Extracorporeal membrane oxygenation Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2018;30(2):233-236
DOI 10.5935/0103-507X.20180029
We report the case of a female patient, 58 years of age, without known heart disease, who underwent liver transplantation without complications. On the second postoperative day, the patient developed cardiogenic shock secondary to stress-induced cardiomyopathy (Takotsubo-like syndrome). The patient was successfully managed with veno-arterial peripheral extracorporeal membrane oxygenation for 6 days, with complete recovery of cardiac function and of the hepatic graft. Coronary syndrome and acute myocarditis were excluded as the causes of the shock. The use of extracorporeal membrane oxygenation in this scenario is possible and safe, considering its specialized protocols and treatment.
Abstract
Rev Bras Ter Intensiva. 2018;30(2):233-236
DOI 10.5935/0103-507X.20180029
We report the case of a female patient, 58 years of age, without known heart disease, who underwent liver transplantation without complications. On the second postoperative day, the patient developed cardiogenic shock secondary to stress-induced cardiomyopathy (Takotsubo-like syndrome). The patient was successfully managed with veno-arterial peripheral extracorporeal membrane oxygenation for 6 days, with complete recovery of cardiac function and of the hepatic graft. Coronary syndrome and acute myocarditis were excluded as the causes of the shock. The use of extracorporeal membrane oxygenation in this scenario is possible and safe, considering its specialized protocols and treatment.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):317-326
DOI 10.5935/0103-507X.20180052
To characterize the transport of severely ill patients with extracorporeal respiratory or cardiovascular support.
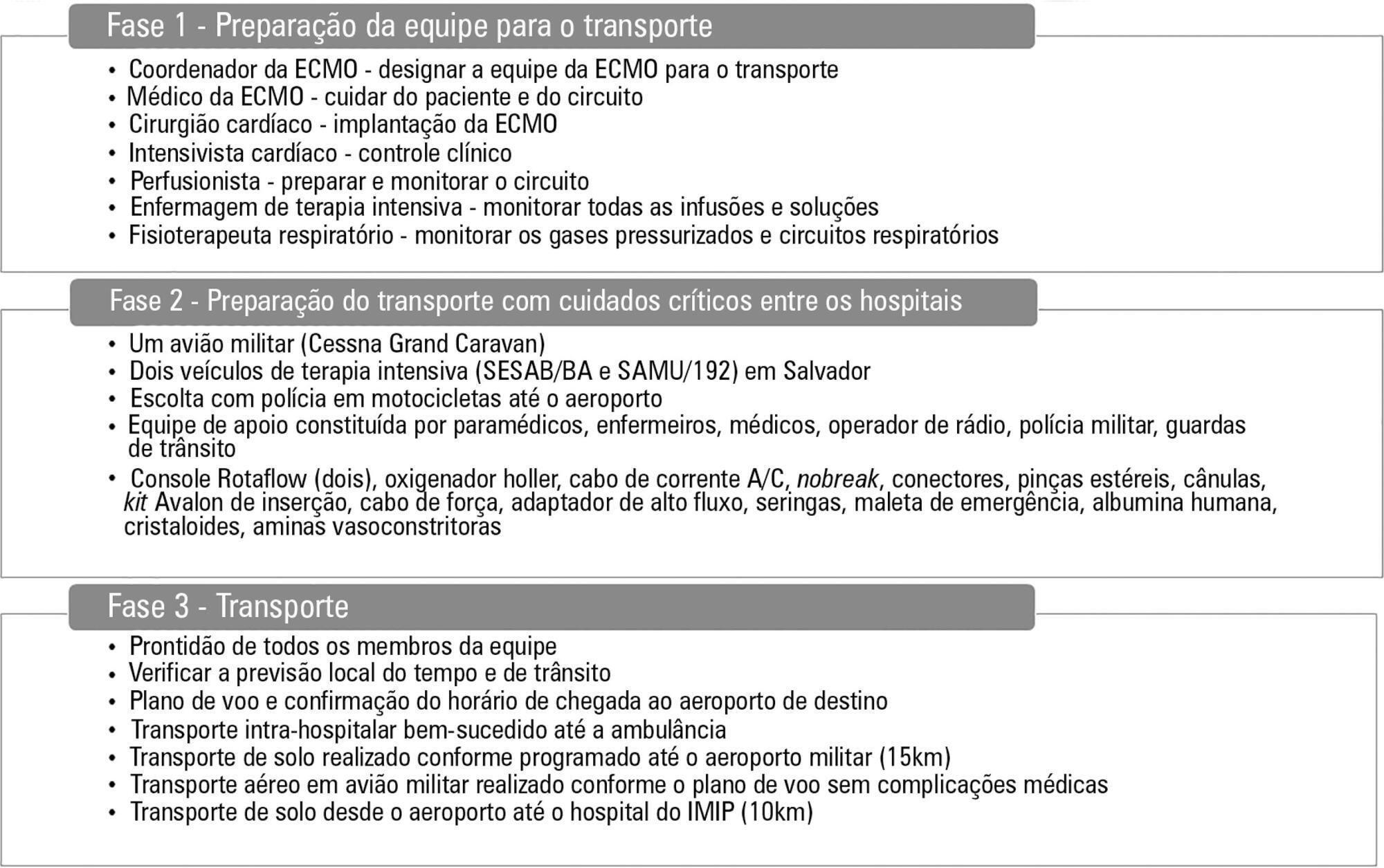
A series of 18 patients in the state of São Paulo, Brazil is described. All patients were consecutively evaluated by a multidisciplinary team at the hospital of origin. The patients were rescued, and extracorporeal membrane oxygenation support was provided on site. The patients were then transported to referral hospitals for extracorporeal membrane oxygenation support. Data were retrieved from a prospectively collected database.
