Critical care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2012;24(3):246-251
DOI 10.1590/S0103-507X2012000300007
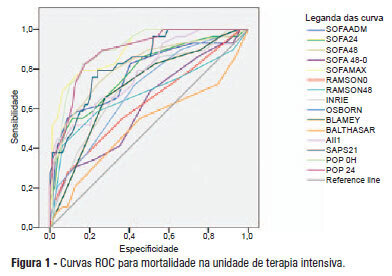
OBJECTIVE: This study compared the general and specific severity indices to assess the prognosis of severe acute pancreatitis at a polyvalent intensive care unit. METHODS: This retrospective study included 108 patients who were diagnosed with severe acute pancreatitis from July 1, 1999 to March 31, 2012. Their demographic and clinical data were collected, and the following severity indices were calculated: Ranson, Osborne, Blamey and Imrie, Balthazar, POP, APACHE II, SAPS II, and SOFA. The discriminative power of these indices with regard to mortality at the intensive care unit and hospital was assessed using the area under the ROC curve. RESULTS: The demographic data of the surviving and deceased patients did not significantly differ at baseline. The mortality rates were 27% and 39% at the intensive care unit and hospital, respectively. The severity indices that exhibited the greatest discriminative power with regard to mortality at the intensive care unit and hospital were the POP 0, POP 24, SOFA (at admission, 24 hours, 48 hours, and discharge), SAPS II, and APACHE II. CONCLUSION: The POP performed better than the other indices (aROC>0.8) at admission and 24 hours later (as originally described). The general physiological dysfunction indices also exhibited reasonable discriminative power (aROC=0.75-0.8), which was unlike the remaining pancreatitis specific indices, whose discriminative power was lower.
Abstract
Rev Bras Ter Intensiva. 2012;24(3):246-251
DOI 10.1590/S0103-507X2012000300007
OBJECTIVE: This study compared the general and specific severity indices to assess the prognosis of severe acute pancreatitis at a polyvalent intensive care unit. METHODS: This retrospective study included 108 patients who were diagnosed with severe acute pancreatitis from July 1, 1999 to March 31, 2012. Their demographic and clinical data were collected, and the following severity indices were calculated: Ranson, Osborne, Blamey and Imrie, Balthazar, POP, APACHE II, SAPS II, and SOFA. The discriminative power of these indices with regard to mortality at the intensive care unit and hospital was assessed using the area under the ROC curve. RESULTS: The demographic data of the surviving and deceased patients did not significantly differ at baseline. The mortality rates were 27% and 39% at the intensive care unit and hospital, respectively. The severity indices that exhibited the greatest discriminative power with regard to mortality at the intensive care unit and hospital were the POP 0, POP 24, SOFA (at admission, 24 hours, 48 hours, and discharge), SAPS II, and APACHE II. CONCLUSION: The POP performed better than the other indices (aROC>0.8) at admission and 24 hours later (as originally described). The general physiological dysfunction indices also exhibited reasonable discriminative power (aROC=0.75-0.8), which was unlike the remaining pancreatitis specific indices, whose discriminative power was lower.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):130-136
DOI 10.1590/S0103-507X2012000200006
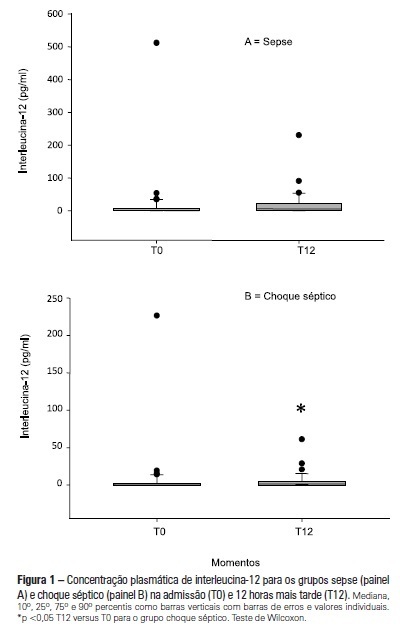
OBJECTIVE: To examine the behavior of interleukin-12 and verify whether it can be used to differentiate septic conditions in children. METHODS: Septic children aged between 28 days and 14 years, prospectively enrolled from 01/2004 to 12/2005, were divided into sepsis (SG; n=47) and septic shock (SSG; n=43) groups. Interleukin-12 levels were measured at admission (T0) and 12 hours later (T12). Disease severity was assessed by the PRISM score. RESULTS: Interleukin-12 levels did not differentiate children with sepsis from those with septic shock at admission [SSG: 0.24 (0-226.4)=SG: 1.23 (0-511.6); p=0.135)] and T12 [SG: 6.11 (0-230.5)=SSG: 1.32 (0-61.0); p=0.1239)]. Comparing time points, no significant difference was observed in the SG [SG, T0: 1.23 (0-511.6)=T12: 6.11 (0-230.5); p=0.075]. In SSG however, interleukin-12 increased from T0 to T12 (SSG, T0: 0.24 (0-226.4)
Abstract
Rev Bras Ter Intensiva. 2012;24(2):130-136
DOI 10.1590/S0103-507X2012000200006
