Você pesquisou por y - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2024;36:e20240005en
DOI 10.62675/2965-2774.20240005-en
To investigate the factors influencing carbon dioxide transfer in a system that integrates an oxygenation membrane in series with high-bicarbonate continuous veno-venous hemodialysis in hypercapnic animals.
In an experimental setting, we induced severe acute kidney injury and hypercapnia in five female Landrace pigs. Subsequently, we initiated high (40mEq/L) bicarbonate continuous veno-venous hemodialysis with an oxygenation membrane in series to maintain a pH above 7.25. At intervals of 1 hour, 6 hours, and 12 hours following the initiation of continuous veno-venous hemodialysis, we performed standardized sweep gas flow titration to quantify carbon dioxide transfer. We evaluated factors associated with carbon dioxide transfer through the membrane lung with a mixed linear model.
A total of 20 sweep gas flow titration procedures were conducted, yielding 84 measurements of carbon dioxide transfer. Multivariate analysis revealed associations among the following (coefficients ± standard errors): core temperature (+7.8 ± 1.6 °C, p < 0.001), premembrane partial pressure of carbon dioxide (+0.2 ± 0.1/mmHg, p < 0.001), hemoglobin level (+3.5 ± 0.6/g/dL, p < 0.001), sweep gas flow (+6.2 ± 0.2/L/minute, p < 0.001), and arterial oxygen saturation (-0.5 ± 0.2%, p = 0.019). Among these variables, and within the physiological ranges evaluated, sweep gas flow was the primary modifiable factor influencing the efficacy of low-blood-flow carbon dioxide removal.
Sweep gas flow is the main carbon dioxide removal-related variable during continuous veno-venous hemodialysis with a high bicarbonate level coupled with an oxygenator. Other carbon dioxide transfer modulating variables included the hemoglobin level, arterial oxygen saturation, partial pressure of carbon dioxide and core temperature. These results should be interpreted as exploratory to inform other well-designed experimental or clinical studies.
Abstract
Crit Care Sci. 2024;36:e20240005en
DOI 10.62675/2965-2774.20240005-en
