Critical illness Archives - Critical Care Science (CCS)

Abstract
Revista Brasileira de Terapia Intensiva. 2010;22(3):236-244
DOI 10.1590/S0103-507X2010000300004
OBJECTIVES: Critically ill cancer patients are at increased risk for acute kidney injury, but studies on these patients are scarce and were all single centered conducted in specialized intensive care units. The objective was to evaluate the characteristics and outcomes in a prospective cohort of cancer patients admitted to several intensive care units with acute kidney injury. METHODS: Prospective multicenter cohort study conducted in intensive care units from 28 hospitals in Brazil over a two-month period. Univariate and multivariate logistic regression were used to identify factors associated with hospital mortality. RESULTS: Out of all 717 intensive care unit admissions, 87 (12%) had acute kidney injury and 36% of them received renal replacement therapy. Kidney injury developed more frequently in patients with hematological malignancies than in patients with solid tumors (26% vs. 11%, P=0.003). Ischemia/shock (76%) and sepsis (67%) were the main contributing factor for and kidney injury was multifactorial in 79% of the patients. Hospital mortality was 71%. General and renal-specific severity-of-illness scores were inaccurate in predicting outcomes for these patients. In a multivariate analysis, length of hospital stay prior to intensive care unit, acute organ dysfunctions, need for mechanical ventilation and a poor performance status were associated with increased mortality. Moreover, cancer-related characteristics were not associated with outcomes. CONCLUSIONS: The present study demonstrates that intensive care units admission and advanced life-support should be considered in selected critically ill cancer patients with kidney injury.
Abstract
Revista Brasileira de Terapia Intensiva. 2010;22(3):236-244
DOI 10.1590/S0103-507X2010000300004
OBJECTIVES: Critically ill cancer patients are at increased risk for acute kidney injury, but studies on these patients are scarce and were all single centered conducted in specialized intensive care units. The objective was to evaluate the characteristics and outcomes in a prospective cohort of cancer patients admitted to several intensive care units with acute kidney injury. METHODS: Prospective multicenter cohort study conducted in intensive care units from 28 hospitals in Brazil over a two-month period. Univariate and multivariate logistic regression were used to identify factors associated with hospital mortality. RESULTS: Out of all 717 intensive care unit admissions, 87 (12%) had acute kidney injury and 36% of them received renal replacement therapy. Kidney injury developed more frequently in patients with hematological malignancies than in patients with solid tumors (26% vs. 11%, P=0.003). Ischemia/shock (76%) and sepsis (67%) were the main contributing factor for and kidney injury was multifactorial in 79% of the patients. Hospital mortality was 71%. General and renal-specific severity-of-illness scores were inaccurate in predicting outcomes for these patients. In a multivariate analysis, length of hospital stay prior to intensive care unit, acute organ dysfunctions, need for mechanical ventilation and a poor performance status were associated with increased mortality. Moreover, cancer-related characteristics were not associated with outcomes. CONCLUSIONS: The present study demonstrates that intensive care units admission and advanced life-support should be considered in selected critically ill cancer patients with kidney injury.
Abstract
Revista Brasileira de Terapia Intensiva. 2010;22(2):166-174
DOI 10.1590/S0103-507X2010000200011
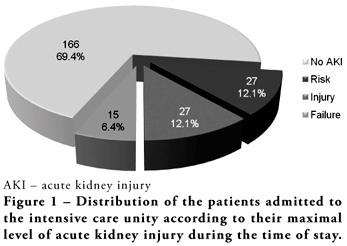
OBJECTIVES: Acute kidney injury is characterized by sudden and generally revertible renal function impairment involving inability to maintain homeostasis. In pediatrics, the main causes of acute kidney injury are sepsis, use of nephrotoxic drugs and renal ischemia in critically ill patients. The incidence of acute kidney injury in these patients ranges from 20 to 30%, resulting in increased morbid-mortality, a 40 to 90% rate. This study aimed to evaluate the incidence of acute kidney injury in intensive care unit patients, to categorize the severity of the acute kidney injury according to the Pediatric Risk, Injury, Failure, Loss, End-Stage (pRIFLE), examine the relationship between the acute kidney injury and severity using the Pediatric Index of Mortality (PIM) and to analyze outcome predictors. METHODS: A prospective study of the patients admitted to the intensive care unit of Hospital Infantil Joana de Gusmão - Florianópolis / SC - Brazil was conducted between July 2008 and January 2009. Were evaluated daily the urine output and serum creatinine, and the patients were categorized according to the pRIFLE criteria. RESULTS: During the follow-up period, 235 children were admitted. The incidence of acute kidney injury was 30.6%, and the maximal pRIFLE score during hospitalization was 12.1% for R, 12.1% for I and 6.4% for F. The mortality rate was 12.3%. The patients who developed acute kidney injury had a ten times bigger risk of death versus the not exposed patients. CONCLUSIONS: Acute kidney injury is frequent in critically ill patients. Early diagnosis and prompt and appropriate therapy for each clinical aspect may change this condition's course and severity, and reduce the patients' morbidity and mortality.
