Hypnotics and sedatives Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(4):507-518
DOI 10.5935/0103-507X.20220145-en
To verify strategies for the prevention and treatment of abstinence syndrome in a pediatric intensive care unit.
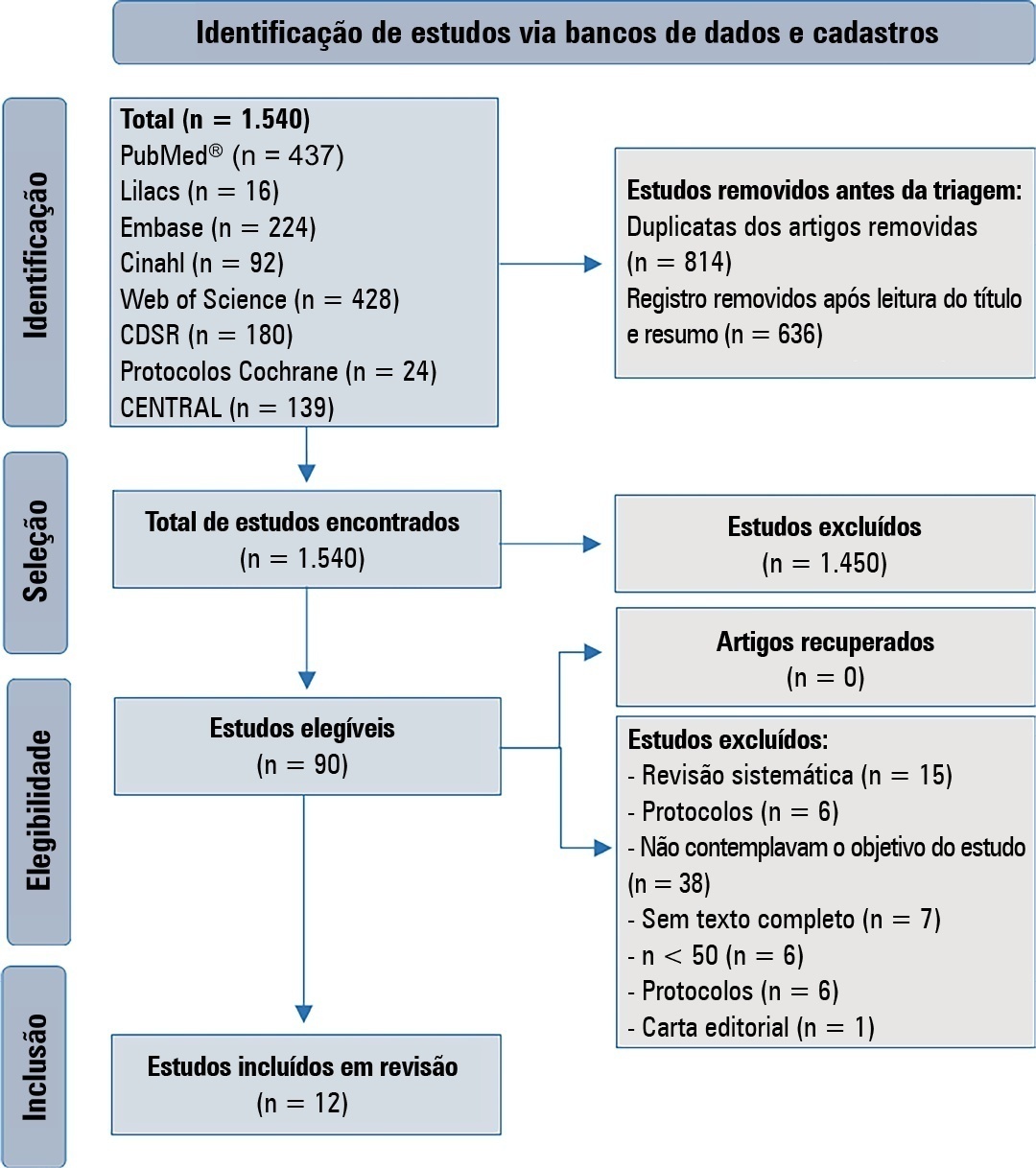
This is a systematic review in the PubMed database®, Lilacs, Embase, Web of Science, Cochrane, Cinahl, Cochrane Database Systematic Review and CENTRAL. A three-step search strategy was used for this review, and the protocol was approved in PROSPERO (CRD42021274670).
Twelve articles were included in the analysis. There was great heterogeneity among the studies included, especially regarding the therapeutic regimens used for sedation and analgesia. Midazolam doses ranged from 0.05mg/kg/hour to 0.3mg/kg/hour. Morphine also varied considerably, from 10mcg/kg/hour to 30mcg/kg/hour, between studies. Among the 12 selected studies, the most commonly used scale for the identification of withdrawal symptoms was the Sophia Observational Withdrawal Symptoms Scale. In three studies, there was a statistically significant difference in the prevention and management of the withdrawal syndrome due to the implementation of different protocols (p < 0.01 and p < 0.001).
