically ill patients, involved risk factors and outcome. METHODS: Retrospective study of patients admitted in an intensive care unit from January 1 to December 31, 2006, excluding admissions for acute pancreatitis, history of pancreatic disease, renal insufficiency or lacking of data. Patients were divided in two groups (with and without high serum lipase) that were compared for clinical, laboratory and radiological variables. Statistical analysis: SPSS 13; Student's t test and Chi-square test (CI 95%) with statistical significance if p< 0.05). RESULTS: 102 patients were included with high serum lipase was present in 39.2% of patients, mean lipase of 797U/L. Patients with high serum lipase had longer hospital stay (p< 0.001), parenteral nutrition (p< 0.001), ventilator support (p=0.04), fever (p< 0.001), hyperamylasemia (p<0.05), hyperbilirrubinemia (p=0.003) and rise of transaminases (p=0.001), with no significant differences in diagnosis, gender, age, APACHE II, SOFA, SAPS, mortality, hypotension, alkaline phosphatase, hemoglobin, lactate, tolerance to enteral nutrition and use of propofol. Imaging study revealed pancreatic alterations in two patients with high serum lipase. CONCLUSIONS: Elevated lipase was commonly found in critical patients, it related with longer length of stay but was not accompanied by increased clinical severity or mortality. It was more frequent with parenteral nutrition. A minority of patients met the criteria of acute pancreatitis.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):362-369
DOI 10.1590/S0103-507X2008000400008
OBJECTIVES: Elevated lipase and amylase are commonly found in patients in intensive care unit without a previously recognized pancreatic illness, constituting a diagnostic and therapeutic challenge. The authors therefore proposed to determine the frequency of asymptomatic high serum lipase in critically ill patients, involved risk factors and outcome. METHODS: Retrospective study of patients admitted in an intensive care unit from January 1 to December 31, 2006, excluding admissions for acute pancreatitis, history of pancreatic disease, renal insufficiency or lacking of data. Patients were divided in two groups (with and without high serum lipase) that were compared for clinical, laboratory and radiological variables. Statistical analysis: SPSS 13; Student's t test and Chi-square test (CI 95%) with statistical significance if p< 0.05). RESULTS: 102 patients were included with high serum lipase was present in 39.2% of patients, mean lipase of 797U/L. Patients with high serum lipase had longer hospital stay (p< 0.001), parenteral nutrition (p< 0.001), ventilator support (p=0.04), fever (p< 0.001), hyperamylasemia (p<0.05), hyperbilirrubinemia (p=0.003) and rise of transaminases (p=0.001), with no significant differences in diagnosis, gender, age, APACHE II, SOFA, SAPS, mortality, hypotension, alkaline phosphatase, hemoglobin, lactate, tolerance to enteral nutrition and use of propofol. Imaging study revealed pancreatic alterations in two patients with high serum lipase. CONCLUSIONS: Elevated lipase was commonly found in critical patients, it related with longer length of stay but was not accompanied by increased clinical severity or mortality. It was more frequent with parenteral nutrition. A minority of patients met the criteria of acute pancreatitis.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):370-375
DOI 10.1590/S0103-507X2008000400009
OBJECTIVE: The aim of this study was to understand the experience of family members, during a patient's stay in the intensive care unit of public and private hospitals using an approximation to the phenomenology referential. METHODS: We interviewed 27 relatives of adult patients, 10 from a public institution and 17 from a private one. RESULTS: From analyses of interviews in a public institution, four thematic categories emerged. In a private institution six categories were identified. Searching for differences and similarities, four similar thematic categories were perceived in both institutions and two categories were absent in the public hospital. CONCLUSION: There are no significant differences between categories in private and public hospitals. This indicates that family behavior and reactions to patient's admission to the ICU are not associated with social or financial aspects. However, a greater knowledge of government policies and programs is necessary, because they favor humanization by allowing family members to accompany the patient in tertiary services.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):370-375
DOI 10.1590/S0103-507X2008000400009