Abstract
Revista Brasileira de Terapia Intensiva. 2010;22(2):166-174
DOI 10.1590/S0103-507X2010000200011
OBJECTIVES: Acute kidney injury is characterized by sudden and generally revertible renal function impairment involving inability to maintain homeostasis. In pediatrics, the main causes of acute kidney injury are sepsis, use of nephrotoxic drugs and renal ischemia in critically ill patients. The incidence of acute kidney injury in these patients ranges from 20 to 30%, resulting in increased morbid-mortality, a 40 to 90% rate. This study aimed to evaluate the incidence of acute kidney injury in intensive care unit patients, to categorize the severity of the acute kidney injury according to the Pediatric Risk, Injury, Failure, Loss, End-Stage (pRIFLE), examine the relationship between the acute kidney injury and severity using the Pediatric Index of Mortality (PIM) and to analyze outcome predictors. METHODS: A prospective study of the patients admitted to the intensive care unit of Hospital Infantil Joana de Gusmão - Florianópolis / SC - Brazil was conducted between July 2008 and January 2009. Were evaluated daily the urine output and serum creatinine, and the patients were categorized according to the pRIFLE criteria. RESULTS: During the follow-up period, 235 children were admitted. The incidence of acute kidney injury was 30.6%, and the maximal pRIFLE score during hospitalization was 12.1% for R, 12.1% for I and 6.4% for F. The mortality rate was 12.3%. The patients who developed acute kidney injury had a ten times bigger risk of death versus the not exposed patients. CONCLUSIONS: Acute kidney injury is frequent in critically ill patients. Early diagnosis and prompt and appropriate therapy for each clinical aspect may change this condition's course and severity, and reduce the patients' morbidity and mortality.
Abstract
Revista Brasileira de Terapia Intensiva. 2009;21(3):306-309
DOI 10.1590/S0103-507X2009000300011
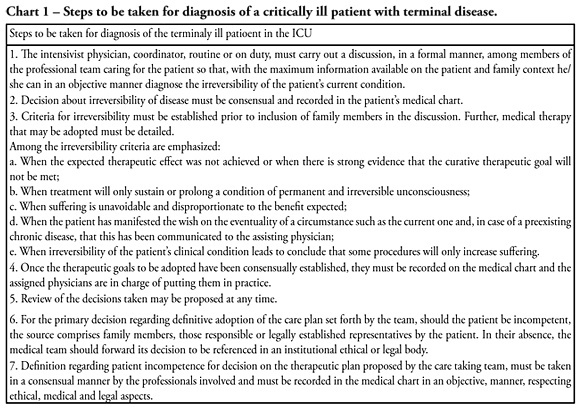
Withholding of treatment in patients with terminal disease is increasingly common in intensive care units, throughout the world. Notwithstanding, Brazilian intensivists still have a great difficulty to offer the best treatment to patients that have not benefited from curative care. The objective of this comment is to suggest an algorithm for the care of terminally ill patients. It was formulated based upon literature and the experience of experts, by members of the ethics committee and end-of-life of AMIB - Brazilian Association of Intensive Care.