From 2011 to 2017, 18 patients aged 29 (25 - 31) years with a SAPS 3 of 84 (68 - 92) and main primary diagnosis of leptospirosis and influenza A (H1N1) virus were transported to three referral hospitals in São Paulo. A median distance of 39 (15 - 82) km was traveled on each rescue mission during a period of 360 (308 - 431) min. A median of one (0 - 2) nurse, three (2 - 3) physicians, and one (0 - 1) physical therapist was present per rescue. Seventeen rescues were made by ambulance, and one rescue was made by helicopter. The observed complications were interruption in the energy supply to the pump in two cases (11%) and oxygen saturation < 70% in two cases. Thirteen patients (72%) survived and were discharged from the hospital. Among the nonsurvivors, there were two cases of brain death, two cases of multiple organ dysfunction syndrome, and one case of irreversible pulmonary fibrosis.
Transportation with extracorporeal support occurred without serious complications, and the hospital survival rate was high.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):317-326
DOI 10.5935/0103-507X.20180052
To characterize the transport of severely ill patients with extracorporeal respiratory or cardiovascular support.
A series of 18 patients in the state of São Paulo, Brazil is described. All patients were consecutively evaluated by a multidisciplinary team at the hospital of origin. The patients were rescued, and extracorporeal membrane oxygenation support was provided on site. The patients were then transported to referral hospitals for extracorporeal membrane oxygenation support. Data were retrieved from a prospectively collected database.
From 2011 to 2017, 18 patients aged 29 (25 - 31) years with a SAPS 3 of 84 (68 - 92) and main primary diagnosis of leptospirosis and influenza A (H1N1) virus were transported to three referral hospitals in São Paulo. A median distance of 39 (15 - 82) km was traveled on each rescue mission during a period of 360 (308 - 431) min. A median of one (0 - 2) nurse, three (2 - 3) physicians, and one (0 - 1) physical therapist was present per rescue. Seventeen rescues were made by ambulance, and one rescue was made by helicopter. The observed complications were interruption in the energy supply to the pump in two cases (11%) and oxygen saturation < 70% in two cases. Thirteen patients (72%) survived and were discharged from the hospital. Among the nonsurvivors, there were two cases of brain death, two cases of multiple organ dysfunction syndrome, and one case of irreversible pulmonary fibrosis.
