Intensive care, neonatal Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(2):186-192
DOI 10.5935/0103-507X.20190030
To describe the characteristics of the heel prick test in newborns admitted to the intensive care unit of a university hospital as well as to determine whether maternal and fetal conditions could have affected the results of this test.
Retrospective longitudinal study with a quantitative approach that evaluated 240 medical records. The data collected were analyzed by descriptive statistical analysis.
There was a predominance of pregnant women aged 20 to 34 years who had a complete secondary education and who had more than six prenatal care visits. Maternal complications or pathologies occurred in 60% of the mothers, and most (67.5%) did not present any condition that could have affected the heel prick test results. Most newborns were premature and exhibited low birth weight. Approximately 90% of newborns exhibited conditions that could have influenced the test, especially prematurity, parenteral nutrition and blood transfusion. Of the 240 newborns, 25% had abnormal heel prick test results, especially for cystic fibrosis and congenital adrenal hyperplasia.
There are maternal and neonatal conditions that can affect heel prick test results, and therefore, their investigation is essential, aiming to guide measures that promote mother and child health and consolidate neonatal screening in this population.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):186-192
DOI 10.5935/0103-507X.20190030
To describe the characteristics of the heel prick test in newborns admitted to the intensive care unit of a university hospital as well as to determine whether maternal and fetal conditions could have affected the results of this test.
Retrospective longitudinal study with a quantitative approach that evaluated 240 medical records. The data collected were analyzed by descriptive statistical analysis.
There was a predominance of pregnant women aged 20 to 34 years who had a complete secondary education and who had more than six prenatal care visits. Maternal complications or pathologies occurred in 60% of the mothers, and most (67.5%) did not present any condition that could have affected the heel prick test results. Most newborns were premature and exhibited low birth weight. Approximately 90% of newborns exhibited conditions that could have influenced the test, especially prematurity, parenteral nutrition and blood transfusion. Of the 240 newborns, 25% had abnormal heel prick test results, especially for cystic fibrosis and congenital adrenal hyperplasia.