To investigate the factors influencing carbon dioxide transfer in a system that integrates an oxygenation membrane in series with high-bicarbonate continuous veno-venous hemodialysis in hypercapnic animals.
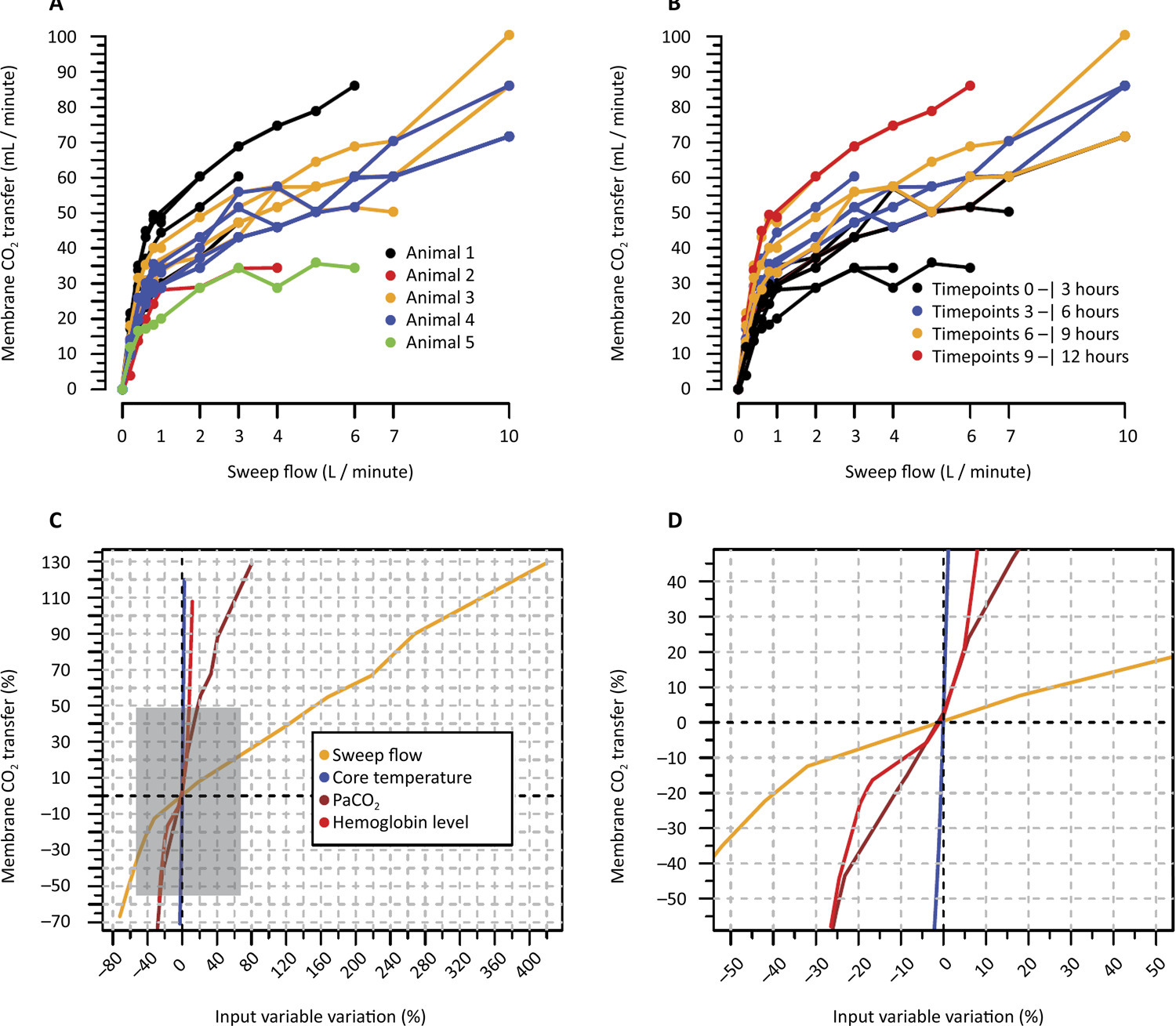
In an experimental setting, we induced severe acute kidney injury and hypercapnia in five female Landrace pigs. Subsequently, we initiated high (40mEq/L) bicarbonate continuous veno-venous hemodialysis with an oxygenation membrane in series to maintain a pH above 7.25. At intervals of 1 hour, 6 hours, and 12 hours following the initiation of continuous veno-venous hemodialysis, we performed standardized sweep gas flow titration to quantify carbon dioxide transfer. We evaluated factors associated with carbon dioxide transfer through the membrane lung with a mixed linear model.
A total of 20 sweep gas flow titration procedures were conducted, yielding 84 measurements of carbon dioxide transfer. Multivariate analysis revealed associations among the following (coefficients ± standard errors): core temperature (+7.8 ± 1.6 °C, p < 0.001), premembrane partial pressure of carbon dioxide (+0.2 ± 0.1/mmHg, p < 0.001), hemoglobin level (+3.5 ± 0.6/g/dL, p < 0.001), sweep gas flow (+6.2 ± 0.2/L/minute, p < 0.001), and arterial oxygen saturation (-0.5 ± 0.2%, p = 0.019). Among these variables, and within the physiological ranges evaluated, sweep gas flow was the primary modifiable factor influencing the efficacy of low-blood-flow carbon dioxide removal.
Sweep gas flow is the main carbon dioxide removal-related variable during continuous veno-venous hemodialysis with a high bicarbonate level coupled with an oxygenator. Other carbon dioxide transfer modulating variables included the hemoglobin level, arterial oxygen saturation, partial pressure of carbon dioxide and core temperature. These results should be interpreted as exploratory to inform other well-designed experimental or clinical studies.
Abstract
Crit Care Sci. 2024;36:e20240253en
DOI 10.62675/2965-2774.20240253-en
To identify the influence of obesity on mortality, time to weaning from mechanical ventilation and mobility at intensive care unit discharge in patients with COVID-19.