Transportation with extracorporeal support occurred without serious complications, and the hospital survival rate was high.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):271-278
DOI 10.5935/0103-507X.20170048
This report aimed to describe the outcomes of the patients with severe H1N1 associated acute respiratory distress syndrome who were treated with extracorporeal membrane oxygenation therapy.
This retrospective review analyzed a single-center cohort of adult patients with H1N1-related acute respiratory distress syndrome who were managed with veno-venous extracorporeal membrane oxygenation during the winter of 2013/2014.
A total of 10 patients received veno-venous extracorporeal membrane oxygenation for H1N1 influenza between January 2013 and March 2014. Seven patients were transferred to our center for extracorporeal membrane oxygenation consideration (all within 72 hours of initiating mechanical ventilation). The median patient age was forty years, and 30% were female. The median arterial oxygen partial pressure to fraction of inspired oxygen ratio was 62.5, and the median RESP score was 6. Three patients received inhaled nitric oxide, and four patients were proned as rescue therapy before extracorporeal membrane oxygenation was initiated. The median duration of mechanical ventilation was twenty-two days (range, 14 - 32). The median length of stay in the intensive care unit was twenty-seven days (range, 14 - 39). The median hospital length of stay was 29.1 days (range, 16.0 - 46.9). Minor bleeding complications occurred in 6 of 10 patients. Eight of the ten patients survived to hospital discharge.
The survivors were relatively young and discharged with good functional status (i.e., enhancing quality-adjusted life-years-saved). Our experience shows that even a relatively new extracorporeal membrane oxygenation program can play an important role in that capacity and provide excellent outcomes for the sickest patients.
Abstract
Rev Bras Ter Intensiva. 2017;29(3):271-278
DOI 10.5935/0103-507X.20170048
This report aimed to describe the outcomes of the patients with severe H1N1 associated acute respiratory distress syndrome who were treated with extracorporeal membrane oxygenation therapy.
This retrospective review analyzed a single-center cohort of adult patients with H1N1-related acute respiratory distress syndrome who were managed with veno-venous extracorporeal membrane oxygenation during the winter of 2013/2014.
A total of 10 patients received veno-venous extracorporeal membrane oxygenation for H1N1 influenza between January 2013 and March 2014. Seven patients were transferred to our center for extracorporeal membrane oxygenation consideration (all within 72 hours of initiating mechanical ventilation). The median patient age was forty years, and 30% were female. The median arterial oxygen partial pressure to fraction of inspired oxygen ratio was 62.5, and the median RESP score was 6. Three patients received inhaled nitric oxide, and four patients were proned as rescue therapy before extracorporeal membrane oxygenation was initiated. The median duration of mechanical ventilation was twenty-two days (range, 14 - 32). The median length of stay in the intensive care unit was twenty-seven days (range, 14 - 39). The median hospital length of stay was 29.1 days (range, 16.0 - 46.9). Minor bleeding complications occurred in 6 of 10 patients. Eight of the ten patients survived to hospital discharge.