There are maternal and neonatal conditions that can affect heel prick test results, and therefore, their investigation is essential, aiming to guide measures that promote mother and child health and consolidate neonatal screening in this population.
Abstract
Rev Bras Ter Intensiva. 2016;28(3):310-314
DOI 10.5935/0103-507X.20160041
To investigate possible stressors to which newborns are exposed in the neonatal intensive care unit.
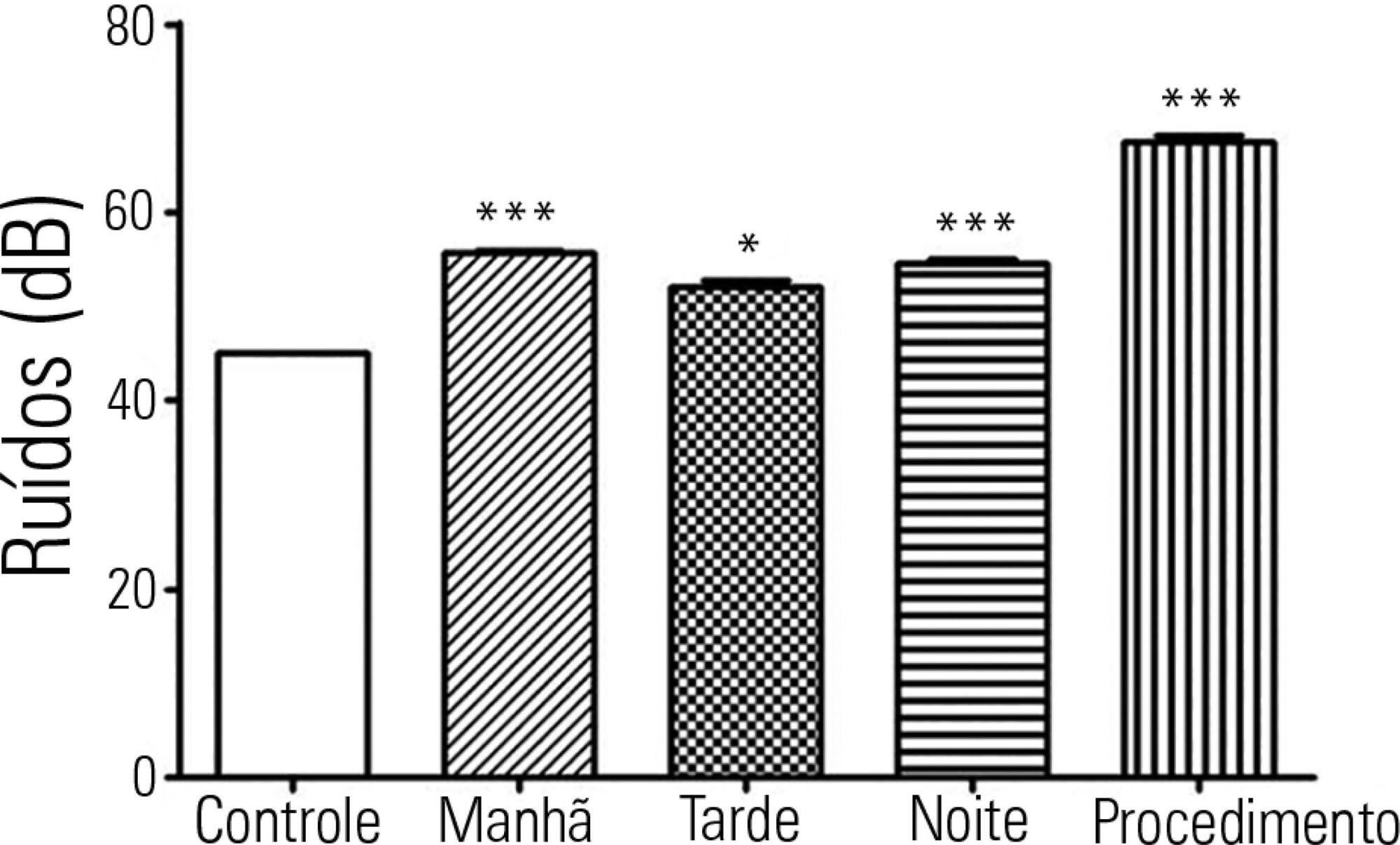
The levels of continuous noise were checked by a decibel meter positioned near the ear of the newborn, brightness was observed by a light meter positioned in the incubator in front of the newborn's eyes, and temperature was checked through the incubator display. The evaluations were performed in three periods of the day, with ten measurements taken at one-minute intervals during each shift for the subsequent statistical analysis.
All shifts showed noise above acceptable levels. Morning (p < 0.001), afternoon (p < 0.05) and night (p < 0.001) showed a significant increase compared to the control. The brightness significantly exceeded the normal range (p < 0.01) in the morning. We observed that only one of the incubators was within the normal temperature limits.
The noise, brightness and temperature intensities were not in accordance with regulatory standards and thus might be possible stressors to newborns.
Abstract
Rev Bras Ter Intensiva. 2016;28(3):310-314
DOI 10.5935/0103-507X.20160041
To investigate possible stressors to which newborns are exposed in the neonatal intensive care unit.
The levels of continuous noise were checked by a decibel meter positioned near the ear of the newborn, brightness was observed by a light meter positioned in the incubator in front of the newborn's eyes, and temperature was checked through the incubator display. The evaluations were performed in three periods of the day, with ten measurements taken at one-minute intervals during each shift for the subsequent statistical analysis.
All shifts showed noise above acceptable levels. Morning (p < 0.001), afternoon (p < 0.05) and night (p < 0.001) showed a significant increase compared to the control. The brightness significantly exceeded the normal range (p < 0.01) in the morning. We observed that only one of the incubators was within the normal temperature limits.
The noise, brightness and temperature intensities were not in accordance with regulatory standards and thus might be possible stressors to newborns.