OBJECTIVE: To examine the behavior of interleukin-12 and verify whether it can be used to differentiate septic conditions in children. METHODS: Septic children aged between 28 days and 14 years, prospectively enrolled from 01/2004 to 12/2005, were divided into sepsis (SG; n=47) and septic shock (SSG; n=43) groups. Interleukin-12 levels were measured at admission (T0) and 12 hours later (T12). Disease severity was assessed by the PRISM score. RESULTS: Interleukin-12 levels did not differentiate children with sepsis from those with septic shock at admission [SSG: 0.24 (0-226.4)=SG: 1.23 (0-511.6); p=0.135)] and T12 [SG: 6.11 (0-230.5)=SSG: 1.32 (0-61.0); p=0.1239)]. Comparing time points, no significant difference was observed in the SG [SG, T0: 1.23 (0-511.6)=T12: 6.11 (0-230.5); p=0.075]. In SSG however, interleukin-12 increased from T0 to T12 (SSG, T0: 0.24 (0-226.4)
Abstract
Rev Bras Ter Intensiva. 2012;24(2):157-161
DOI 10.1590/S0103-507X2012000200010
OBJECTIVE: Because patients hospitalized in intensive care units are at risk for poor nutrition, and nutritional therapy is not always started at an appropriate time, the present study aimed to correlate nutritional status, early nutrition, and hyperglycemia with patient mortality in an intensive care unit. METHODS: This archival cohort study used the secondary database of 453 patients who stayed at least 48 hours in an intensive care unit and were assessed for 8 days of hospitalization. Patient nutritional status was defined according to the body mass index. Early nutrition was defined as an feeding energy within the first 48 hours of hospitalization, regardless of the administration route. Blood glucose levels were monitored using a glucometer. RESULTS: A majority of patients were male (54.2%), and approximately half of patients were overweight (48.4%). At the end of the first 48 hours, 69.4% of patients had received nutrition, and only 13.5% of patients still exhibited hyperglycemia. The patients who received early nutritional therapy exhibited lower a mortality risk (p = 0.002), regardless of the presence of other factors associated with mortality. CONCLUSIONS: The significant correlation between early nutritional therapy and survival emphasizes the importance of nutrition in severely ill patients. The low frequency of hyperglycemia found in this study might indicate that the prescription of nutritional therapy and the application of an insulin protocol are appropriate at institutional intensive care units.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):157-161
DOI 10.1590/S0103-507X2012000200010
OBJECTIVE: Because patients hospitalized in intensive care units are at risk for poor nutrition, and nutritional therapy is not always started at an appropriate time, the present study aimed to correlate nutritional status, early nutrition, and hyperglycemia with patient mortality in an intensive care unit. METHODS: This archival cohort study used the secondary database of 453 patients who stayed at least 48 hours in an intensive care unit and were assessed for 8 days of hospitalization. Patient nutritional status was defined according to the body mass index. Early nutrition was defined as an feeding energy within the first 48 hours of hospitalization, regardless of the administration route. Blood glucose levels were monitored using a glucometer. RESULTS: A majority of patients were male (54.2%), and approximately half of patients were overweight (48.4%). At the end of the first 48 hours, 69.4% of patients had received nutrition, and only 13.5% of patients still exhibited hyperglycemia. The patients who received early nutritional therapy exhibited lower a mortality risk (p = 0.002), regardless of the presence of other factors associated with mortality. CONCLUSIONS: The significant correlation between early nutritional therapy and survival emphasizes the importance of nutrition in severely ill patients. The low frequency of hyperglycemia found in this study might indicate that the prescription of nutritional therapy and the application of an insulin protocol are appropriate at institutional intensive care units.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):197-206
DOI 10.1590/S0103-507X2012000200017
