Intensive care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2012;24(3):252-257
DOI 10.1590/S0103-507X2012000300008
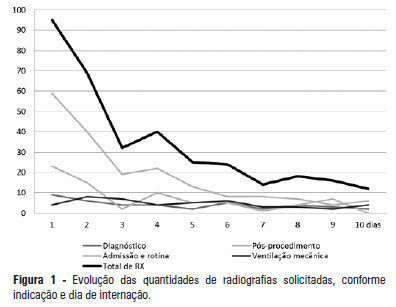
OBJECTIVE: This study determined the prevalence of clinical abnormalities in chest radiographs and its relationship with decision-making in intensive care. METHODS: This prospective cohort study involved nonconsecutive patients who were admitted to the intensive care unit at the Hospital Universitário Professor Polydoro Ernani de São Thiago of the Universidade Federal de Santa Catarina. Imaging tests in the intensive care unit (ICU) were assessed daily between February and May 2011 and divided according to the reason for hospitalization, the type of test requested, anatomical segment under assessment and the purpose of the request. The imaging tests were interpreted by intensivists and subsequently divided according to the detected abnormalities and changes in medical care. The chi-squared test was used for statistical analysis. RESULTS: The study sample included 106 patients. A total of 447 imaging tests were assessed, 425 of which were anteroposterior chest radiographs. An average of 4.01 radiographs per patient was obtained. Among the requested radiographs, 79.3% were normal, and 35.2% of abnormal radiographs did not prompt changes in medical care. CONCLUSION: Most of the radiographs performed in the intensive care unit exhibited no statistically significant clinical alterations, and the radiographs that revealed abnormalities did not necessarily lead to changes in medical care.
Abstract
Rev Bras Ter Intensiva. 2012;24(3):252-257
DOI 10.1590/S0103-507X2012000300008
OBJECTIVE: This study determined the prevalence of clinical abnormalities in chest radiographs and its relationship with decision-making in intensive care. METHODS: This prospective cohort study involved nonconsecutive patients who were admitted to the intensive care unit at the Hospital Universitário Professor Polydoro Ernani de São Thiago of the Universidade Federal de Santa Catarina. Imaging tests in the intensive care unit (ICU) were assessed daily between February and May 2011 and divided according to the reason for hospitalization, the type of test requested, anatomical segment under assessment and the purpose of the request. The imaging tests were interpreted by intensivists and subsequently divided according to the detected abnormalities and changes in medical care. The chi-squared test was used for statistical analysis. RESULTS: The study sample included 106 patients. A total of 447 imaging tests were assessed, 425 of which were anteroposterior chest radiographs. An average of 4.01 radiographs per patient was obtained. Among the requested radiographs, 79.3% were normal, and 35.2% of abnormal radiographs did not prompt changes in medical care. CONCLUSION: Most of the radiographs performed in the intensive care unit exhibited no statistically significant clinical alterations, and the radiographs that revealed abnormalities did not necessarily lead to changes in medical care.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):151-156
DOI 10.1590/S0103-507X2012000200009
OBJECTIVE:To characterize drug prescriptions in a university hospital adult intensive care unit. METHODS: Single-center, observational, descriptive, cross-sectional study conducted at an adult general intensive care unit. The study population included all of the unit's inpatients from January to March 2011. The following characteristics for all prescriptions recorded during this period were examined: drug name (generic, brand name or abbreviation), dosage strength, pharmaceutical form, dose, route of administration, patient name, patient registration in the institution, clinic and hospital bed as well as the name, board license number, signature of the prescriber and date of the prescription. It was quantified the percentage of prescribed drugs included in the National List of Essential Drugs, the World Health Organization Model List of Essential Medicines and the University Hospital Center Pharmacotherapy Guide. The prescribed drugs were classified based on the Anatomical Therapeutic Chemical classification system (levels 1 and 2). RESULTS: Eight hundred forty-four prescriptions were reviewed from 72 patients (mean age: 59.04 ± 21.80), 54.92% of whom were female. The mean number of prescriptions per patient was 11.72 ± 11.68. The