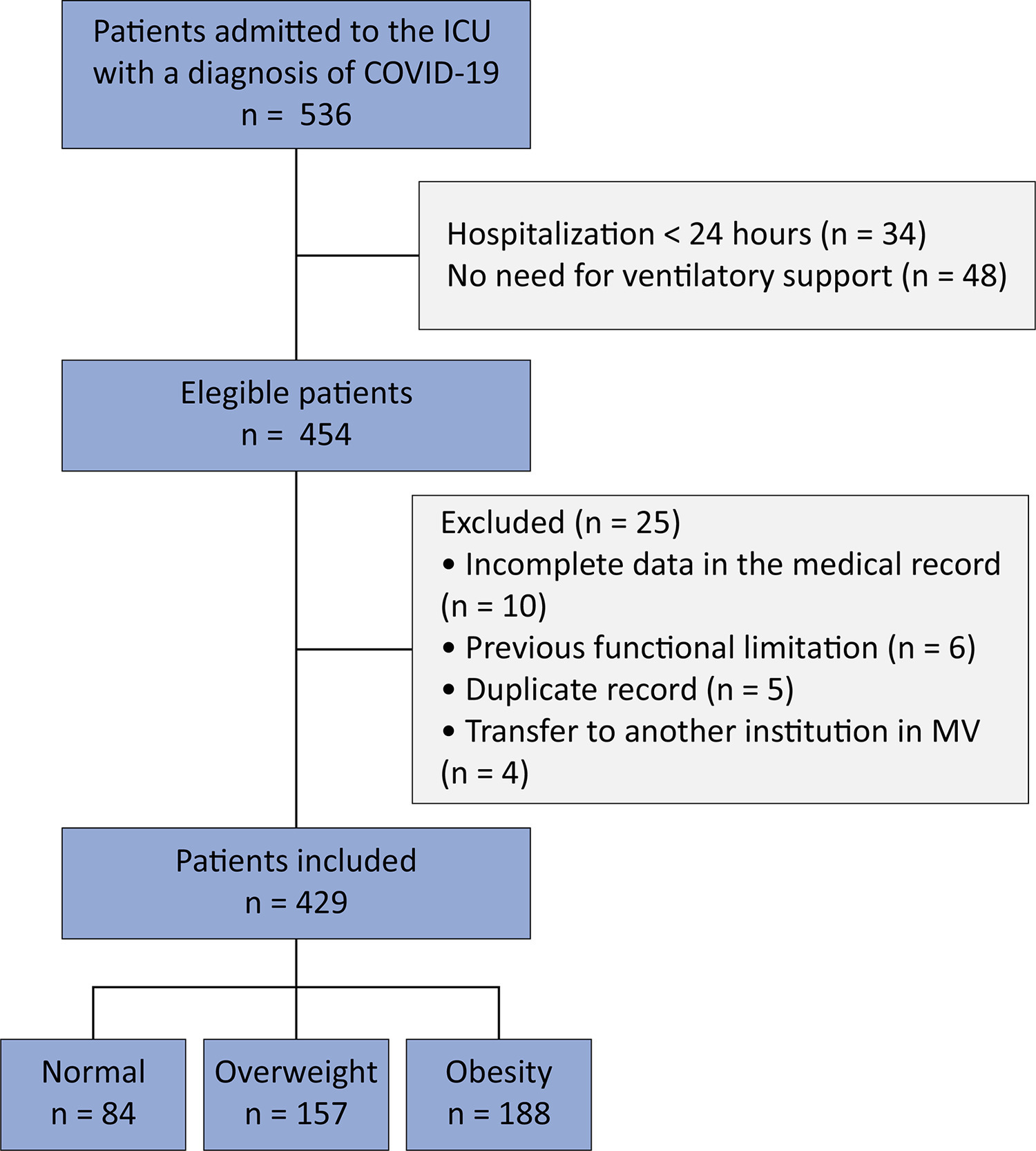
This retrospective cohort study was carried out between March and August 2020. All adult patients admitted to the intensive care unit in need of ventilatory support and confirmed to have COVID-19 were included. The outcomes included mortality, time on mechanical ventilation, and mobility at intensive care unit discharge.
Four hundred and twenty-nine patients were included, 36.6% of whom were overweight and 43.8% of whom were obese. Compared with normal body mass index patients, overweight and obese patients had lower mortality (p = 0.002) and longer intensive care unit survival (log-rank p < 0.001). Compared with patients with a normal body mass index, overweight patients had a 36% lower risk of death (p = 0.04), while patients with obesity presented a 23% lower risk (p < 0.001). There was no association between obesity and time on mechanical ventilation. The level of mobility at intensive care unit discharge did not differ between groups and showed a moderate inverse correlation with length of stay in the intensive care unit (r = -0.461; p < 0.001).
Overweight and obese patients had lower mortality and higher intensive care unit survival rates. The duration of mechanical ventilation and mobility level at intensive care unit discharge did not differ between the groups.