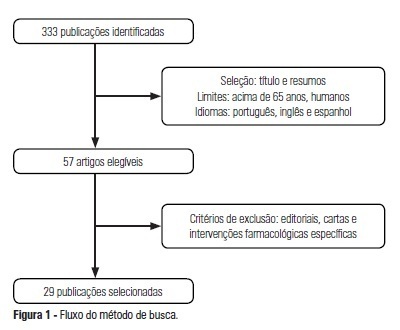
OBJECTIVE: The use of interventionist medical technology in terminal elderly patients must be associated with palliative care as a measure of clinical support in intensive care units. Palliative care is an important component of end-of-life care, and the assistance provided by the healthcare team should be guided by decisions made by patients and their family members. Prolongation of life not accompanied by therapies aimed at relieving symptoms, such as pain and dyspnea, contributes to patient and family member stress suffering. The aim of the present study was to survey advances made in the application of palliative care in intensive care units. METHODS: Medline and Bireme were used to perform a systematic literature review of intensive care units-based palliative care for elderly patients. RESULTS: A total of 29 articles describing palliative care in intensive care units were analyzed according to the variables "satisfaction of relatives when they participate in the discussions on palliative care" and "difficulties to implement such type of care due to lack of technical skills of the health caregivers." CONCLUSION: Palliative care for elderly patients in intensive care units must be more thoroughly investigated to improve the relationships and communication among patients, their relatives, and the healthcare team. As greater numbers of elderly patients are admitted to intensive care units, the skills of health caregivers must improve to meet the challenges posed by the end-of-life care.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):197-206
DOI 10.1590/S0103-507X2012000200017
OBJECTIVE: The use of interventionist medical technology in terminal elderly patients must be associated with palliative care as a measure of clinical support in intensive care units. Palliative care is an important component of end-of-life care, and the assistance provided by the healthcare team should be guided by decisions made by patients and their family members. Prolongation of life not accompanied by therapies aimed at relieving symptoms, such as pain and dyspnea, contributes to patient and family member stress suffering. The aim of the present study was to survey advances made in the application of palliative care in intensive care units. METHODS: Medline and Bireme were used to perform a systematic literature review of intensive care units-based palliative care for elderly patients. RESULTS: A total of 29 articles describing palliative care in intensive care units were analyzed according to the variables "satisfaction of relatives when they participate in the discussions on palliative care" and "difficulties to implement such type of care due to lack of technical skills of the health caregivers." CONCLUSION: Palliative care for elderly patients in intensive care units must be more thoroughly investigated to improve the relationships and communication among patients, their relatives, and the healthcare team. As greater numbers of elderly patients are admitted to intensive care units, the skills of health caregivers must improve to meet the challenges posed by the end-of-life care.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):6-22
DOI 10.1590/S0103-507X2012000100003
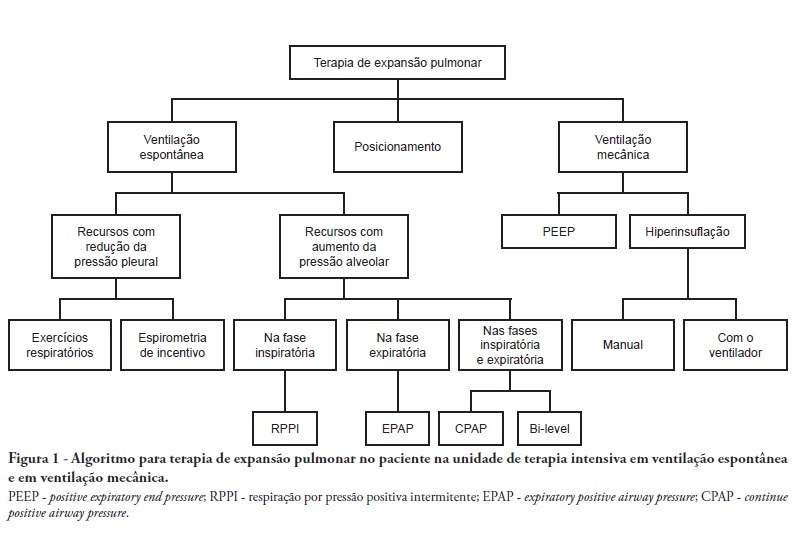
Complications from immobility in intensive care unit patients contribute to functional decline, increased healthcare costs, reduced quality of life and higher post-discharge mortality. Physical therapy focuses on promoting recovery and preserving function, and it may minimize the impact of these complications. A group of Brazilian Association of Intensive Care Medicine physical therapy experts developed this document that contains minimal physical therapy recommendations appropriate to the Brazilian real-world clinical situation. Prevention and treatment of atelectasis, procedures related to the removal of secretions and treatment of conditions related to physical deconditioning and functional decline are discussed. Equally important is the consideration that prescribing and executing activities, mobilizations and exercises are roles of the physical therapist, whose diagnosis should precede any intervention.