OBJECTIVE: The aim of this study was to understand the experience of family members, during a patient's stay in the intensive care unit of public and private hospitals using an approximation to the phenomenology referential. METHODS: We interviewed 27 relatives of adult patients, 10 from a public institution and 17 from a private one. RESULTS: From analyses of interviews in a public institution, four thematic categories emerged. In a private institution six categories were identified. Searching for differences and similarities, four similar thematic categories were perceived in both institutions and two categories were absent in the public hospital. CONCLUSION: There are no significant differences between categories in private and public hospitals. This indicates that family behavior and reactions to patient's admission to the ICU are not associated with social or financial aspects. However, a greater knowledge of government policies and programs is necessary, because they favor humanization by allowing family members to accompany the patient in tertiary services.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):385-393
DOI 10.1590/S0103-507X2008000400011
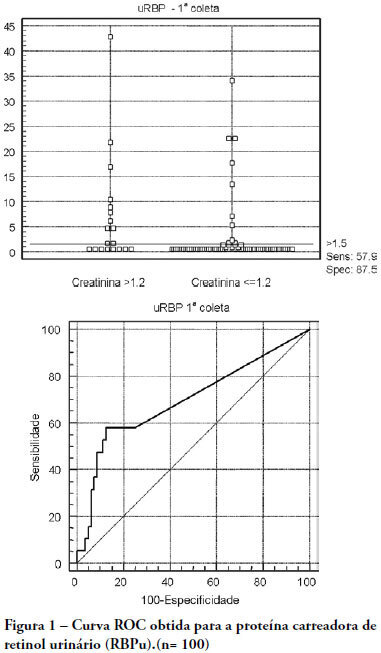
OBJECTIVES: The early assessment of renal dysfunction using common markers does not provide either a sensitive or specific indication of renal dysfunction in critically ill patients. More specific and sensitive markers are desirable for the early detection of an initial renal pathophysiological process. Urinary retinol-binding protein could be an alternative method to early evaluation of renal function in these patients. METHODS: This study followed-up 100 critical care patients and assessed their clinical and laboratory variables, including plasma creatinine and urinary retinol-binding ratio, and demographic variables. RESULTS: The sample was characterized by geriatric (63.4±15.6 years), male (68%), being 53% surgical patients. Statistical analysis showed association between plasma creatinine and the following variables: gender (p-0.026), age (p-0.038), use of vasoactive drugs (p-0.003), proteinuria (p-0.025), Acute Physiological Chronic Health Evaluation (APACHE) II score (p-0.000), urea (p-0.000), potassium (p-0.003) and estimated creatinine clearance (p-0.000). Urinary retinol-binding protein was correlated with more variables: weight, use of invasive ventilation (p-0.000), use of nonsteroidal antiinflammatory drugs (p-0.018), use of vasoactive drugs (p-0.021), high temperature (>37.5ºC) (p-0.005), proteinuria (p-0.000), bilirubinuria (p-0.004), urinary flow (p-0.019), minimal diastolic pressure (p-0.032), minimal systolic pressure (p-0.029), APACHE II (p-0.000), creatinine (p-0.001), urea (p-0.001), estimated creatinine clearance (p-0.000). Urinary retinol-binding protein also tended to associate with previous renal disease, vasculopathy and neoplasm. Sodium excretion fraction correlated with plasma creatinine and urinary retinol-binding protein in univariate analysis. CONCLUSIONS: Urinary retinol-binding protein might be considered in clinical practice as a better marker regarding diagnostic performance in patients at risk of developing acute kidney injury, when compared with other markers routinely used. Moreover, urinary retinol-binding protein has other features of a good diagnostic test - it is a practical and non-invasive method.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):385-393
DOI 10.1590/S0103-507X2008000400011
OBJECTIVES: The early assessment of renal dysfunction using common markers does not provide either a sensitive or specific indication of renal dysfunction in critically ill patients. More specific and sensitive markers are desirable for the early detection of an initial renal pathophysiological process. Urinary retinol-binding protein could be an alternative method to early evaluation of renal function in these patients. METHODS: This study followed-up 100 critical care patients and assessed their clinical and laboratory variables, including plasma creatinine and urinary retinol-binding ratio, and demographic variables. RESULTS: The sample was characterized by geriatric (63.4±15.6 years), male (68%), being 53% surgical patients. Statistical analysis showed association between plasma creatinine and the following variables: gender (p-0.026), age (p-0.038), use of vasoactive drugs (p-0.003), proteinuria (p-0.025), Acute Physiological Chronic Health Evaluation (APACHE) II score (p-0.000), urea (p-0.000), potassium (p-0.003) and estimated creatinine clearance (p-0.000). Urinary retinol-binding protein was correlated with more variables: weight, use of invasive ventilation (p-0.000), use of