Abstract
Rev Bras Ter Intensiva. 2016;28(3):341-347
DOI 10.5935/0103-507X.20160058
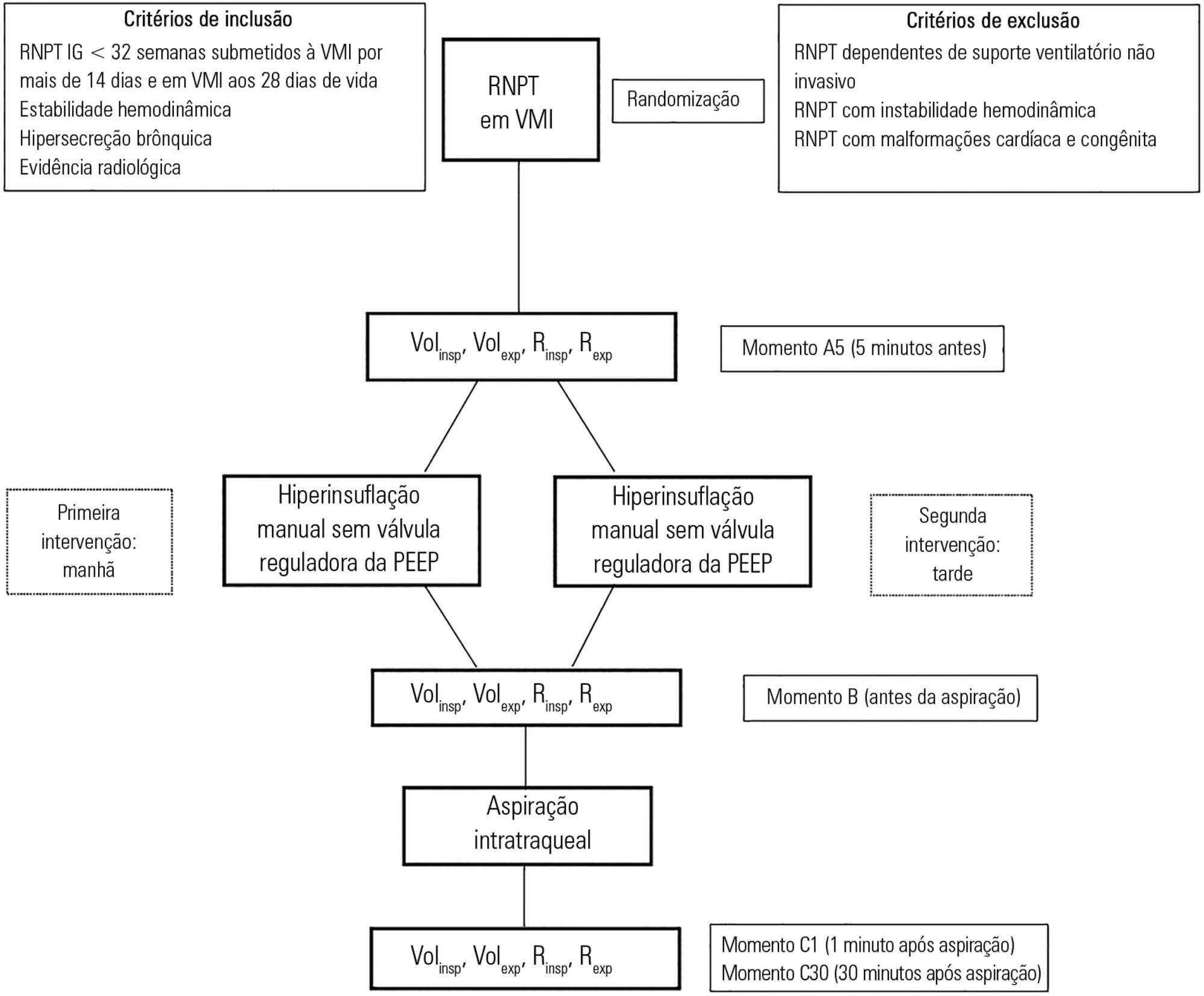
To assess the effects of manual hyperinflation, performed with a manual resuscitator with and without the positive end-expiratory pressure valve, on the respiratory function of preterm newborns under mechanical ventilation.