Abstract
Rev Bras Ter Intensiva. 2012;24(1):6-22
DOI 10.1590/S0103-507X2012000100003
Complications from immobility in intensive care unit patients contribute to functional decline, increased healthcare costs, reduced quality of life and higher post-discharge mortality. Physical therapy focuses on promoting recovery and preserving function, and it may minimize the impact of these complications. A group of Brazilian Association of Intensive Care Medicine physical therapy experts developed this document that contains minimal physical therapy recommendations appropriate to the Brazilian real-world clinical situation. Prevention and treatment of atelectasis, procedures related to the removal of secretions and treatment of conditions related to physical deconditioning and functional decline are discussed. Equally important is the consideration that prescribing and executing activities, mobilizations and exercises are roles of the physical therapist, whose diagnosis should precede any intervention.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):442-447
DOI 10.1590/S0103-507X2011000400008
INTRODUCTION: The importance of autopsies is a common theme of discussions both in Brazil and around the world as it elucidates causes of death and has wide ranging social value. However this is a practice that is gradually being considered unnecessary and there have been a decline in the number of postmortems examinations. OBJECTIVES: To compare clinical and pathological diagnosis in critically ill patients with difficult premortem diagnosis. METHODS: All autopsy cases (total of 98) from any of the three general medical/surgical intensive care units (78 beds in total) affiliated to the medical school from January 2003 to December 2006 were analyzed. We analyzed the clinical and pathological diagnosis based on the Goldman criteria. RESULTS: In 49 (50%) cases, there were class I and II of Goldman. In contrast, only 30 (30.6%) had a complete agreement between premortem and postmortem diagnosis and were classified as class V. Infections had a significantly greater rate of concordant diagnosis than cardiovascular diseases. CONCLUSION: We found significant discrepancies between clinical and pathological findings, reinforcing the value of postmortem examination.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):442-447
DOI 10.1590/S0103-507X2011000400008
INTRODUCTION: The importance of autopsies is a common theme of discussions both in Brazil and around the world as it elucidates causes of death and has wide ranging social value. However this is a practice that is gradually being considered unnecessary and there have been a decline in the number of postmortems examinations. OBJECTIVES: To compare clinical and pathological diagnosis in critically ill patients with difficult premortem diagnosis. METHODS: All autopsy cases (total of 98) from any of the three general medical/surgical intensive care units (78 beds in total) affiliated to the medical school from January 2003 to December 2006 were analyzed. We analyzed the clinical and pathological diagnosis based on the Goldman criteria. RESULTS: In 49 (50%) cases, there were class I and II of Goldman. In contrast, only 30 (30.6%) had a complete agreement between premortem and postmortem diagnosis and were classified as class V. Infections had a significantly greater rate of concordant diagnosis than cardiovascular diseases. CONCLUSION: We found significant discrepancies between clinical and pathological findings, reinforcing the value of postmortem examination.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):335-340
DOI 10.1590/S0103-507X2011000300012
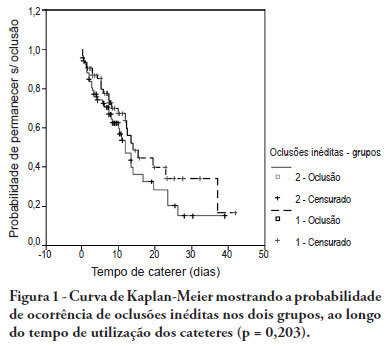