total number of drugs prescribed was 12,052 and 9,571 (79.41%) of the drugs were prescribed using the generic name. The most frequent absent information in the drug description was the pharmaceutical form of the drug (8,829/73.26%). The dosage strength was indicated in 7,231 (60%) of the prescriptions, and the prescriber and patient information were indicated in over 96% of the prescriptions. The prescribed drugs were classified in 13 therapeutic groups and 55 subgroups. Systemic antibacterials represented one of the most frequently prescribed subgroups. CONCLUSION: Most of the reviewed information was present in the prescriptions. However, the dosage strength and pharmaceutical form were absent in many prescriptions. The characterization of prescriptions at different hospital units is essential for the development of strategies that reduce drug utilization problems.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):151-156
DOI 10.1590/S0103-507X2012000200009
OBJECTIVE:To characterize drug prescriptions in a university hospital adult intensive care unit. METHODS: Single-center, observational, descriptive, cross-sectional study conducted at an adult general intensive care unit. The study population included all of the unit's inpatients from January to March 2011. The following characteristics for all prescriptions recorded during this period were examined: drug name (generic, brand name or abbreviation), dosage strength, pharmaceutical form, dose, route of administration, patient name, patient registration in the institution, clinic and hospital bed as well as the name, board license number, signature of the prescriber and date of the prescription. It was quantified the percentage of prescribed drugs included in the National List of Essential Drugs, the World Health Organization Model List of Essential Medicines and the University Hospital Center Pharmacotherapy Guide. The prescribed drugs were classified based on the Anatomical Therapeutic Chemical classification system (levels 1 and 2). RESULTS: Eight hundred forty-four prescriptions were reviewed from 72 patients (mean age: 59.04 ± 21.80), 54.92% of whom were female. The mean number of prescriptions per patient was 11.72 ± 11.68. The total number of drugs prescribed was 12,052 and 9,571 (79.41%) of the drugs were prescribed using the generic name. The most frequent absent information in the drug description was the pharmaceutical form of the drug (8,829/73.26%). The dosage strength was indicated in 7,231 (60%) of the prescriptions, and the prescriber and patient information were indicated in over 96% of the prescriptions. The prescribed drugs were classified in 13 therapeutic groups and 55 subgroups. Systemic antibacterials represented one of the most frequently prescribed subgroups. CONCLUSION: Most of the reviewed information was present in the prescriptions. However, the dosage strength and pharmaceutical form were absent in many prescriptions. The characterization of prescriptions at different hospital units is essential for the development of strategies that reduce drug utilization problems.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):162-166
DOI 10.1590/S0103-507X2012000200011
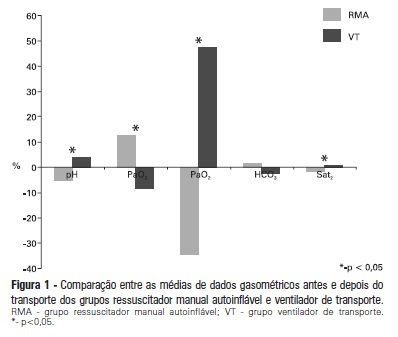
OBJECTIVE: To evaluate the effects on blood gases by two methods of ventilation (with transport ventilation or self-inflating manual resuscitator) during intra-hospital transport of patients after cardiac surgery. METHODS: Observational, longitudinal, prospective, randomized study. Two samples of arterial blood were collected at the end of the surgery and another at the end of patient transport. RESULTS: We included 23 patients: 13 in the Group with transport ventilation and 10 in the Group with self-inflating manual resuscitator. Baseline characteristics were similar between both groups, except for higher acute severity of illness in the Group with transport ventilation. We observed significant differences in comparisons of percentage variations of gasometric data: pH (transport ventilation + 4% x MR -5%, p=0.007), PaCO2 (-8% x +13%, p=0.006), PaO2 (+47% x -34%, p=0.01) and SatO2 (+0.6% x -1.7%, p=0.001). CONCLUSION: The use of mechanical ventilation results in fewer repercussions for blood gas analysis in the intra-hospital transport of cardiac surgery patients.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):162-166
DOI 10.1590/S0103-507X2012000200011