Abstract
Revista Brasileira de Terapia Intensiva. 2009;21(3):306-309
DOI 10.1590/S0103-507X2009000300011
Withholding of treatment in patients with terminal disease is increasingly common in intensive care units, throughout the world. Notwithstanding, Brazilian intensivists still have a great difficulty to offer the best treatment to patients that have not benefited from curative care. The objective of this comment is to suggest an algorithm for the care of terminally ill patients. It was formulated based upon literature and the experience of experts, by members of the ethics committee and end-of-life of AMIB - Brazilian Association of Intensive Care.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(1):22-26
DOI 10.1590/S0103-507X2006000100005
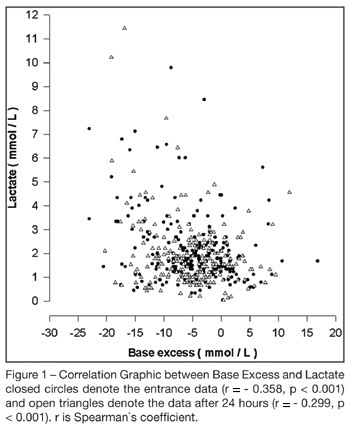
BACKGROUND AND OBJECTIVES: To correlate standard base excess (SBE) with serum lactate level and demonstrate the independent prognostic significance of each one. METHODS: In a retrospective study, we retrieved data from 333 patients of our prospectively collected database of 7-bed medical intensive care unit of a 1800-bed university hospital. RESULTS: The results have shown a poor correlation between SBE and lactate, r = - 0.358, p < 0.001, and an independent prognostic significance of each one when analyzed concomitantly, odds ratio (95% Confidence interval) = 0.996 (0.992 - 0.999) to standard base excess and 1.000 (1.000 - 1.002) to lactate at entrance; and odds ratio (95% Confidence interval ) = 0.990 (0.985 - 0.994) to standard base excess and 1.003 (1.001 - 1.005) to lactate after 24 hours. The accuracy of standard base excess was close to lactate to determine in-intensive care unit death. CONCLUSIONS: The lactic component of the metabolic acidosis is not the major determinant of standard base excess. Serum lactate and SBE are independent outcome predictors in critically ill patients.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(1):22-26
DOI 10.1590/S0103-507X2006000100005
BACKGROUND AND OBJECTIVES: To correlate standard base excess (SBE) with serum lactate level and demonstrate the independent prognostic significance of each one. METHODS: In a retrospective study, we retrieved data from 333 patients of our prospectively collected database of 7-bed medical intensive care unit of a 1800-bed university hospital. RESULTS: The results have shown a poor correlation between SBE and lactate, r = - 0.358, p < 0.001, and an independent prognostic significance of each one when analyzed concomitantly, odds ratio (95% Confidence interval) = 0.996 (0.992 - 0.999) to standard base excess and 1.000 (1.000 - 1.002) to lactate at entrance; and odds ratio (95% Confidence interval ) = 0.990 (0.985 - 0.994) to standard base excess and 1.003 (1.001 - 1.005) to lactate after 24 hours. The accuracy of standard base excess was close to lactate to determine in-intensive care unit death. CONCLUSIONS: The lactic component of the metabolic acidosis is not the major determinant of standard base excess. Serum lactate and SBE are independent outcome predictors in critically ill patients.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(3):307-310
DOI 10.1590/S0103-507X2006000300014
BACKGROUND AND OBJECTIVES: The diffuse axonal polyneuropathy, more commonly known as Critical Illness Polyneuropathy (CIP), has been discussed by authors by decades; however, it has only been deeply studied over the last thirty years, becoming more important as an important cause of long term dependence on mechanical ventilation by seriously ill patients in intensive care medicine. CONTENTS: A significant reason for such interest is due to the importance of the CIP as complication of the septic shock and in patients with multiple organ failure, as much as responsible for the prolonging hospitalization in the Intensive Care Unit, as for the gradual reduction of the chance of survival. It has been suggested that the polyneuropathy is related with cytokines and other mediators which would increase the permeability of the vases, resulting in endoneural edema and causing the axonal injury. It is difficult to do the initial diagnostic, which, in general, are only possibly recognized when the sepsis complications or the multiple organs failure have been satisfactorily controlled. The diagnosis is made through the eletroneuromiography exam, and although there is still no effective drug treatment other than the control of the basic illness, it is consensus among multidisciplinary team that the development of the CIP does not have to be understood as a way to reduce the intensity of treatment. CONCLUSIONS: Spit of your prevalence, it is still unknown the mainly factors which are physiopathology associated as soon as your correct therapy.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(3):307-310