Cross-sectional study of hemodynamically stable preterm newborns with gestational age of less than 32 weeks, under mechanical ventilation and dependent on it at 28 days of life. Manual hyperinflation was applied randomly, alternating the use or not of the positive end-expiratory pressure valve, followed by tracheal aspiration for ending the maneuver. For nominal data, the two-tailed Wilcoxon test was applied at the 5% significance level and 80% power.
Twenty-eight preterm newborns, with an average birth weight of 1,005.71 ± 372.16g, an average gestational age of 28.90 ± 1.79 weeks, an average corrected age of 33.26 ± 1.78 weeks, and an average mechanical ventilation time of 29.5 (15 - 53) days, were studied. Increases in inspiratory and expiratory volumes occurred between time-points A5 (before the maneuver) and C1 (immediately after tracheal aspiration) in both the maneuver with the valve (p = 0.001 and p = 0.009) and without the valve (p = 0.026 and p = 0.001), respectively. There was also an increase in expiratory resistance between time-points A5 and C1 (p = 0.044).
Lung volumes increased when performing the maneuver with and without the valve, with a significant difference in the first minute after aspiration. There was a significant difference in expiratory resistance between the time-points A5 (before the maneuver) and C1 (immediately after tracheal aspiration) in the first minute after aspiration within each maneuver.
Abstract
Rev Bras Ter Intensiva. 2016;28(3):341-347
DOI 10.5935/0103-507X.20160058
To assess the effects of manual hyperinflation, performed with a manual resuscitator with and without the positive end-expiratory pressure valve, on the respiratory function of preterm newborns under mechanical ventilation.
Cross-sectional study of hemodynamically stable preterm newborns with gestational age of less than 32 weeks, under mechanical ventilation and dependent on it at 28 days of life. Manual hyperinflation was applied randomly, alternating the use or not of the positive end-expiratory pressure valve, followed by tracheal aspiration for ending the maneuver. For nominal data, the two-tailed Wilcoxon test was applied at the 5% significance level and 80% power.
Twenty-eight preterm newborns, with an average birth weight of 1,005.71 ± 372.16g, an average gestational age of 28.90 ± 1.79 weeks, an average corrected age of 33.26 ± 1.78 weeks, and an average mechanical ventilation time of 29.5 (15 - 53) days, were studied. Increases in inspiratory and expiratory volumes occurred between time-points A5 (before the maneuver) and C1 (immediately after tracheal aspiration) in both the maneuver with the valve (p = 0.001 and p = 0.009) and without the valve (p = 0.026 and p = 0.001), respectively. There was also an increase in expiratory resistance between time-points A5 and C1 (p = 0.044).
Lung volumes increased when performing the maneuver with and without the valve, with a significant difference in the first minute after aspiration. There was a significant difference in expiratory resistance between the time-points A5 (before the maneuver) and C1 (immediately after tracheal aspiration) in the first minute after aspiration within each maneuver.
Abstract
Rev Bras Ter Intensiva. 2016;28(3):270-277
DOI 10.5935/0103-507X.20160053
To estimate the prevalence of burnout in intensivist doctors working in adult, pediatric and neonatal intensive care units in five Brazilian capitals.
Descriptive epidemiological study with a random sample stratified by conglomerate with 180 intensivist doctors from five capitals representing the Brazilian geographic regions: Porto Alegre (RS), Sao Paulo (SP), Salvador (BA), Goiania (GO) and Belem (PA). A self-administered questionnaire examining sociodemographic data and the level of burnout was evaluated through the Maslach Burnout Inventory.
A total of 180 doctors were evaluated, of which 54.4% were female. The average age was 39 ± 8.1 years, 63.4% had specialization as the highest degree, 55.7% had up to 10 years of work experience in an intensive care unit, and 46.1% had the title intensive care specialist. Most (50.3%) had weekly workloads between 49 and 72 hours, and the most frequent employee type was salaried. High levels of emotional exhaustion, depersonalization and inefficacy were found (50.6%, 26.1% and 15.0%, respectively). The prevalence of burnout was 61.7% when considering a high level in at least one dimension and 5% with a high level in three dimensions simultaneously.