The survivors were relatively young and discharged with good functional status (i.e., enhancing quality-adjusted life-years-saved). Our experience shows that even a relatively new extracorporeal membrane oxygenation program can play an important role in that capacity and provide excellent outcomes for the sickest patients.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):78-82
DOI 10.5935/0103-507X.20160001
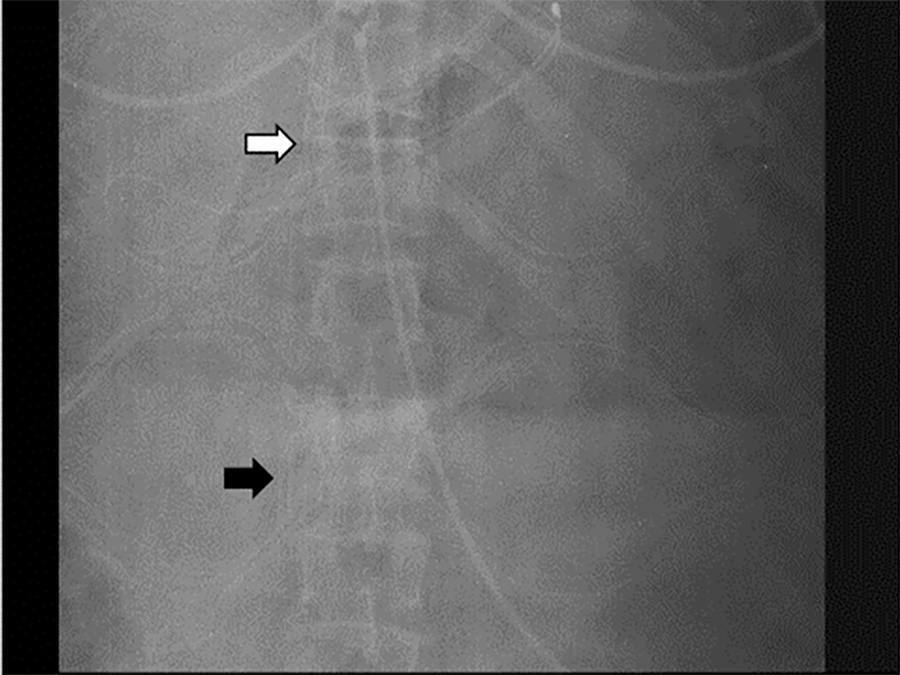
Extracorporeal membrane oxygenation is used in refractory hypoxemia in many clinical settings. Thoracic trauma patients usually develop acute respiratory distress syndrome. Due to high risk of bleeding, thrombotic complications present in this context are particularly difficult to manage and usually require insertion of an inferior vena cava filter to prevent embolism from the distal veins to the pulmonary circulation. Here, we present a case of a thoracic trauma patient with severe acute respiratory distress syndrome requiring venovenous extracorporeal membrane oxygenation via a right internal jugular double lumen cannula due to a previously inserted inferior vena cava filter caused by distal bilateral calf muscle vein deep vein thrombosis.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):78-82
DOI 10.5935/0103-507X.20160001
Extracorporeal membrane oxygenation is used in refractory hypoxemia in many clinical settings. Thoracic trauma patients usually develop acute respiratory distress syndrome. Due to high risk of bleeding, thrombotic complications present in this context are particularly difficult to manage and usually require insertion of an inferior vena cava filter to prevent embolism from the distal veins to the pulmonary circulation. Here, we present a case of a thoracic trauma patient with severe acute respiratory distress syndrome requiring venovenous extracorporeal membrane oxygenation via a right internal jugular double lumen cannula due to a previously inserted inferior vena cava filter caused by distal bilateral calf muscle vein deep vein thrombosis.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):11-18
DOI 10.5935/0103-507X.20160006
The aim of this study was to explore the factors associated with blood oxygen partial pressure and carbon dioxide partial pressure.