Abstract
Crit Care Sci. 2024;36:e20240253en
DOI 10.62675/2965-2774.20240253-en
To identify the influence of obesity on mortality, time to weaning from mechanical ventilation and mobility at intensive care unit discharge in patients with COVID-19.
This retrospective cohort study was carried out between March and August 2020. All adult patients admitted to the intensive care unit in need of ventilatory support and confirmed to have COVID-19 were included. The outcomes included mortality, time on mechanical ventilation, and mobility at intensive care unit discharge.
Four hundred and twenty-nine patients were included, 36.6% of whom were overweight and 43.8% of whom were obese. Compared with normal body mass index patients, overweight and obese patients had lower mortality (p = 0.002) and longer intensive care unit survival (log-rank p < 0.001). Compared with patients with a normal body mass index, overweight patients had a 36% lower risk of death (p = 0.04), while patients with obesity presented a 23% lower risk (p < 0.001). There was no association between obesity and time on mechanical ventilation. The level of mobility at intensive care unit discharge did not differ between groups and showed a moderate inverse correlation with length of stay in the intensive care unit (r = -0.461; p < 0.001).
Overweight and obese patients had lower mortality and higher intensive care unit survival rates. The duration of mechanical ventilation and mobility level at intensive care unit discharge did not differ between the groups.
Abstract
Crit Care Sci. 2024;36:e20240040en
DOI 10.62675/2965-2774.20240040-en
Abstract
Crit Care Sci. 2024;36:e20240040en
DOI 10.62675/2965-2774.20240040-en
Abstract
Crit Care Sci. 2024;36:e20240203en
DOI 10.62675/2965-2774.20240203-en
To assess whether the respiratory oxygenation index (ROX index) measured after the start of high-flow nasal cannula oxygen therapy can help identify the need for intubation in patients with acute respiratory failure due to coronavirus disease 2019.
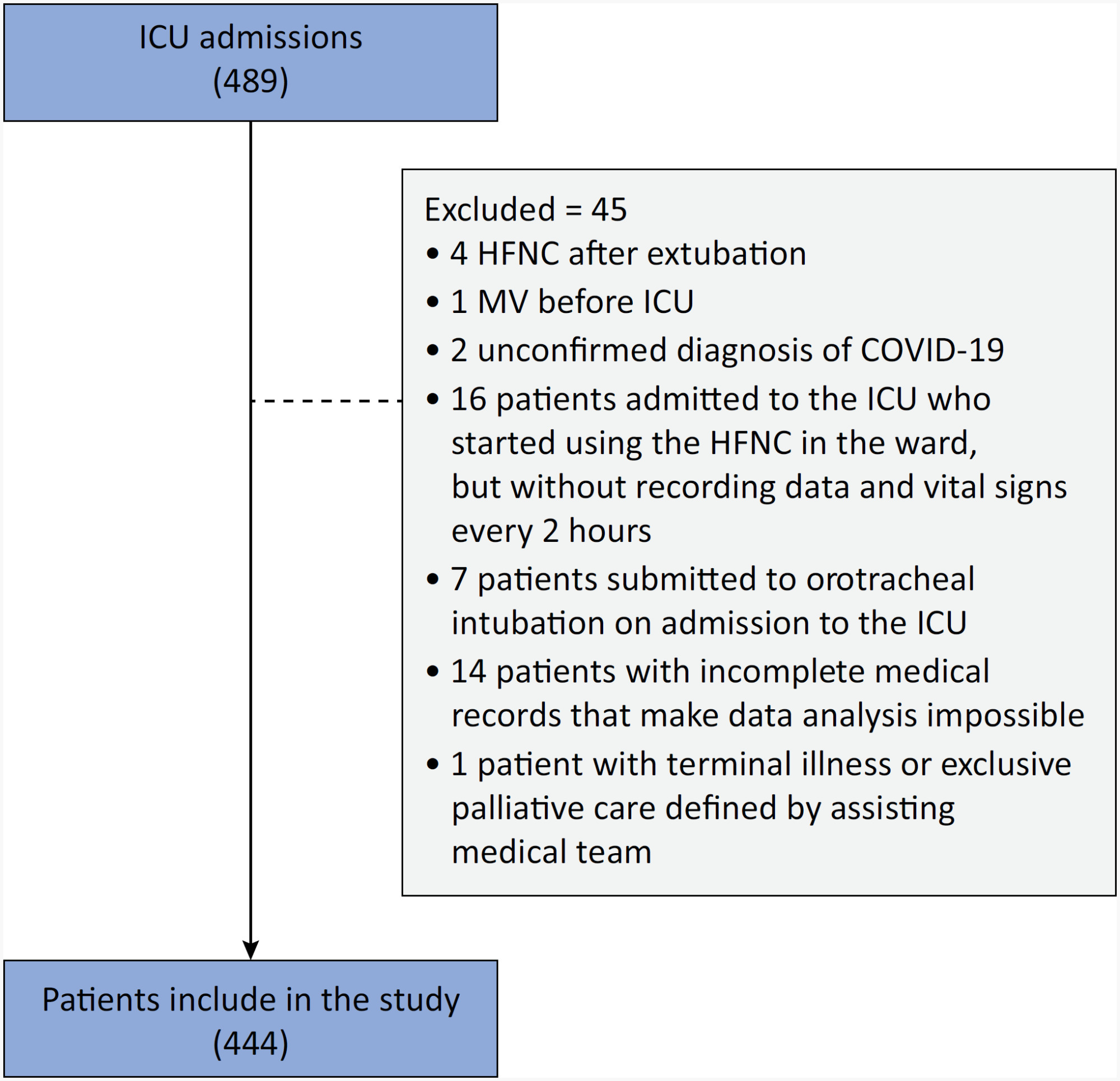
This retrospective, observational, multicenter study was conducted at the intensive care units of six Brazilian hospitals from March to December 2020. The primary outcome was the need for intubation up to 7 days after starting the high-flow nasal cannula.