A high prevalence of burnout syndrome among intensivist doctors was observed. Strategies for the promotion and protection of health in these workers must be discussed and implemented in hospitals.
Abstract
Rev Bras Ter Intensiva. 2016;28(3):270-277
DOI 10.5935/0103-507X.20160053
To estimate the prevalence of burnout in intensivist doctors working in adult, pediatric and neonatal intensive care units in five Brazilian capitals.
Descriptive epidemiological study with a random sample stratified by conglomerate with 180 intensivist doctors from five capitals representing the Brazilian geographic regions: Porto Alegre (RS), Sao Paulo (SP), Salvador (BA), Goiania (GO) and Belem (PA). A self-administered questionnaire examining sociodemographic data and the level of burnout was evaluated through the Maslach Burnout Inventory.
A total of 180 doctors were evaluated, of which 54.4% were female. The average age was 39 ± 8.1 years, 63.4% had specialization as the highest degree, 55.7% had up to 10 years of work experience in an intensive care unit, and 46.1% had the title intensive care specialist. Most (50.3%) had weekly workloads between 49 and 72 hours, and the most frequent employee type was salaried. High levels of emotional exhaustion, depersonalization and inefficacy were found (50.6%, 26.1% and 15.0%, respectively). The prevalence of burnout was 61.7% when considering a high level in at least one dimension and 5% with a high level in three dimensions simultaneously.
A high prevalence of burnout syndrome among intensivist doctors was observed. Strategies for the promotion and protection of health in these workers must be discussed and implemented in hospitals.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):386-392
DOI 10.1590/S0103-507X2012000400016
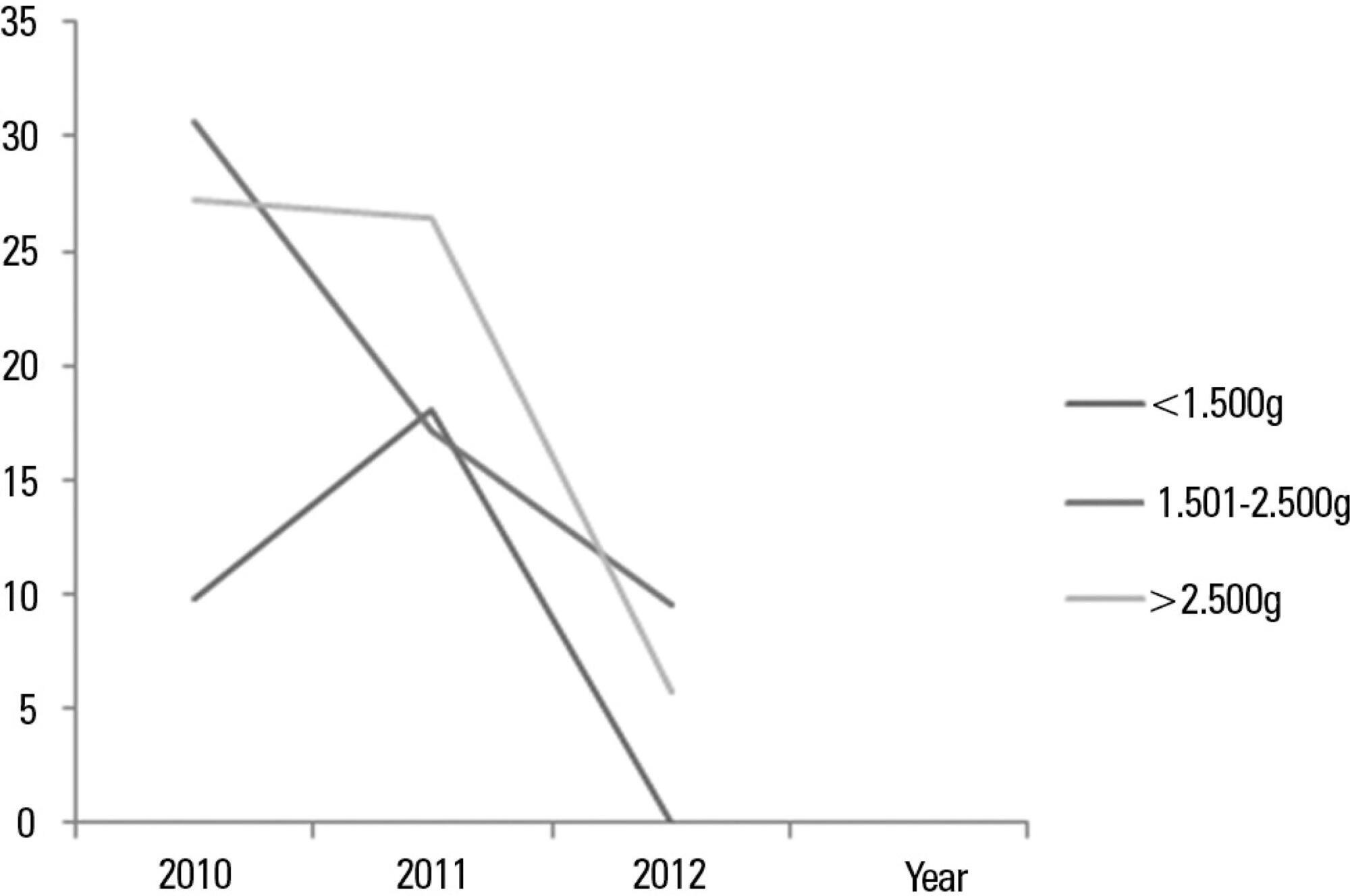
OBJECTIVE: To analyze the process of care provided to premature infants in a neonatal intensive care unit and the factors associated with their mortality. METHODS: Cross-sectional retrospective study of premature infants in an intensive care unit between 2008 and 2010. The characteristics of the mothers and premature infants were described, and a bivariate analysis was performed on the following characteristics: the study period and the "death" outcome (hospital, neonatal and early) using Pearson's chi-square test, Fisher's exact test or a chi-square test for linear trends. Bivariate and multivariable logistic regression analyses were performed using a stepwise backward logistic regression method between the variables with p<0.20 and the "death" outcome. A p value <0.05 was considered to be significant. RESULTS: In total, 293 preterm infants were studied. Increased access to complementary tests (transfontanellar ultrasound and Doppler echocardiogram) and