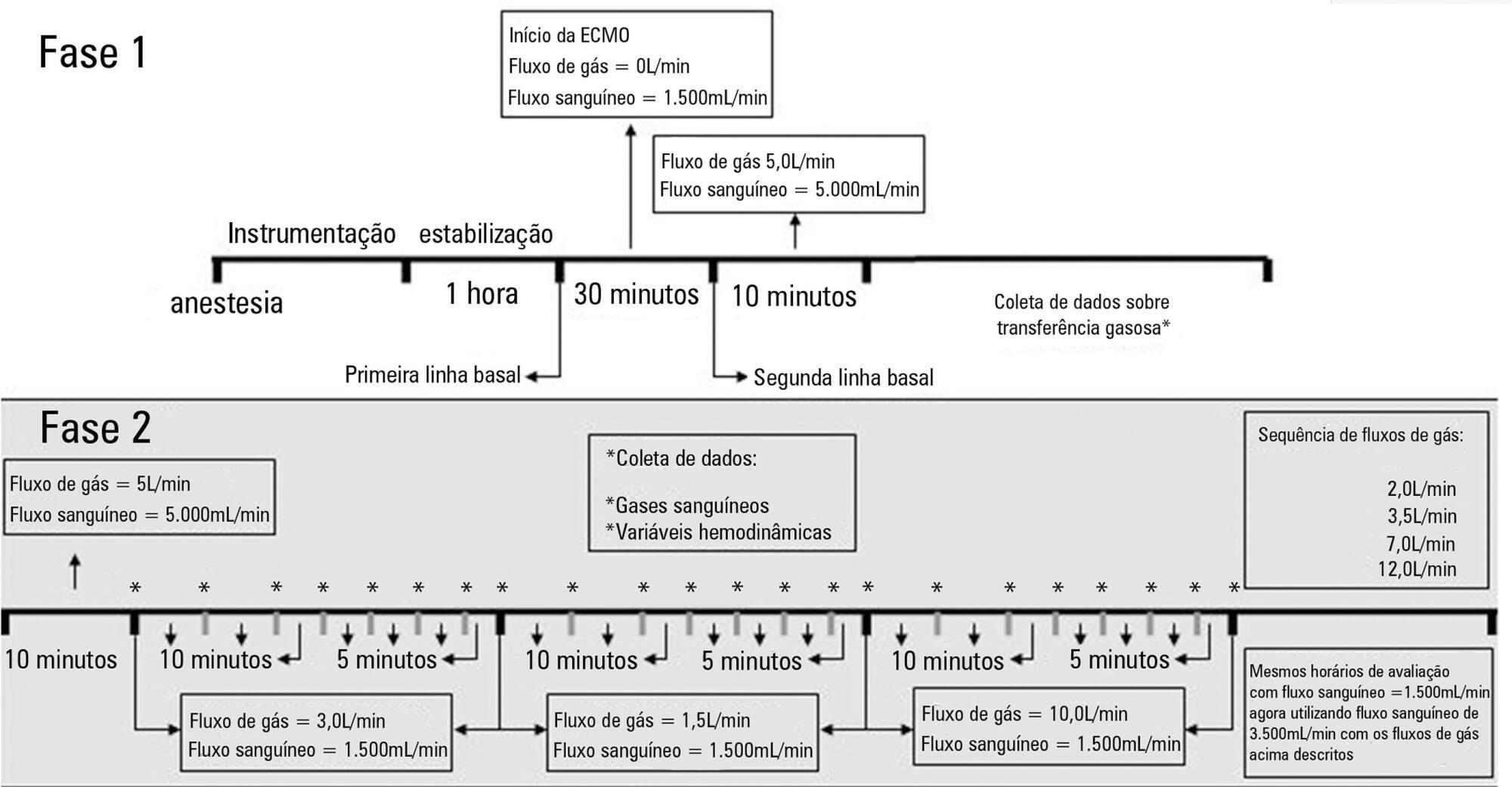
The factors associated with oxygen - and carbon dioxide regulation were investigated in an apneic pig model under veno-venous extracorporeal membrane oxygenation support. A predefined sequence of blood and sweep flows was tested.
Oxygenation was mainly associated with extracorporeal membrane oxygenation blood flow (beta coefficient = 0.036mmHg/mL/min), cardiac output (beta coefficient = -11.970mmHg/L/min) and pulmonary shunting (beta coefficient = -0.232mmHg/%). Furthermore, the initial oxygen partial pressure and carbon dioxide partial pressure measurements were also associated with oxygenation, with beta coefficients of 0.160 and 0.442mmHg/mmHg, respectively. Carbon dioxide partial pressure was associated with cardiac output (beta coefficient = 3.578mmHg/L/min), sweep gas flow (beta coefficient = -2.635mmHg/L/min), temperature (beta coefficient = 4.514mmHg/ºC), initial pH (beta coefficient = -66.065mmHg/0.01 unit) and hemoglobin (beta coefficient = 6.635mmHg/g/dL).