There was great variation in the sedoanalgesia regimen used by the studies and the method of weaning and evaluation of withdrawal syndrome. More studies are needed to provide more robust evidence about the most appropriate treatment for the prevention and reduction of withdrawal signs and symptoms in critically ill children.
CRD 42021274670
Abstract
Rev Bras Ter Intensiva. 2022;34(4):507-518
DOI 10.5935/0103-507X.20220145-en
To verify strategies for the prevention and treatment of abstinence syndrome in a pediatric intensive care unit.
This is a systematic review in the PubMed database®, Lilacs, Embase, Web of Science, Cochrane, Cinahl, Cochrane Database Systematic Review and CENTRAL. A three-step search strategy was used for this review, and the protocol was approved in PROSPERO (CRD42021274670).
Twelve articles were included in the analysis. There was great heterogeneity among the studies included, especially regarding the therapeutic regimens used for sedation and analgesia. Midazolam doses ranged from 0.05mg/kg/hour to 0.3mg/kg/hour. Morphine also varied considerably, from 10mcg/kg/hour to 30mcg/kg/hour, between studies. Among the 12 selected studies, the most commonly used scale for the identification of withdrawal symptoms was the Sophia Observational Withdrawal Symptoms Scale. In three studies, there was a statistically significant difference in the prevention and management of the withdrawal syndrome due to the implementation of different protocols (p < 0.01 and p < 0.001).
There was great variation in the sedoanalgesia regimen used by the studies and the method of weaning and evaluation of withdrawal syndrome. More studies are needed to provide more robust evidence about the most appropriate treatment for the prevention and reduction of withdrawal signs and symptoms in critically ill children.
CRD 42021274670
Abstract
Rev Bras Ter Intensiva. 2020;32(3):433-438
DOI 10.5935/0103-507X.20200073
To describe the use of neuromuscular blockade as well as other practices among Brazilian physicians in adult intensive care units.
An online national survey was designed and administered to Brazilian intensivists. Questions were selected using the Delphi method and assessed physicians’ demographic data, intensive care unit characteristics, practices regarding airway management, use of neuromuscular blockade and sedation during endotracheal intubation in the intensive care unit. As a secondary outcome, we applied a multivariate analysis to evaluate factors associated with the use of neuromuscular blockade.
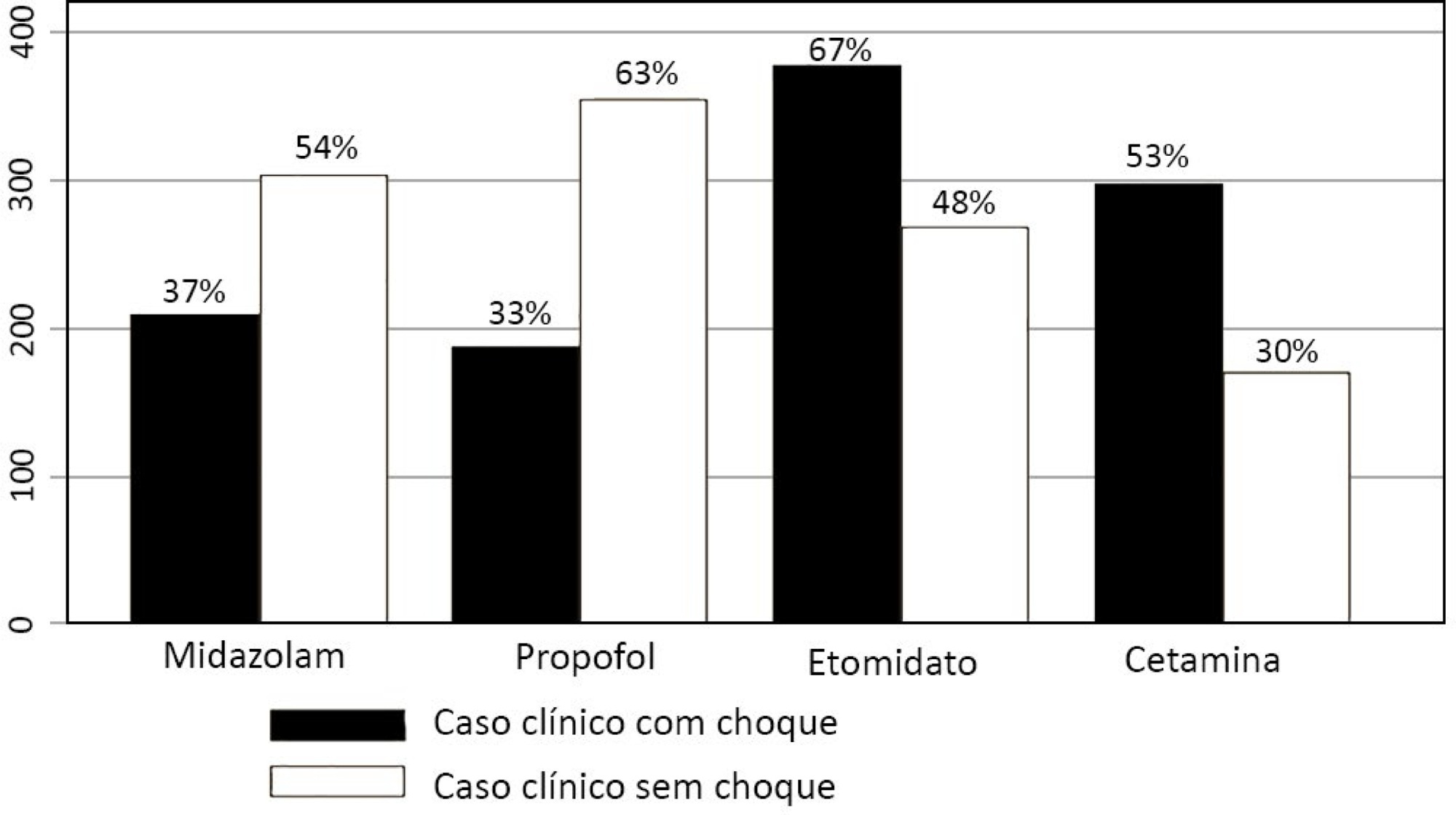
Five hundred sixty-five intensivists from all Brazilian regions responded to the questionnaire. The majority of respondents were male (65%), with a mean age of 38 ( 8.4 years, and 58.5% had a board certification in critical care. Only 40.7% of the intensivists reported the use of neuromuscular blockade during all or in more than 75% of endotracheal intubations. In the multivariate analysis, the number of intubations performed monthly and physician specialization in anesthesiology were directly associated with frequent use of neuromuscular blockade. Etomidate and ketamine were more commonly used in the clinical situation of hypotension and shock, while propofol and midazolam were more commonly prescribed in the situation of clinical stability.