nonsteroidal antiinflammatory drugs (p-0.018), use of vasoactive drugs (p-0.021), high temperature (>37.5ºC) (p-0.005), proteinuria (p-0.000), bilirubinuria (p-0.004), urinary flow (p-0.019), minimal diastolic pressure (p-0.032), minimal systolic pressure (p-0.029), APACHE II (p-0.000), creatinine (p-0.001), urea (p-0.001), estimated creatinine clearance (p-0.000). Urinary retinol-binding protein also tended to associate with previous renal disease, vasculopathy and neoplasm. Sodium excretion fraction correlated with plasma creatinine and urinary retinol-binding protein in univariate analysis. CONCLUSIONS: Urinary retinol-binding protein might be considered in clinical practice as a better marker regarding diagnostic performance in patients at risk of developing acute kidney injury, when compared with other markers routinely used. Moreover, urinary retinol-binding protein has other features of a good diagnostic test - it is a practical and non-invasive method.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):249-253
DOI 10.1590/S0103-507X2008000300007
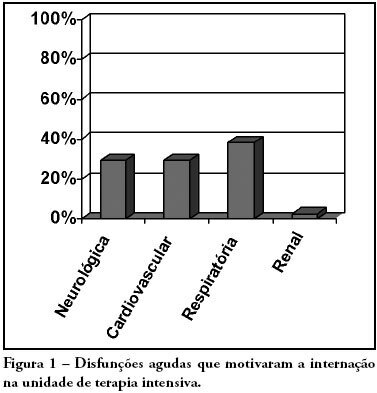
OBJECTIVES: Due to the high incidence in our service, we did object on this study describe the features and outcome of patients with systemic lupus erythematosus (SLE) admitted to the intensive care unit of Walter Cantídio University Hospital METHODS: Patients were restrospectively characterized according to demography parameters, time of diagnosis of SLE, organ dysfunction and laboratorial parameters at admission, supportive therapies during their stay, length of stay in the hospital before admission, length of stay in the unit, readmission to the unit and outcome. We also evaluated Systemic Lupus Erythematosus Disease Activity (SLEDAI) score, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, expected mortality and standardized mortality ratio. RESULTS: From November 2003 to October 2006, 1,052 patients were admitted to the intensive care unit. Fifty patients had SLE and were included in this retrospective study. Of the 50 patients with SLE admitted to the ICU, 88.2% were female. The mean age was 30.3 ± 12.8 years. The median time of diagnosis of SLE was 67 months. The most common organ dysfunctions were renal (70.6%), cardiovascular (61.8%), respiratory (55.9%) and neurological (55.9%). The main reasons for admission to the ICU were respiratory (38.2%), cardiologic (29.4%) and neurological (29.4%) dysfunctions. Among the intensive care therapies, 44.1% of the patients needed blood products, 41.2% vasopressor agents and 35.3% mechanical ventilation, 23.5% dialysis. The mean SLEDAI score was 15.0 ± 12.2. The mean APACHE II score was 19.3 ± 6.8, with a predicted mortality rate of 37.6%. The actual mortality rate in ICU was 29.4%, with 8.8% before 48 hours. The standardized mortality ratio was 0.78. Patients with APACHE II > 18, with more than 3 acute organ involvements, leukopenia (< 4000 cells/mm3) and gastrointestinal or metabolic involvement had higher mortality in the intensive care unit. CONCLUSION: Although the severity of patients at admission to the ICU, demonstrated by APACHE II and the acute dysfunctions, the outcomes of analysed patients sugest susceptibility to the therapy.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):249-253
DOI 10.1590/S0103-507X2008000300007
OBJECTIVES: Due to the high incidence in our service, we did object on this study describe the features and outcome of patients with systemic lupus erythematosus (SLE) admitted to the intensive care unit of Walter Cantídio University Hospital METHODS: Patients were restrospectively characterized according to demography parameters, time of diagnosis of SLE, organ dysfunction and laboratorial parameters at admission, supportive therapies during their stay, length of stay in the hospital before admission, length of stay in the unit, readmission to the unit and outcome. We also evaluated Systemic Lupus Erythematosus Disease Activity (SLEDAI) score, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, expected mortality and standardized mortality ratio. RESULTS: From November 2003 to October 2006, 1,052 patients were admitted to the intensive care unit. Fifty patients had SLE and were included in this retrospective study. Of the 50 patients with SLE admitted to the ICU, 88.2% were female. The mean age was 30.3 ± 12.8 years. The median time of diagnosis of SLE was 67 months. The most common organ dysfunctions were renal (70.6%), cardiovascular (61.8%), respiratory (55.9%) and neurological (55.9%). The main reasons for admission to the ICU were respiratory (38.2%), cardiologic (29.4%) and neurological (29.4%) dysfunctions. Among the intensive care therapies, 44.1% of the patients needed blood products, 41.2% vasopressor agents and 35.3% mechanical ventilation, 23.5% dialysis. The mean SLEDAI score was 15.0 ± 12.2. The mean APACHE II score was 19.3 ± 6.8, with a predicted mortality rate of 37.6%. The actual mortality rate in ICU was 29.4%, with 8.8% before 48 hours. The standardized mortality ratio was 0.78. Patients with APACHE II > 18, with more than 3 acute organ involvements, leukopenia (< 4000 cells/mm3) and gastrointestinal or metabolic involvement had higher mortality in the intensive care unit. CONCLUSION: Although the severity of patients at admission to the ICU, demonstrated by APACHE II and the acute dysfunctions, the outcomes of analysed patients sugest susceptibility to the therapy.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):278-285
DOI 10.1590/S0103-507X2008000300011
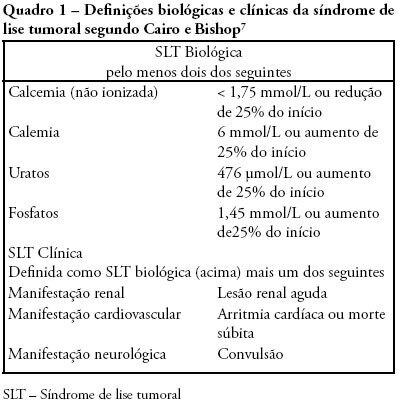
Tumor lysis syndrome is characterized by the massive destruction of malignant cells and the release in the extra-cellular space of their content. While Tumor lysis syndrome may occur spontaneously before treatment, it usually develops shortly after the initiation of cytotoxic chemotherapy. These metabolites can overwhelm the homeostatic mechanisms with development of hyperuricaemia, hyperkalaemia, hyperphosphataemia, and hypocalcaemia. These biological manifestations may lead to clinical manifestations including, acute kidney injury, seizure, or sudden death that require intensive care. Since clinical tumor lysis syndrome is associated with a poor prognosis both prevention of tumor lysis syndrome and prevention of clinical consequences of tumor lysis syndrome are mandatory. The objective of this review is to describe pathophysiological mechanisms, biological and clinical manifestations of tumor Lysis syndrome, and to provide upto-date guidelines to ensure prevention of tumor lysis syndrome. Review of selected studies on tumor lysis syndrome published at the PubMed database www.pubmed.gov during the last 20 years. Additional references were retrieved from the studies initially selected. Tumor lysis syndrome is a frequent and life-threatening complication of the newly diagnosed malignancies. Preventive measures, including hydration, uricolytic agents, eviction of factors predisposing to acute kidney injury and, in the more severe patients, on prophylactic renal replacement therapy, are required to prevent or limit clinical consequences of Tumor lysis syndrome. However optimal timing and modalities of prevention remains unknown and may be modified by the changing spectrum of patients at risk of tumor lysis syndrome. Development and validation of risk based strategies is required to limit the high morbidity and mortality of this complication.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):278-285
DOI 10.1590/S0103-507X2008000300011
Tumor lysis syndrome is characterized by the massive destruction of malignant cells and the release in the extra-cellular space of their content. While Tumor lysis syndrome may occur spontaneously before treatment, it usually develops shortly after the initiation of cytotoxic chemotherapy. These metabolites can overwhelm the homeostatic mechanisms with development of hyperuricaemia, hyperkalaemia, hyperphosphataemia, and hypocalcaemia. These biological manifestations may lead to clinical manifestations including, acute kidney injury, seizure, or sudden death that require intensive care. Since clinical tumor lysis syndrome is associated with a poor prognosis both prevention of tumor lysis syndrome and prevention of clinical consequences of tumor lysis syndrome are mandatory. The objective of this review is to describe pathophysiological mechanisms, biological and clinical manifestations of tumor Lysis syndrome, and to provide upto-date guidelines to ensure prevention of tumor lysis syndrome. Review of selected studies on tumor lysis syndrome published at the PubMed database www.pubmed.gov during the last 20 years. Additional references were retrieved from the studies initially selected. Tumor lysis syndrome is a frequent and life-threatening complication of the newly diagnosed malignancies. Preventive measures, including hydration, uricolytic agents, eviction of factors predisposing to acute kidney injury and, in the more severe patients, on prophylactic renal replacement therapy, are required to prevent or limit clinical consequences of Tumor lysis syndrome. However optimal timing and modalities of prevention remains unknown and may be modified by the changing spectrum of patients at risk of tumor lysis syndrome. Development and validation of risk based strategies is required to limit the high morbidity and mortality of this complication.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):235-240