In conclusion, elevations in blood and sweep gas flows in an apneic veno-venous extracorporeal membrane oxygenation model resulted in an increase in oxygen partial pressure and a reduction in carbon dioxide partial pressure 2, respectively. Furthermore, without the possibility of causal inference, oxygen partial pressure was negatively associated with pulmonary shunting and cardiac output, and carbon dioxide partial pressure was positively associated with cardiac output, core temperature and initial hemoglobin.
Abstract
Rev Bras Ter Intensiva. 2016;28(1):11-18
DOI 10.5935/0103-507X.20160006
The aim of this study was to explore the factors associated with blood oxygen partial pressure and carbon dioxide partial pressure.
The factors associated with oxygen - and carbon dioxide regulation were investigated in an apneic pig model under veno-venous extracorporeal membrane oxygenation support. A predefined sequence of blood and sweep flows was tested.
Oxygenation was mainly associated with extracorporeal membrane oxygenation blood flow (beta coefficient = 0.036mmHg/mL/min), cardiac output (beta coefficient = -11.970mmHg/L/min) and pulmonary shunting (beta coefficient = -0.232mmHg/%). Furthermore, the initial oxygen partial pressure and carbon dioxide partial pressure measurements were also associated with oxygenation, with beta coefficients of 0.160 and 0.442mmHg/mmHg, respectively. Carbon dioxide partial pressure was associated with cardiac output (beta coefficient = 3.578mmHg/L/min), sweep gas flow (beta coefficient = -2.635mmHg/L/min), temperature (beta coefficient = 4.514mmHg/ºC), initial pH (beta coefficient = -66.065mmHg/0.01 unit) and hemoglobin (beta coefficient = 6.635mmHg/g/dL).
In conclusion, elevations in blood and sweep gas flows in an apneic veno-venous extracorporeal membrane oxygenation model resulted in an increase in oxygen partial pressure and a reduction in carbon dioxide partial pressure 2, respectively. Furthermore, without the possibility of causal inference, oxygen partial pressure was negatively associated with pulmonary shunting and cardiac output, and carbon dioxide partial pressure was positively associated with cardiac output, core temperature and initial hemoglobin.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):397-401
DOI 10.5935/0103-507X.20150066
A 17-year-old Brazilian male presented with progressive dyspnea for 15 days, worsening in the last 24 hours, and was admitted in respiratory failure and cardiogenic shock, with multiple organ dysfunctions. Echocardiography showed a left ventricle ejection fraction of 11%, severe diffuse hypokinesia, and a systolic pulmonary artery pressure of 50mmHg, resulting in the need for hemodynamic support with dobutamine (20mcg/kg/min) and noradrenaline (1.7mcg/kg/min). After 48 hours with no clinical or hemodynamic improvement, an extracorporeal membrane oxygenation was implanted. The patient presented with hemodynamic, systemic perfusion and renal and liver function improvements; however, his cardiac function did not recover after 72 hours, and he was transfer to another hospital. Air transport was conducted from Salvador to Recife in Brazil. A heart transplant was performed with rapid recovery of both liver and kidney functions, as well as good graft function. Histopathology of the explanted heart showed chronic active myocarditis and amastigotes of Trypanosoma cruzi. The estimated global prevalence of T. cruzi infections declined from 18 million in 1991, when the first regional control initiative began, to 5.7 million in 2010. Myocarditis is an inflammatory disease due to infectious or non-infectious conditions. Clinical manifestation is variable, ranging from subclinical presentation to refractory heart failure and cardiogenic shock. Several reports suggest that the use of extracorporeal membrane oxygenation in patients presenting with severe refractory myocarditis is a potential bridging therapy to heart transplant when there is no spontaneous recovery of ventricular function. In a 6-month follow-up outpatient consult, the patient presented well and was asymptomatic.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):397-401
DOI 10.5935/0103-507X.20150066