A total of 444 patients were included in the study, and 261 (58.7%) were subjected to intubation. An analysis of the area under the receiver operating characteristic curve (AUROC) showed that the ability to discriminate between successful and failed high-flow nasal cannula oxygen therapy within 7 days was greater for the ROX index measured at 24 hours (AUROC 0.80; 95%CI 0.76 - 0.84). The median interval between high-flow nasal cannula initiation and intubation was 24 hours (24 - 72), and the most accurate predictor of intubation obtained before 24 hours was the ROX index measured at 12 hours (AUROC 0.75; 95%CI 0.70 - 0.79). Kaplan-Meier curves revealed a greater probability of intubation within 7 days in patients with a ROX index ≤ 5.54 at 12 hours (hazard ratio 3.07; 95%CI 2.24 - 4.20) and ≤ 5.96 at 24 hours (hazard ratio 5.15; 95%CI 3.65 - 7.27).
The ROX index can aid in the early identification of patients with acute respiratory failure due to COVID-19 who will progress to the failure of high-flow nasal cannula supportive therapy and the need for intubation.
Abstract
Crit Care Sci. 2024;36:e20240203en
DOI 10.62675/2965-2774.20240203-en
To assess whether the respiratory oxygenation index (ROX index) measured after the start of high-flow nasal cannula oxygen therapy can help identify the need for intubation in patients with acute respiratory failure due to coronavirus disease 2019.
This retrospective, observational, multicenter study was conducted at the intensive care units of six Brazilian hospitals from March to December 2020. The primary outcome was the need for intubation up to 7 days after starting the high-flow nasal cannula.
A total of 444 patients were included in the study, and 261 (58.7%) were subjected to intubation. An analysis of the area under the receiver operating characteristic curve (AUROC) showed that the ability to discriminate between successful and failed high-flow nasal cannula oxygen therapy within 7 days was greater for the ROX index measured at 24 hours (AUROC 0.80; 95%CI 0.76 - 0.84). The median interval between high-flow nasal cannula initiation and intubation was 24 hours (24 - 72), and the most accurate predictor of intubation obtained before 24 hours was the ROX index measured at 12 hours (AUROC 0.75; 95%CI 0.70 - 0.79). Kaplan-Meier curves revealed a greater probability of intubation within 7 days in patients with a ROX index ≤ 5.54 at 12 hours (hazard ratio 3.07; 95%CI 2.24 - 4.20) and ≤ 5.96 at 24 hours (hazard ratio 5.15; 95%CI 3.65 - 7.27).
The ROX index can aid in the early identification of patients with acute respiratory failure due to COVID-19 who will progress to the failure of high-flow nasal cannula supportive therapy and the need for intubation.