DOI 10.1590/S0103-507X2008000300005
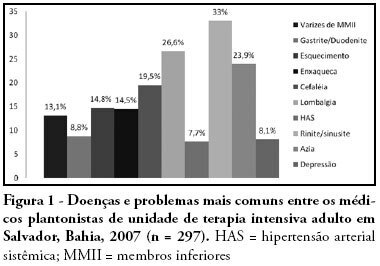
OBJECTIVES: Burnout syndrome is a response to prolonged occupational stress that involves three main dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment. The aim of this study was to describe socio-demographic characteristics of intensive care unit physicians and evaluate factors associated to the presence of Burnout syndrome in this population. METHODS: A cross-sectional study was performed to evaluate physicians who have worked in intensive care units from the city of Salvador (Bahia - Brazil) with a minimum weekly workload of 12-hour. An anonymous self-reported questionnaire was used and it was divided into two parts: socio-demographic characteristics and evaluation of Burnout syndrome through Maslach Burnout Inventory. RESULTS: We studied 297 physicians and most of them were male (70%). The mean age and time of graduation were, respectively, 34.2 and 9 years. High levels of emotional exhaustion, depersonalization, and reduced personal accomplishment were found in respectively, 47.5%, 24.6% and 28.3%. The prevalence of Burnout syndrome, considered as high level in at least one dimension, was of 63.3%. This prevalence was statistically lower in physicians specialized on intensive care, those with more than nine years of graduation and those who intend to continue working in intensive care units for more than 10 years. The prevalence was higher in the doctors with more than 24-hours of uninterrupted intensive care work per week. CONCLUSIONS: Burnout syndrome was common among intensive care physicians and it was more frequent in the youngest doctors, with higher workload and without specialization on intensive care.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):235-240
DOI 10.1590/S0103-507X2008000300005
OBJECTIVES: Burnout syndrome is a response to prolonged occupational stress that involves three main dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment. The aim of this study was to describe socio-demographic characteristics of intensive care unit physicians and evaluate factors associated to the presence of Burnout syndrome in this population. METHODS: A cross-sectional study was performed to evaluate physicians who have worked in intensive care units from the city of Salvador (Bahia - Brazil) with a minimum weekly workload of 12-hour. An anonymous self-reported questionnaire was used and it was divided into two parts: socio-demographic characteristics and evaluation of Burnout syndrome through Maslach Burnout Inventory. RESULTS: We studied 297 physicians and most of them were male (70%). The mean age and time of graduation were, respectively, 34.2 and 9 years. High levels of emotional exhaustion, depersonalization, and reduced personal accomplishment were found in respectively, 47.5%, 24.6% and 28.3%. The prevalence of Burnout syndrome, considered as high level in at least one dimension, was of 63.3%. This prevalence was statistically lower in physicians specialized on intensive care, those with more than nine years of graduation and those who intend to continue working in intensive care units for more than 10 years. The prevalence was higher in the doctors with more than 24-hours of uninterrupted intensive care work per week. CONCLUSIONS: Burnout syndrome was common among intensive care physicians and it was more frequent in the youngest doctors, with higher workload and without specialization on intensive care.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):18-21
DOI 10.1590/S0103-507X2006000100004
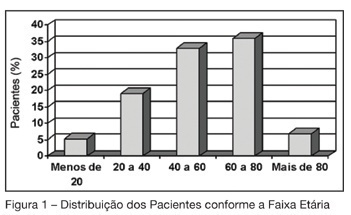
BACKGROUND AND OBJECTIVES: The aim of this study was to analyze the morbidity and the mortality of critically ill patients admitted to the intensive care unit in a teaching hospital, using the APACHE II score. METHODS: Descriptive and retrospective study, with analysis of 300 patients admitted to ICU from March 2004 to July 2005. RESULTS: Of the 300 patients admitted to ICU, 51.7% were men, average 54.2 ± 19.57 years and 78% from the wards of the teaching hospital itself. There was more prevalence of patients aged 60 years or older (43%). The main dysfunctions were from the respiratory and cardiocirculatory systems. Length of stay in ICU was 7.51 ± 8.21 days. The mean of APACHE II was 16.48 ± 7.67, with meaningful difference between survivors and deceased patients. The real mortality rate in ICU was 32.7%, without meaningful difference between patients that died before or after 48 hours. The standardized mortality ratio was 1.1. CONCLUSIONS: Despite the severity of the patients admitted to ICU, the standardized mortality ratio suggests a satisfactory quality in the service.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):18-21