OBJECTIVE: To evaluate the effects on blood gases by two methods of ventilation (with transport ventilation or self-inflating manual resuscitator) during intra-hospital transport of patients after cardiac surgery. METHODS: Observational, longitudinal, prospective, randomized study. Two samples of arterial blood were collected at the end of the surgery and another at the end of patient transport. RESULTS: We included 23 patients: 13 in the Group with transport ventilation and 10 in the Group with self-inflating manual resuscitator. Baseline characteristics were similar between both groups, except for higher acute severity of illness in the Group with transport ventilation. We observed significant differences in comparisons of percentage variations of gasometric data: pH (transport ventilation + 4% x MR -5%, p=0.007), PaCO2 (-8% x +13%, p=0.006), PaO2 (+47% x -34%, p=0.01) and SatO2 (+0.6% x -1.7%, p=0.001). CONCLUSION: The use of mechanical ventilation results in fewer repercussions for blood gas analysis in the intra-hospital transport of cardiac surgery patients.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):106-110
DOI 10.1590/S0103-507X2012000100016
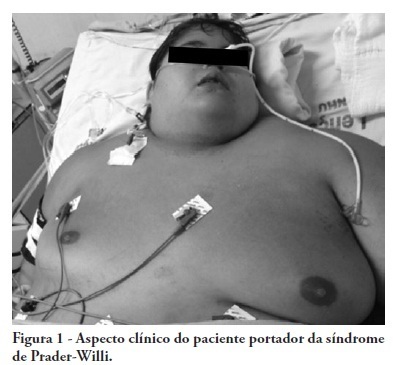
Prader-Willi syndrome is a genetic neurobehavioral disease affecting children's development and resulting in obesity, reduced height, hypotonia, endocrine disorders and cognitive deficits, which may impair oral integrity. This study aims to report on a case involving a white male 15-year-old patient with Prader-Willi syndrome whose oral examination revealed bacterial plaque, gingivitis, poor occlusion, viscous salivation and multiple lip, jugal mucosa, inserted gum and tongue ulcerations. An excision biopsy revealed oral ulcerations typical of herpes, which were considered to be likely to correlate with herpes encephalitis. This result demonstrates that a large portion of the deleterious effects of Prader-Willi syndrome can be attenuated by appropriate diagnosis and early therapeutic intervention, highlighting the role of an integrated multidisciplinary team in the development of therapeutic protocols for Prader-Willi syndrome patients.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):106-110
DOI 10.1590/S0103-507X2012000100016
Prader-Willi syndrome is a genetic neurobehavioral disease affecting children's development and resulting in obesity, reduced height, hypotonia, endocrine disorders and cognitive deficits, which may impair oral integrity. This study aims to report on a case involving a white male 15-year-old patient with Prader-Willi syndrome whose oral examination revealed bacterial plaque, gingivitis, poor occlusion, viscous salivation and multiple lip, jugal mucosa, inserted gum and tongue ulcerations. An excision biopsy revealed oral ulcerations typical of herpes, which were considered to be likely to correlate with herpes encephalitis. This result demonstrates that a large portion of the deleterious effects of Prader-Willi syndrome can be attenuated by appropriate diagnosis and early therapeutic intervention, highlighting the role of an integrated multidisciplinary team in the development of therapeutic protocols for Prader-Willi syndrome patients.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):448-454
DOI 10.1590/S0103-507X2011000400009
OBJECTIVES: This study aimed to assess family member acceptance of orthotanasia as related to symptom management, patient preference and the influence of the medical team's communication on therapy. METHODS: This was a descriptive one-year study conducted at the adult intensive care unit of the Hospital do Servidor Público Estadual. A structured questionnaire based on the Quality of Dying and Death (QODD 22) instrument and prior informal interviews were used. RESULTS: Sixty family members were assessed; the mean age was 51.7 + 12.1 years, and 81.7% were female. The patients were hospitalized for a mean of 31 + 26.9 days, and 17.0% of these days were spent in the intensive care unit. Most of the patients had neurological conditions. Most of the patients (53.3%) had discussed their end-of-life care wishes with family members; however, 76.7% of them had not discussed this issue with their doctors (p < 0.00). The family members reported being favorable to orthotanasia in 83.3% of the cases. Most (85.0%) desired the medical team to clearly approach the subject, and 