OBJECTIVE: To evaluate the effectiveness of intermittent 10 U/mL heparin flushes in reducing the occlusion of peripherally inserted central catheters in neonates. METHODS: In this randomized, open-label, prospective, controlled study, neonates were allocated either to receive 0.5 mL flushes of heparin (Group 1: n = 64) or saline (Group 2: n = 69) every 4 hours. Actions were taken to restore patency by using negative pressure (3-way stopcock method) in cases of occlusion. RESULTS: A total of 133 neonates were included. No significant intergroup difference was observed in the number of new occlusions (26 in Group 1, or 31/1,000 catheter-days; 36 in Group 2, or 36/1,000 catheter-days; P = 0.19). In Group 1, 5 catheters had 9 recurrent obstructions after successful clearance maneuvers. In Group 2, 19 catheters had 40 relapses (P < 0.0001), showing heparin's protective role against recurrence of obstruction (Relative Risk = 0.36). However, heparin failed to prevent catheter withdrawal due to permanent occlusion (3 catheters in Group 1 and 8 in Group 2; P = 0.24). CONCLUSION: Intermittent heparin is not effective for preventing the occlusion of peripherally inserted central catheters in neonates but reduces relapses when clearance maneuvers were successful
Abstract
Rev Bras Ter Intensiva. 2011;23(3):335-340
DOI 10.1590/S0103-507X2011000300012
OBJECTIVE: To evaluate the effectiveness of intermittent 10 U/mL heparin flushes in reducing the occlusion of peripherally inserted central catheters in neonates. METHODS: In this randomized, open-label, prospective, controlled study, neonates were allocated either to receive 0.5 mL flushes of heparin (Group 1: n = 64) or saline (Group 2: n = 69) every 4 hours. Actions were taken to restore patency by using negative pressure (3-way stopcock method) in cases of occlusion. RESULTS: A total of 133 neonates were included. No significant intergroup difference was observed in the number of new occlusions (26 in Group 1, or 31/1,000 catheter-days; 36 in Group 2, or 36/1,000 catheter-days; P = 0.19). In Group 1, 5 catheters had 9 recurrent obstructions after successful clearance maneuvers. In Group 2, 19 catheters had 40 relapses (P < 0.0001), showing heparin's protective role against recurrence of obstruction (Relative Risk = 0.36). However, heparin failed to prevent catheter withdrawal due to permanent occlusion (3 catheters in Group 1 and 8 in Group 2; P = 0.24). CONCLUSION: Intermittent heparin is not effective for preventing the occlusion of peripherally inserted central catheters in neonates but reduces relapses when clearance maneuvers were successful
Abstract
Rev Bras Ter Intensiva. 2011;23(2):242-248
DOI 10.1590/S0103-507X2011000200019
Levothyroxine absorption in hypothyroid patients can be influenced by several factors, particularly medications and concomitant food administration. This is especially evident in intensive care unit patients, where a continual enteral diet and the administration of multiple medications changes its absorption. Changes or adaptations in the hypothalamic-pituitary-thyroid axis, in conjunction with clinical abnormalities possibly related to under-treatment of hypothyroidism, render levothyroxine replacement therapy very challenging. Here, we report two intensive care hypothyroidism patients and their respective levothyroxine replacement management issues, focusing on a number of controversial issues, such as the optimal replacement dose, how fast the levothyroxine doses should be increased, triiodothyronine requirements, the interference of an enteral diet with absorption, and finally, the possible consequences of undertreated hypothyroidism and levothyroxine replacement monitoring useful clinical/laboratory parameters.
Abstract
Rev Bras Ter Intensiva. 2011;23(2):242-248
DOI 10.1590/S0103-507X2011000200019
Levothyroxine absorption in hypothyroid patients can be influenced by several factors, particularly medications and concomitant food administration. This is especially evident in intensive care unit patients, where a continual enteral diet and the administration of multiple medications changes its absorption. Changes or adaptations in the hypothalamic-pituitary-thyroid axis, in conjunction with clinical abnormalities possibly related to under-treatment of hypothyroidism, render levothyroxine replacement therapy very challenging. Here, we report two intensive care hypothyroidism patients and their respective levothyroxine replacement management issues, focusing on a number of controversial issues, such as the optimal replacement dose, how fast the levothyroxine doses should be increased, triiodothyronine requirements, the interference of an enteral diet with absorption, and finally, the possible consequences of undertreated hypothyroidism and levothyroxine replacement monitoring useful clinical/laboratory parameters.