DOI 10.1590/S0103-507X2006000100004
BACKGROUND AND OBJECTIVES: The aim of this study was to analyze the morbidity and the mortality of critically ill patients admitted to the intensive care unit in a teaching hospital, using the APACHE II score. METHODS: Descriptive and retrospective study, with analysis of 300 patients admitted to ICU from March 2004 to July 2005. RESULTS: Of the 300 patients admitted to ICU, 51.7% were men, average 54.2 ± 19.57 years and 78% from the wards of the teaching hospital itself. There was more prevalence of patients aged 60 years or older (43%). The main dysfunctions were from the respiratory and cardiocirculatory systems. Length of stay in ICU was 7.51 ± 8.21 days. The mean of APACHE II was 16.48 ± 7.67, with meaningful difference between survivors and deceased patients. The real mortality rate in ICU was 32.7%, without meaningful difference between patients that died before or after 48 hours. The standardized mortality ratio was 1.1. CONCLUSIONS: Despite the severity of the patients admitted to ICU, the standardized mortality ratio suggests a satisfactory quality in the service.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):27-33
DOI 10.1590/S0103-507X2006000100006
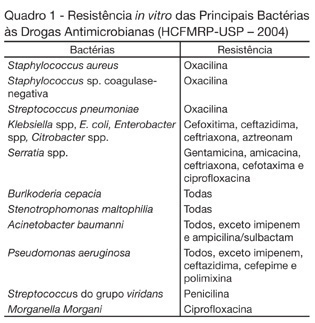
BACKGROUND AND OBJECTIVES: Nosocomial infection represents a challenge in clinical practice involving hospitalized patients, as they considerably extend the hospitalization period and morbidity and mortality rates and, at the same time, increase hospital costs. Given their clinical conditions, which require invasive procedures and antimicrobial treatment, hospitalized patients, especially at the Intensive Care Unit, are particularly susceptible to hospital infection. This study aimed to evaluate the occurrence of multiresistant bacteria in patients hospitalized at the Intensive Care Unit of a Brazilian emergency hospital. METHODS: Our retrospective study was approved by the Ethics Committee and considered the period between October 2003 and September 2004. A database was developed through variable coding and double entry, and Statistical Package for Social Sciences (SPSS) software, version 10.0, was used for statistical analysis. RESULTS: Multiresistant bacteria were identified in 68 patients, 47 (69.1%) of whom were men, with 55 years as the mean age. All patients were submitted to endotracheal intubation and central venipuncture. The most frequent bacteria were coagulase-negative Staphylococcus sp. (36.4%), followed by Staphylococcus aureus (19%). Cephalosporin was the most frequently used (21.4%) antimicrobial agent. CONCLUSIONS: Knowledge on infection occurrence provokes reflections on multiresistance, directs educative actions and favors interventions to prevent and control problem situations.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):27-33
DOI 10.1590/S0103-507X2006000100006
BACKGROUND AND OBJECTIVES: Nosocomial infection represents a challenge in clinical practice involving hospitalized patients, as they considerably extend the hospitalization period and morbidity and mortality rates and, at the same time, increase hospital costs. Given their clinical conditions, which require invasive procedures and antimicrobial treatment, hospitalized patients, especially at the Intensive Care Unit, are particularly susceptible to hospital infection. This study aimed to evaluate the occurrence of multiresistant bacteria in patients hospitalized at the Intensive Care Unit of a Brazilian emergency hospital. METHODS: Our retrospective study was approved by the Ethics Committee and considered the period between October 2003 and September 2004. A database was developed through variable coding and double entry, and Statistical Package for Social Sciences (SPSS) software, version 10.0, was used for statistical analysis. RESULTS: Multiresistant bacteria were identified in 68 patients, 47 (69.1%) of whom were men, with 55 years as the mean age. All patients were submitted to endotracheal intubation and central venipuncture. The most frequent bacteria were coagulase-negative Staphylococcus sp. (36.4%), followed by Staphylococcus aureus (19%). Cephalosporin was the most frequently used (21.4%) antimicrobial agent. CONCLUSIONS: Knowledge on infection occurrence provokes reflections on multiresistance, directs educative actions and favors interventions to prevent and control problem situations.