The reported use of neuromuscular blockade was low among intensivists, and sedative drugs were chosen in accordance with patient hemodynamic stability. These results may help the design of future studies regarding airway management in Brazil.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):433-438
DOI 10.5935/0103-507X.20200073
To describe the use of neuromuscular blockade as well as other practices among Brazilian physicians in adult intensive care units.
An online national survey was designed and administered to Brazilian intensivists. Questions were selected using the Delphi method and assessed physicians’ demographic data, intensive care unit characteristics, practices regarding airway management, use of neuromuscular blockade and sedation during endotracheal intubation in the intensive care unit. As a secondary outcome, we applied a multivariate analysis to evaluate factors associated with the use of neuromuscular blockade.
Five hundred sixty-five intensivists from all Brazilian regions responded to the questionnaire. The majority of respondents were male (65%), with a mean age of 38 ( 8.4 years, and 58.5% had a board certification in critical care. Only 40.7% of the intensivists reported the use of neuromuscular blockade during all or in more than 75% of endotracheal intubations. In the multivariate analysis, the number of intubations performed monthly and physician specialization in anesthesiology were directly associated with frequent use of neuromuscular blockade. Etomidate and ketamine were more commonly used in the clinical situation of hypotension and shock, while propofol and midazolam were more commonly prescribed in the situation of clinical stability.
The reported use of neuromuscular blockade was low among intensivists, and sedative drugs were chosen in accordance with patient hemodynamic stability. These results may help the design of future studies regarding airway management in Brazil.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):15-20
DOI 10.5935/0103-507X.20190003
To describe the incidence of clinical and non-clinical events during intrahospital transport of critically ill patients and to analyze the associated risk factors.
Cohort study with retrospective data collected from October 2016 to October 2017. All cases of intrahospital transport for diagnostic and therapeutic purposes in a large hospital with six adult intensive care units were analyzed, and the adverse events and related risk factors were evaluated.
During the study period, 1,559 intrahospital transports were performed with 1,348 patients, with a mean age of 66 ± 17 years and a mean transport time of 43 ± 34 minutes. During transport, 19.8% of the patients were using vasoactive drugs; 13.7% were under sedation; and 10.6% were under mechanical ventilation. Clinical events occurred in 117 transports (7.5%), and non-clinical events occurred in 125 (8.0%) transports. Communication failures were prevalent; however, the multivariate analysis showed that the use of sedatives, noradrenaline and nitroprusside and a transport time greater than 36.5 minutes were associated with adverse clinical events. The use of dobutamine and a transport time greater than 36.5 minutes were associated with non-clinical events. At the end of transport, 98.1% of the patients presented unchanged clinical conditions compared with baseline.