65.0% wished to take part in the quality of end-of-life decision making process. The family members were generally satisfied with information they received from the doctors: 93.3% believed they had received appropriately frequent communications about the clinical conditions; 81.7% were able to clarify their doubts regarding the patient's clinical status; the communication was understood by 83.3% of the respondents; and 80.0% believed that clear and honest information had been provided. Only 43.3% of the respondents wished to be present at the time of their loved ones' deaths. A significant association between family member acceptance of orthotanasia and participation in end-of-life decisions (p = 0.042) was observed. CONCLUSIONS: Most of the respondents were favorable to orthotanasia and wished to participate in end-of-life discussions.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):448-454
DOI 10.1590/S0103-507X2011000400009
OBJECTIVES: This study aimed to assess family member acceptance of orthotanasia as related to symptom management, patient preference and the influence of the medical team's communication on therapy. METHODS: This was a descriptive one-year study conducted at the adult intensive care unit of the Hospital do Servidor Público Estadual. A structured questionnaire based on the Quality of Dying and Death (QODD 22) instrument and prior informal interviews were used. RESULTS: Sixty family members were assessed; the mean age was 51.7 + 12.1 years, and 81.7% were female. The patients were hospitalized for a mean of 31 + 26.9 days, and 17.0% of these days were spent in the intensive care unit. Most of the patients had neurological conditions. Most of the patients (53.3%) had discussed their end-of-life care wishes with family members; however, 76.7% of them had not discussed this issue with their doctors (p < 0.00). The family members reported being favorable to orthotanasia in 83.3% of the cases. Most (85.0%) desired the medical team to clearly approach the subject, and 65.0% wished to take part in the quality of end-of-life decision making process. The family members were generally satisfied with information they received from the doctors: 93.3% believed they had received appropriately frequent communications about the clinical conditions; 81.7% were able to clarify their doubts regarding the patient's clinical status; the communication was understood by 83.3% of the respondents; and 80.0% believed that clear and honest information had been provided. Only 43.3% of the respondents wished to be present at the time of their loved ones' deaths. A significant association between family member acceptance of orthotanasia and participation in end-of-life decisions (p = 0.042) was observed. CONCLUSIONS: Most of the respondents were favorable to orthotanasia and wished to participate in end-of-life discussions.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):462-469
DOI 10.1590/S0103-507X2011000400011
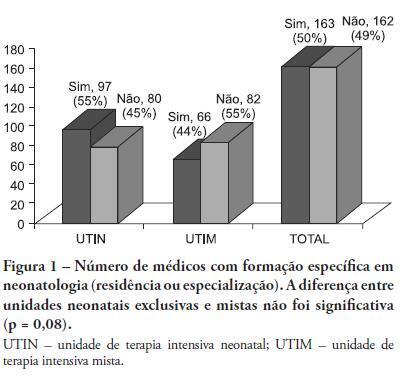
OBJECTIVE: This study described the sociodemographic profile and professional qualifications of pediatric intensive care physicians in the State of Rio de Janeiro (RJ), southeastern Brazil. METHODS: This investigation was an observational, cross-sectional and descriptive study that was conducted in neonatal, pediatric and mixed intensive care units in the State of Rio de Janeiro. Physicians working in the participating intensive care units voluntarily completed a semistructured and anonymous questionnaire. Questionnaires that were not returned within 30 days were considered lost, and questionnaires with less than 75% questions completed were excluded. The differences in neonatal and pediatric intensive care physicians' medical training were compared using the Chi-squared test with a 5% significance level. RESULTS: A total of 410 physicians were included in this study: 84% female, 48% between 30 and 39 years old and 45% with monthly incomes between US $1,700 to 2,700. Forty percent of these physicians worked exclusively in this specialty, and 72% worked in more than one intensive care unit. Only 50% of the participants had received specific training (either medical residency or specialization) in neonatology, and only 33% were board-certified specialists in this area. Only 27% of the physicians had received specific training in pediatric intensive care medicine, and only 17% were