A 17-year-old Brazilian male presented with progressive dyspnea for 15 days, worsening in the last 24 hours, and was admitted in respiratory failure and cardiogenic shock, with multiple organ dysfunctions. Echocardiography showed a left ventricle ejection fraction of 11%, severe diffuse hypokinesia, and a systolic pulmonary artery pressure of 50mmHg, resulting in the need for hemodynamic support with dobutamine (20mcg/kg/min) and noradrenaline (1.7mcg/kg/min). After 48 hours with no clinical or hemodynamic improvement, an extracorporeal membrane oxygenation was implanted. The patient presented with hemodynamic, systemic perfusion and renal and liver function improvements; however, his cardiac function did not recover after 72 hours, and he was transfer to another hospital. Air transport was conducted from Salvador to Recife in Brazil. A heart transplant was performed with rapid recovery of both liver and kidney functions, as well as good graft function. Histopathology of the explanted heart showed chronic active myocarditis and amastigotes of Trypanosoma cruzi. The estimated global prevalence of T. cruzi infections declined from 18 million in 1991, when the first regional control initiative began, to 5.7 million in 2010. Myocarditis is an inflammatory disease due to infectious or non-infectious conditions. Clinical manifestation is variable, ranging from subclinical presentation to refractory heart failure and cardiogenic shock. Several reports suggest that the use of extracorporeal membrane oxygenation in patients presenting with severe refractory myocarditis is a potential bridging therapy to heart transplant when there is no spontaneous recovery of ventricular function. In a 6-month follow-up outpatient consult, the patient presented well and was asymptomatic.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):178-184
DOI 10.5935/0103-507X.20150030
To analyze the correlations of the blood flow/pump rotation ratio and the transmembrane pressure, CO2 and O2 transfer during the extracorporeal respiratory support.
Five animals were instrumented and submitted to extracorporeal membrane oxygenation in a five-step protocol, including abdominal sepsis and lung injury.
This study showed that blood flow/pump rotations ratio variations are dependent on extracorporeal membrane oxygenation blood flow in a positive logarithmic fashion. Blood flow/pump rotation ratio variations are negatively associated with transmembrane pressure (R2 = 0.5 for blood flow = 1500mL/minute and R2 = 0.4 for blood flow = 3500mL/minute, both with p < 0.001) and positively associated with CO2 transfer variations (R2 = 0.2 for sweep gas flow ≤ 6L/minute, p < 0.001, and R2 = 0.1 for sweep gas flow > 6L/minute, p = 0.006), and the blood flow/pump rotation ratio is not associated with O2 transfer variations (R2 = 0.01 for blood flow = 1500mL/minute, p = 0.19, and R2 = - 0.01 for blood flow = 3500 mL/minute, p = 0.46).
Blood flow/pump rotation ratio variation is negatively associated with transmembrane pressure and positively associated with CO2 transfer in this animal model. According to the clinical situation, a decrease in the blood flow/pump rotation ratio can indicate artificial lung dysfunction without the occurrence of hypoxemia.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):178-184
DOI 10.5935/0103-507X.20150030
To analyze the correlations of the blood flow/pump rotation ratio and the transmembrane pressure, CO2 and O2 transfer during the extracorporeal respiratory support.
Five animals were instrumented and submitted to extracorporeal membrane oxygenation in a five-step protocol, including abdominal sepsis and lung injury.
This study showed that blood flow/pump rotations ratio variations are dependent on extracorporeal membrane oxygenation blood flow in a positive logarithmic fashion. Blood flow/pump rotation ratio variations are negatively associated with transmembrane pressure (R2 = 0.5 for blood flow = 1500mL/minute and R2 = 0.4 for blood flow = 3500mL/minute, both with p < 0.001) and positively associated with CO2 transfer variations (R2 = 0.2 for sweep gas flow ≤ 6L/minute, p < 0.001, and R2 = 0.1 for sweep gas flow > 6L/minute, p = 0.006), and the blood flow/pump rotation ratio is not associated with O2 transfer variations (R2 = 0.01 for blood flow = 1500mL/minute, p = 0.19, and R2 = - 0.01 for blood flow = 3500 mL/minute, p = 0.46).