Intrahospital transport is related to a high incidence of adverse events, and transport time and the use of sedatives and vasoactive drugs were related to these events.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):15-20
DOI 10.5935/0103-507X.20190003
To describe the incidence of clinical and non-clinical events during intrahospital transport of critically ill patients and to analyze the associated risk factors.
Cohort study with retrospective data collected from October 2016 to October 2017. All cases of intrahospital transport for diagnostic and therapeutic purposes in a large hospital with six adult intensive care units were analyzed, and the adverse events and related risk factors were evaluated.
During the study period, 1,559 intrahospital transports were performed with 1,348 patients, with a mean age of 66 ± 17 years and a mean transport time of 43 ± 34 minutes. During transport, 19.8% of the patients were using vasoactive drugs; 13.7% were under sedation; and 10.6% were under mechanical ventilation. Clinical events occurred in 117 transports (7.5%), and non-clinical events occurred in 125 (8.0%) transports. Communication failures were prevalent; however, the multivariate analysis showed that the use of sedatives, noradrenaline and nitroprusside and a transport time greater than 36.5 minutes were associated with adverse clinical events. The use of dobutamine and a transport time greater than 36.5 minutes were associated with non-clinical events. At the end of transport, 98.1% of the patients presented unchanged clinical conditions compared with baseline.
Intrahospital transport is related to a high incidence of adverse events, and transport time and the use of sedatives and vasoactive drugs were related to these events.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):344-348
DOI 10.1590/S0103-507X2008000400005
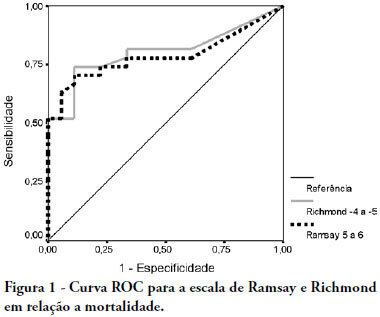
OBJECTIVE: The main purpose of this study was to compare performance of the Ramsay and Richmond sedation scores on mechanically ventilated critically ill patients, in a university-affiliated hospital. METHODS: This was a 4-month prospective study, which included a total of 45 patients mechanically ventilated, with at least 48 hours stay in the intensive care unit. Each patient was assessed daily for sedation mode, sedative and analgesic doses and sedation level using the Ramsay and Richmond scores. Statistical analysis was made using Student's t-test, Pearson's and Spearman's correlation, and constructing ROC-curves. RESULTS: A high general mortality of 60% was observed. The length of sedation and daily dose of medication did not correlate with mortality. Deep sedation (Ramsay > 4 or Richmond < -3) was positively correlated with probability of death with an AUC > 0.78. An adequate level of sedation (Ramsay 2 to 4 or Richmond 0 to -3) was sensitively correlated with probability of survival with an AUC > 0.80. A low level of sedation was observed in 63 days evaluated (8.64%), and no correlation was found between occurrence of agitation and unfavorable outcomes. Correlation between Ramsay and Richmond scores (Pearson's > 0.810 - p<0.0001) was good. CONCLUSION: In this study, Ramsay and Richmond sedation scores were similar for the assessment of deep, insufficient and adequate sedation. Both have good correlation with mortality in over sedated patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):344-348
DOI 10.1590/S0103-507X2008000400005
OBJECTIVE: The main purpose of this study was to compare performance of the Ramsay and Richmond sedation scores on mechanically ventilated critically ill patients, in a university-affiliated hospital. METHODS: This was a 4-month prospective study, which included a total of 45 patients mechanically ventilated, with at least 48 hours stay in the intensive care unit. Each patient was assessed daily for sedation mode, sedative and analgesic doses and sedation level using the Ramsay and Richmond scores. Statistical analysis was made using Student's t-test, Pearson's and Spearman's correlation, and constructing ROC-curves. RESULTS: A high general mortality of 60% was observed. The length of sedation and daily dose of medication did not correlate with mortality. Deep sedation (Ramsay > 4 or Richmond < -3) was positively correlated with probability of death with an AUC > 0.78. An adequate level of sedation (Ramsay 2 to 4 or Richmond 0 to -3) was sensitively correlated with probability of survival with an AUC > 0.80. A low level of sedation was observed in 63 days evaluated (8.64%), and no correlation was found between occurrence of agitation and unfavorable outcomes. Correlation between Ramsay and Richmond scores (Pearson's > 0.810 - p<0.0001) was good. CONCLUSION: In this study, Ramsay and Richmond sedation scores were similar for the assessment of deep, insufficient and adequate sedation. Both have good correlation with mortality in over sedated patients.