breastfeeding rates were indicators of improving care. Mortality was concentrated in the neonatal period, especially in the early neonatal period, and was associated with extreme prematurity, small size for gestational age and an Apgar score <7 at 5 minutes after birth. The late-onset sepsis was also associated with a greater chance of neonatal death, and antenatal corticosteroids were protective against neonatal and early deaths. CONCLUSIONS: Although these results are comparable to previous findings regarding mortality among premature infants in Brazil, the study emphasizes the need to implement strategies that promote breastfeeding and reduce neonatal mortality and its early component.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):386-392
DOI 10.1590/S0103-507X2012000400016
OBJECTIVE: To analyze the process of care provided to premature infants in a neonatal intensive care unit and the factors associated with their mortality. METHODS: Cross-sectional retrospective study of premature infants in an intensive care unit between 2008 and 2010. The characteristics of the mothers and premature infants were described, and a bivariate analysis was performed on the following characteristics: the study period and the "death" outcome (hospital, neonatal and early) using Pearson's chi-square test, Fisher's exact test or a chi-square test for linear trends. Bivariate and multivariable logistic regression analyses were performed using a stepwise backward logistic regression method between the variables with p<0.20 and the "death" outcome. A p value <0.05 was considered to be significant. RESULTS: In total, 293 preterm infants were studied. Increased access to complementary tests (transfontanellar ultrasound and Doppler echocardiogram) and breastfeeding rates were indicators of improving care. Mortality was concentrated in the neonatal period, especially in the early neonatal period, and was associated with extreme prematurity, small size for gestational age and an Apgar score <7 at 5 minutes after birth. The late-onset sepsis was also associated with a greater chance of neonatal death, and antenatal corticosteroids were protective against neonatal and early deaths. CONCLUSIONS: Although these results are comparable to previous findings regarding mortality among premature infants in Brazil, the study emphasizes the need to implement strategies that promote breastfeeding and reduce neonatal mortality and its early component.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):239-244
DOI 10.5935/0103-507X.20130041
This study sought to evaluate infections related to health care caused by coagulase-negative Staphylococci in a neonatal intensive care unit by assessing antimicrobial susceptibility profiles and potentially effective antibiotic regimens.