Blood flow/pump rotation ratio variation is negatively associated with transmembrane pressure and positively associated with CO2 transfer in this animal model. According to the clinical situation, a decrease in the blood flow/pump rotation ratio can indicate artificial lung dysfunction without the occurrence of hypoxemia.

Abstract
Rev Bras Ter Intensiva. 2015;27(2):134-140
DOI 10.5935/0103-507X.20150024
The development of the extracorporeal membrane oxygenation in Latin America represents a challenge in this specialty field. The objective of this article was to describe the results of a new extracorporeal membrane oxygenation program in an intensive care unit.
This retrospective cohort study included 22 patients who required extracorporeal membrane oxygenation and were treated from January 2011 to June 2014. The baseline characteristics, indications, duration of the condition, days on mechanical ventilation, days in the intensive care unit, complications, and hospital mortality were evaluated.
Fifteen patients required extracorporeal membrane oxygenation after lung transplantation, and seven patients required oxygenation due to acute respiratory distress. All transplanted patients were weaned from extracorporeal membrane oxygenation with a median duration of 3 days (Interquartile range - IQR: 2 - 5), were on mechanical ventilation for a median of 15.5 days (IQR: 3 - 25), and had an intensive care unit stay of 31.5 days (IQR: 19 - 53) and a median hospital stay of 60 days (IQR: 36 - 89) with 20% mortality. Patients with acute respiratory distress had a median oxygenation membrane duration of 9 days (IQR: 3 - 14), median mechanical ventilation time of 25 days (IQR: 13 - 37), a 31 day stay in therapy (IQR: 11 - 38), a 32 day stay in the hospital (IQR: 11 - 41), and 57% mortality. The main complications were infections (80%), acute kidney failure (43%), bleeding at the surgical site and at the site of cannula placement (22%), plateletopenia (60%), and coagulopathy (30%).
In spite of the steep learning curve, we considered this experience to be satisfactory, with results and complications comparable to those reported in the literature.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):134-140
DOI 10.5935/0103-507X.20150024
The development of the extracorporeal membrane oxygenation in Latin America represents a challenge in this specialty field. The objective of this article was to describe the results of a new extracorporeal membrane oxygenation program in an intensive care unit.
This retrospective cohort study included 22 patients who required extracorporeal membrane oxygenation and were treated from January 2011 to June 2014. The baseline characteristics, indications, duration of the condition, days on mechanical ventilation, days in the intensive care unit, complications, and hospital mortality were evaluated.
Fifteen patients required extracorporeal membrane oxygenation after lung transplantation, and seven patients required oxygenation due to acute respiratory distress. All transplanted patients were weaned from extracorporeal membrane oxygenation with a median duration of 3 days (Interquartile range - IQR: 2 - 5), were on mechanical ventilation for a median of 15.5 days (IQR: 3 - 25), and had an intensive care unit stay of 31.5 days (IQR: 19 - 53) and a median hospital stay of 60 days (IQR: 36 - 89) with 20% mortality. Patients with acute respiratory distress had a median oxygenation membrane duration of 9 days (IQR: 3 - 14), median mechanical ventilation time of 25 days (IQR: 13 - 37), a 31 day stay in therapy (IQR: 11 - 38), a 32 day stay in the hospital (IQR: 11 - 41), and 57% mortality. The main complications were infections (80%), acute kidney failure (43%), bleeding at the surgical site and at the site of cannula placement (22%), plateletopenia (60%), and coagulopathy (30%).
In spite of the steep learning curve, we considered this experience to be satisfactory, with results and complications comparable to those reported in the literature.