Abstract
Crit Care Sci. 2024;36:e20240260en
DOI 10.62675/2965-2774.20240260-en
Abstract
Crit Care Sci. 2024;36:e20240260en
DOI 10.62675/2965-2774.20240260-en
Abstract
Crit Care Sci. 2024;36:e20240284en
DOI 10.62675/2965-2774.20240284-en
To examine the physical function and respiratory muscle strength of patients - who recovered from critical COVID-19 – after intensive care unit discharge to the ward on Days one (D1) and seven (D7), and to investigate variables associated with functional impairment.
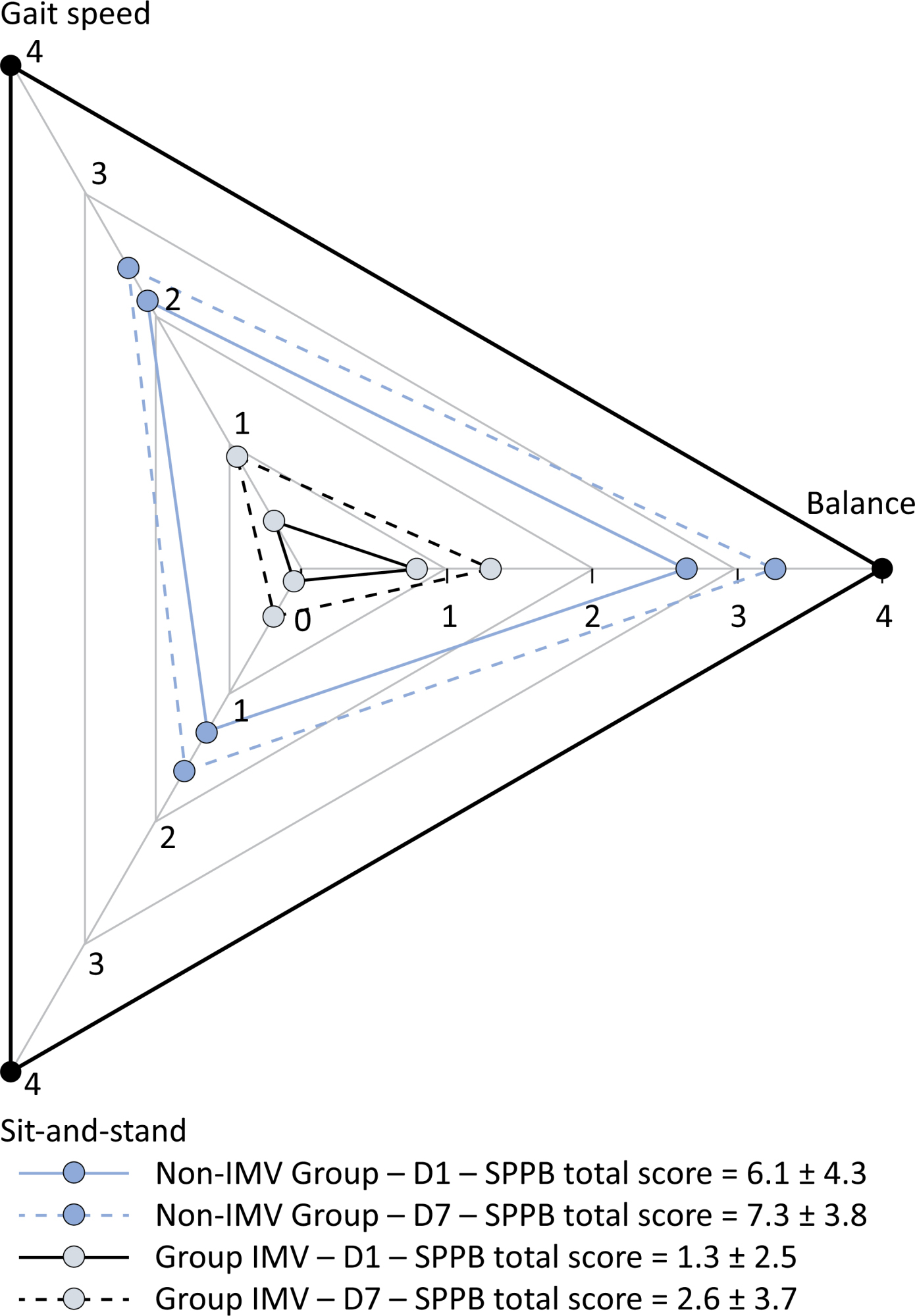
This was a prospective cohort study of adult patients with COVID-19 who needed invasive mechanical ventilation, non-invasive ventilation or high-flow nasal cannula and were discharged from the intensive care unit to the ward. Participants were submitted to Medical Research Council sum-score, handgrip strength, maximal inspiratory pressure, maximal expiratory pressure, and short physical performance battery tests. Participants were grouped into two groups according to their need for invasive ventilation: the Invasive Mechanical Ventilation Group (IMV Group) and the Non-Invasive Mechanical Ventilation Group (Non-IMV Group).