board-certified specialists (p < 0.0005 for both comparisons). Most (87%) physicians had participated in scientific events within the past 5 years, and 55% used the internet for continued medical education. However, only 25% had participated in any research. Most (63%) physicians were dissatisfied with their professional activity; 49% were dissatisfied due to working conditions, 23% due to low incomes and 18% due to training-related issues. CONCLUSION: These results suggested that the medical qualifications of neonatal and pediatric intensive care physicians in the State of Rio de Janeiro, Brazil are inadequate, especially in pediatric intensive care medicine. A high level of dissatisfaction was reported, which may jeopardize the quality of medical assistance that is provided by these professionals.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):462-469
DOI 10.1590/S0103-507X2011000400011
OBJECTIVE: This study described the sociodemographic profile and professional qualifications of pediatric intensive care physicians in the State of Rio de Janeiro (RJ), southeastern Brazil. METHODS: This investigation was an observational, cross-sectional and descriptive study that was conducted in neonatal, pediatric and mixed intensive care units in the State of Rio de Janeiro. Physicians working in the participating intensive care units voluntarily completed a semistructured and anonymous questionnaire. Questionnaires that were not returned within 30 days were considered lost, and questionnaires with less than 75% questions completed were excluded. The differences in neonatal and pediatric intensive care physicians' medical training were compared using the Chi-squared test with a 5% significance level. RESULTS: A total of 410 physicians were included in this study: 84% female, 48% between 30 and 39 years old and 45% with monthly incomes between US $1,700 to 2,700. Forty percent of these physicians worked exclusively in this specialty, and 72% worked in more than one intensive care unit. Only 50% of the participants had received specific training (either medical residency or specialization) in neonatology, and only 33% were board-certified specialists in this area. Only 27% of the physicians had received specific training in pediatric intensive care medicine, and only 17% were board-certified specialists (p < 0.0005 for both comparisons). Most (87%) physicians had participated in scientific events within the past 5 years, and 55% used the internet for continued medical education. However, only 25% had participated in any research. Most (63%) physicians were dissatisfied with their professional activity; 49% were dissatisfied due to working conditions, 23% due to low incomes and 18% due to training-related issues. CONCLUSION: These results suggested that the medical qualifications of neonatal and pediatric intensive care physicians in the State of Rio de Janeiro, Brazil are inadequate, especially in pediatric intensive care medicine. A high level of dissatisfaction was reported, which may jeopardize the quality of medical assistance that is provided by these professionals.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):68-77
DOI 10.1590/S0103-507X2011000100012
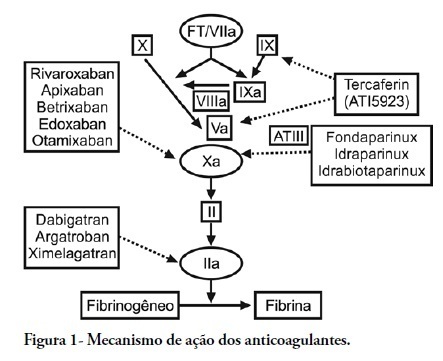
Thromboembolic events commonly occur in critically ill patients, and although they do not consistently present with specific signs and symptoms, they are associated with high morbity and mortality. Antithrombotic agents are the mainstay of the prevention and treatment of venous thromboembolism, and they are also used for stroke prevention in atrial fibrillation, embolism prevention in heart failure, and anticoagulation of prosthetic valves. These drugs have been combined with antiplatelet therapy for the prevention of secondary acute coronary syndrome. Antithrombotic agents such as Aspirin, clopidogrel, vitamin K antagonists and fondaparinux, an indirect Factor Xa inhibitor, are already incorporated into our clinical practice. New small-molecule, selective Factor Xa and thrombin inhibitors that simultaneously inhibit free plasma and clot-associated factor activities have received considerable attention recently. These new oral anticoagulants are in various phases of clinical development. dabigatran, rivaroxaban and apixaban are in more advanced phases of clinical development and are already available in a number of countries. This review article highlights the studies describing the use of these three anticoagulants in an intensive care setting.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):68-77