This was a retrospective descriptive study performed on a case series of healthcare-associated infections, and the antimicrobial susceptibility profiles were evaluated. Newborns from other hospitals who were admitted to a neonatal intensive care unit in Rio de Janeiro between January 1, 2010, and June 30, 2012, were studied.
In total, 765 patients were admitted, totaling 3,051 patient-days, and the incidence density of general infection was 18.9 per 1,000 patient-days. The rate of central venous catheter use was 71.6%, and the positive culture rate for all sites and all infections related to health care were 68.4%. Coagulase-negative Staphylococci were identified in 11 (19.2%) of 57 health care-related infections, and infections with extended-spectrum beta-lactamase producing Klebsiella pneumoniae and Candida sp. constituted 5 cases each. Of the 11 cases of coagulase-negative Staphylococci, 10 (90.9%) were primary bloodstream infections. The sensitivity of the coagulase-negative Staphylococci isolates to vancomycin, clindamycin, ciprofloxacin, oxacillin and gentamycin was 100%, 81.8%, 72.7%, 27.2% and 22.2%, respectively. There were no deaths directly attributed to coagulase-negative Staphylococci infection.
Coagulase-negative Staphylococci was the main agent identified in healthcare-associated infections, with low rates of infections related to central venous catheter. In hospitals with a high oxacillin resistance profile, similar to those included in this study, vancomycin may be used as an initial therapy, although clindamycin represents a viable alternative.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):239-244
DOI 10.5935/0103-507X.20130041
This study sought to evaluate infections related to health care caused by coagulase-negative Staphylococci in a neonatal intensive care unit by assessing antimicrobial susceptibility profiles and potentially effective antibiotic regimens.
This was a retrospective descriptive study performed on a case series of healthcare-associated infections, and the antimicrobial susceptibility profiles were evaluated. Newborns from other hospitals who were admitted to a neonatal intensive care unit in Rio de Janeiro between January 1, 2010, and June 30, 2012, were studied.
In total, 765 patients were admitted, totaling 3,051 patient-days, and the incidence density of general infection was 18.9 per 1,000 patient-days. The rate of central venous catheter use was 71.6%, and the positive culture rate for all sites and all infections related to health care were 68.4%. Coagulase-negative Staphylococci were identified in 11 (19.2%) of 57 health care-related infections, and infections with extended-spectrum beta-lactamase producing Klebsiella pneumoniae and Candida sp. constituted 5 cases each. Of the 11 cases of coagulase-negative Staphylococci, 10 (90.9%) were primary bloodstream infections. The sensitivity of the coagulase-negative Staphylococci isolates to vancomycin, clindamycin, ciprofloxacin, oxacillin and gentamycin was 100%, 81.8%, 72.7%, 27.2% and 22.2%, respectively. There were no deaths directly attributed to coagulase-negative Staphylococci infection.
Coagulase-negative Staphylococci was the main agent identified in healthcare-associated infections, with low rates of infections related to central venous catheter. In hospitals with a high oxacillin resistance profile, similar to those included in this study, vancomycin may be used as an initial therapy, although clindamycin represents a viable alternative.