DOI 10.1590/S0103-507X2006000300014
BACKGROUND AND OBJECTIVES: The diffuse axonal polyneuropathy, more commonly known as Critical Illness Polyneuropathy (CIP), has been discussed by authors by decades; however, it has only been deeply studied over the last thirty years, becoming more important as an important cause of long term dependence on mechanical ventilation by seriously ill patients in intensive care medicine. CONTENTS: A significant reason for such interest is due to the importance of the CIP as complication of the septic shock and in patients with multiple organ failure, as much as responsible for the prolonging hospitalization in the Intensive Care Unit, as for the gradual reduction of the chance of survival. It has been suggested that the polyneuropathy is related with cytokines and other mediators which would increase the permeability of the vases, resulting in endoneural edema and causing the axonal injury. It is difficult to do the initial diagnostic, which, in general, are only possibly recognized when the sepsis complications or the multiple organs failure have been satisfactorily controlled. The diagnosis is made through the eletroneuromiography exam, and although there is still no effective drug treatment other than the control of the basic illness, it is consensus among multidisciplinary team that the development of the CIP does not have to be understood as a way to reduce the intensity of treatment. CONCLUSIONS: Spit of your prevalence, it is still unknown the mainly factors which are physiopathology associated as soon as your correct therapy.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(3):268-275
DOI 10.1590/S0103-507X2006000300009
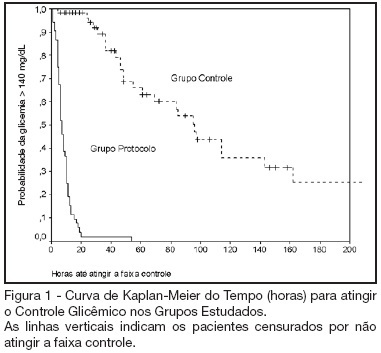
BACKGROUND AND OBJECTIVES: Actually tight glycemic control is a major concern in critical care. The objective of this study was to evaluate effectiveness and safety of Yale insulin infusion protocol in a Brazilian medical and surgical intensive care unit. METHODS: Retrospective, before-after cohort study. Selected end-points were mean blood glucose levels, time-to-reach target range of 80 - 140 mg/dL, and percent of blood glucose in target range and hypoglycemia incidence. RESULTS: Were studied 112 patients: 60 in control group (CG) and 52 in protocol group (PG). Bedside blood glucose was measured 5392 times for a mean value of 131.2 ± 14.7 mg/dL in the PG versus 2485 times for a mean value of 181.7 ± 36.1 mg/dL in the CG. Blood glucose values were in the target range 65% and 32% of the times, respectively for PG and CG groups (p < 0.001). The median time to reach glucose target range was 7 h (range 4 -10 h) for PG and 96 hr (range 46 - 278 h) for CG (p < 0.001). Incidence of severe hypoglycemia did not reach difference statistically significant: 4 patients in PG versus 2 patients in CG. CONCLUSIONS: Yale insulin infusion protocol was effective and safe to improve blood glucose control in a Brazilian medical and surgical intensive care unit.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(3):268-275
DOI 10.1590/S0103-507X2006000300009
BACKGROUND AND OBJECTIVES: Actually tight glycemic control is a major concern in critical care. The objective of this study was to evaluate effectiveness and safety of Yale insulin infusion protocol in a Brazilian medical and surgical intensive care unit. METHODS: Retrospective, before-after cohort study. Selected end-points were mean blood glucose levels, time-to-reach target range of 80 - 140 mg/dL, and percent of blood glucose in target range and hypoglycemia incidence. RESULTS: Were studied 112 patients: 60 in control group (CG) and 52 in protocol group (PG). Bedside blood glucose was measured 5392 times for a mean value of 131.2 ± 14.7 mg/dL in the PG versus 2485 times for a mean value of 181.7 ± 36.1 mg/dL in the CG. Blood glucose values were in the target range 65% and 32% of the times, respectively for PG and CG groups (p < 0.001). The median time to reach glucose target range was 7 h (range 4 -10 h) for PG and 96 hr (range 46 - 278 h) for CG (p < 0.001). Incidence of severe hypoglycemia did not reach difference statistically significant: 4 patients in PG versus 2 patients in CG. CONCLUSIONS: Yale insulin infusion protocol was effective and safe to improve blood glucose control in a Brazilian medical and surgical intensive care unit.