DOI 10.1590/S0103-507X2011000100012
Thromboembolic events commonly occur in critically ill patients, and although they do not consistently present with specific signs and symptoms, they are associated with high morbity and mortality. Antithrombotic agents are the mainstay of the prevention and treatment of venous thromboembolism, and they are also used for stroke prevention in atrial fibrillation, embolism prevention in heart failure, and anticoagulation of prosthetic valves. These drugs have been combined with antiplatelet therapy for the prevention of secondary acute coronary syndrome. Antithrombotic agents such as Aspirin, clopidogrel, vitamin K antagonists and fondaparinux, an indirect Factor Xa inhibitor, are already incorporated into our clinical practice. New small-molecule, selective Factor Xa and thrombin inhibitors that simultaneously inhibit free plasma and clot-associated factor activities have received considerable attention recently. These new oral anticoagulants are in various phases of clinical development. dabigatran, rivaroxaban and apixaban are in more advanced phases of clinical development and are already available in a number of countries. This review article highlights the studies describing the use of these three anticoagulants in an intensive care setting.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):291-299
DOI 10.1590/S0103-507X2010000300012
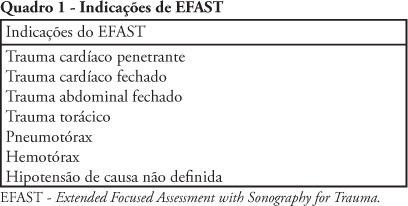
Trauma is the leading cause of death in people below 45 years-old in Brazil, and responsible for one third of all intensive care unit admissions. The increasing knowledge on ultrasound diagnosis methods and its availability for life-threatening injuries (such as cardiac tamponade and abdominal cavity solid organs rupture leading to hemorrhagic shock) diagnosis and monitoring, lead to the development o the FAST (Focused Assessment with Sonography for Trauma) protocol, aimed to be used both in the emergency and intensive care unit settings. Due to its reproducibility, lack of radiation exposure, and bedside feasibility, this technology is being increasingly accepted. A new protocol extension, the Extended-FAST, provides valuable information for improved patients' management, extending its availability from the abdominal conditions to other diagnosis such as hemothorax, pleural effusion and pneumothorax. We must underline that this technique is able to replace computed tomography and diagnostic peritoneal wash, and do not delay surgical procedure instead of perform this exam . Thus, its careful appraisal in connection with the clinical information should guide the therapeutic approaches, specially in inhospitable sites such as intensive care units in war zones, rural or distant places, were other imagery methods are not available.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):291-299
DOI 10.1590/S0103-507X2010000300012
Trauma is the leading cause of death in people below 45 years-old in Brazil, and responsible for one third of all intensive care unit admissions. The increasing knowledge on ultrasound diagnosis methods and its availability for life-threatening injuries (such as cardiac tamponade and abdominal cavity solid organs rupture leading to hemorrhagic shock) diagnosis and monitoring, lead to the development o the FAST (Focused Assessment with Sonography for Trauma) protocol, aimed to be used both in the emergency and intensive care unit settings. Due to its reproducibility, lack of radiation exposure, and bedside feasibility, this technology is being increasingly accepted. A new protocol extension, the Extended-FAST, provides valuable information for improved patients' management, extending its availability from the abdominal conditions to other diagnosis such as hemothorax, pleural effusion and pneumothorax. We must underline that this technique is able to replace computed tomography and diagnostic peritoneal wash, and do not delay surgical procedure instead of perform this exam . Thus, its careful appraisal in connection with the clinical information should guide the therapeutic approaches, specially in inhospitable sites such as intensive care units in war zones, rural or distant places, were other imagery methods are not available.