Abstract
Rev Bras Ter Intensiva. 2012;24(3):224-229
DOI 10.1590/S0103-507X2012000300004
OBJECTIVE: This study analyzed the factors that are associated with the need for packed red blood cell transfusions in premature infants in a neonatal intensive care unit. METHODS: This study is a cross-sectional study of secondary data from premature infants who were admitted to a neonatal intensive care unit between 2008 and 2010. Premature infants with low birth weight were included. Packed red blood cell transfusion was the dependent variable. Pearson's Chi-square or Fisher's exact tests were used for data analysis, and the median, minimum, and maximum values were calculated. Prevalence ratios were calculated using the Poisson regression and Pearson correlation coefficient. Linear regression analyses were performed. P < 0.05 was considered to be significant. RESULTS: We examined 254 premature infants, and 39.4% of this sample received packed red blood cells. Transfusions were 70% less prevalent in premature infants who were born at >32 weeks of gestation, and 191% more prevalent in infants who exhibited late-onset neonatal sepsis. The number of transfusions per patient was negatively correlated with gestational age and positively correlated with late-onset neonatal sepsis. A gestational age <32 weeks and late-onset neonatal sepsis explained 45% of the transfusions (p<0.0001). CONCLUSIONS: Premature infants with a gestational age <32 weeks and who developed late-onset neonatal sepsis exhibited a greater need for packed red blood cell transfusions.
Abstract
Rev Bras Ter Intensiva. 2012;24(3):224-229
DOI 10.1590/S0103-507X2012000300004
OBJECTIVE: This study analyzed the factors that are associated with the need for packed red blood cell transfusions in premature infants in a neonatal intensive care unit. METHODS: This study is a cross-sectional study of secondary data from premature infants who were admitted to a neonatal intensive care unit between 2008 and 2010. Premature infants with low birth weight were included. Packed red blood cell transfusion was the dependent variable. Pearson's Chi-square or Fisher's exact tests were used for data analysis, and the median, minimum, and maximum values were calculated. Prevalence ratios were calculated using the Poisson regression and Pearson correlation coefficient. Linear regression analyses were performed. P < 0.05 was considered to be significant. RESULTS: We examined 254 premature infants, and 39.4% of this sample received packed red blood cells. Transfusions were 70% less prevalent in premature infants who were born at >32 weeks of gestation, and 191% more prevalent in infants who exhibited late-onset neonatal sepsis. The number of transfusions per patient was negatively correlated with gestational age and positively correlated with late-onset neonatal sepsis. A gestational age <32 weeks and late-onset neonatal sepsis explained 45% of the transfusions (p<0.0001). CONCLUSIONS: Premature infants with a gestational age <32 weeks and who developed late-onset neonatal sepsis exhibited a greater need for packed red blood cell transfusions.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):119-129
DOI 10.1590/S0103-507X2012000200005
Developing guidelines for the role of the physiotherapist in neonatal and pediatric intensive care units is essential because these professionals are responsible for the rehabilitation of critically ill patients. Rehabilitation includes the evaluation and prevention of functional kinetic alterations, application of treatment interventions (respiratory and/or motor physiotherapy), control and application of medical gases, care of mechanical ventilation, weaning and extubation, tracheal gas insufflation, inflation/deflation of the endotracheal cuff protocol, and surfactant application, aiming to allow patients to have a full recovery and return to their functional activities. In this article, we present guidelines that are intended to guide the physiotherapist in some of the prevention/treatment interventions in respiratory therapy (airway clearance, lung expansion, position in bed, airway suction, drug inhalation, and cough assist), which help in the rehabilitation process of newborns and children in intensive care units during mechanical ventilation and up to 12 hours following extubation.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):119-129
DOI 10.1590/S0103-507X2012000200005
Developing guidelines for the role of the physiotherapist in neonatal and pediatric intensive care units is essential because these professionals are responsible for the rehabilitation of critically ill patients. Rehabilitation includes the evaluation and prevention of functional kinetic alterations, application of treatment interventions (respiratory and/or motor physiotherapy), control and application of medical gases, care of mechanical ventilation, weaning and extubation, tracheal gas insufflation, inflation/deflation of the endotracheal cuff protocol, and surfactant application, aiming to allow patients to have a full recovery and return to their functional activities. In this article, we present guidelines that are intended to guide the physiotherapist in some of the prevention/treatment interventions in respiratory therapy (airway clearance, lung expansion, position in bed, airway suction, drug inhalation, and cough assist), which help in the rehabilitation process of newborns and children in intensive care units during mechanical ventilation and up to 12 hours following extubation.