Patients in the IMV Group (n = 31) were younger and had higher Sequential Organ Failure Assessment scores than those in the Non-IMV Group (n = 33). The short physical performance battery scores (range 0 - 12) on D1 and D7 were 6.1 ± 4.3 and 7.3 ± 3.8, respectively for the Non-Invasive Mechanical Ventilation Group, and 1.3 ± 2.5 and 2.6 ± 3.7, respectively for the IMV Group. The prevalence of intensive care unit-acquired weakness on D7 was 13% for the Non-IMV Group and 72% for the IMV Group. The maximal inspiratory pressure, maximal expiratory pressure, and handgrip strength increased on D7 in both groups, but the maximal expiratory pressure and handgrip strength were still weak. Only maximal inspiratory pressure was recovered (i.e., > 80% of the predicted value) in the Non-IMV Group. Female sex, and the need and duration of invasive mechanical were independently and negatively associated with the short physical performance battery score and handgrip strength.
Patients who recovered from critical COVID-19 and who received invasive mechanical ventilation presented greater disability than those who were not invasively ventilated. However, they both showed marginal functional improvement during early recovery, regardless of the need for invasive mechanical ventilation. This might highlight the severity of disability caused by SARS-CoV-2.
Abstract
Crit Care Sci. 2024;36:e20240284en
DOI 10.62675/2965-2774.20240284-en
To examine the physical function and respiratory muscle strength of patients - who recovered from critical COVID-19 – after intensive care unit discharge to the ward on Days one (D1) and seven (D7), and to investigate variables associated with functional impairment.
This was a prospective cohort study of adult patients with COVID-19 who needed invasive mechanical ventilation, non-invasive ventilation or high-flow nasal cannula and were discharged from the intensive care unit to the ward. Participants were submitted to Medical Research Council sum-score, handgrip strength, maximal inspiratory pressure, maximal expiratory pressure, and short physical performance battery tests. Participants were grouped into two groups according to their need for invasive ventilation: the Invasive Mechanical Ventilation Group (IMV Group) and the Non-Invasive Mechanical Ventilation Group (Non-IMV Group).
Patients in the IMV Group (n = 31) were younger and had higher Sequential Organ Failure Assessment scores than those in the Non-IMV Group (n = 33). The short physical performance battery scores (range 0 - 12) on D1 and D7 were 6.1 ± 4.3 and 7.3 ± 3.8, respectively for the Non-Invasive Mechanical Ventilation Group, and 1.3 ± 2.5 and 2.6 ± 3.7, respectively for the IMV Group. The prevalence of intensive care unit-acquired weakness on D7 was 13% for the Non-IMV Group and 72% for the IMV Group. The maximal inspiratory pressure, maximal expiratory pressure, and handgrip strength increased on D7 in both groups, but the maximal expiratory pressure and handgrip strength were still weak. Only maximal inspiratory pressure was recovered (i.e., > 80% of the predicted value) in the Non-IMV Group. Female sex, and the need and duration of invasive mechanical were independently and negatively associated with the short physical performance battery score and handgrip strength.
Patients who recovered from critical COVID-19 and who received invasive mechanical ventilation presented greater disability than those who were not invasively ventilated. However, they both showed marginal functional improvement during early recovery, regardless of the need for invasive mechanical ventilation. This might highlight the severity of disability caused by SARS-CoV-2.
Abstract
Crit Care Sci. 2024;36:e20240058en
DOI 10.62675/2965-2774.20240058-en
Abstract
Crit Care Sci. 2024;36:e20240058en
DOI 10.62675/2965-2774.20240058-en
Abstract
Crit Care Sci. 2024;36:e20240068en
DOI 10.62675/2965-2774.20240068-en
To identify factors associated with hospitalization in the intensive care unit in children and adolescents with COVID-19.
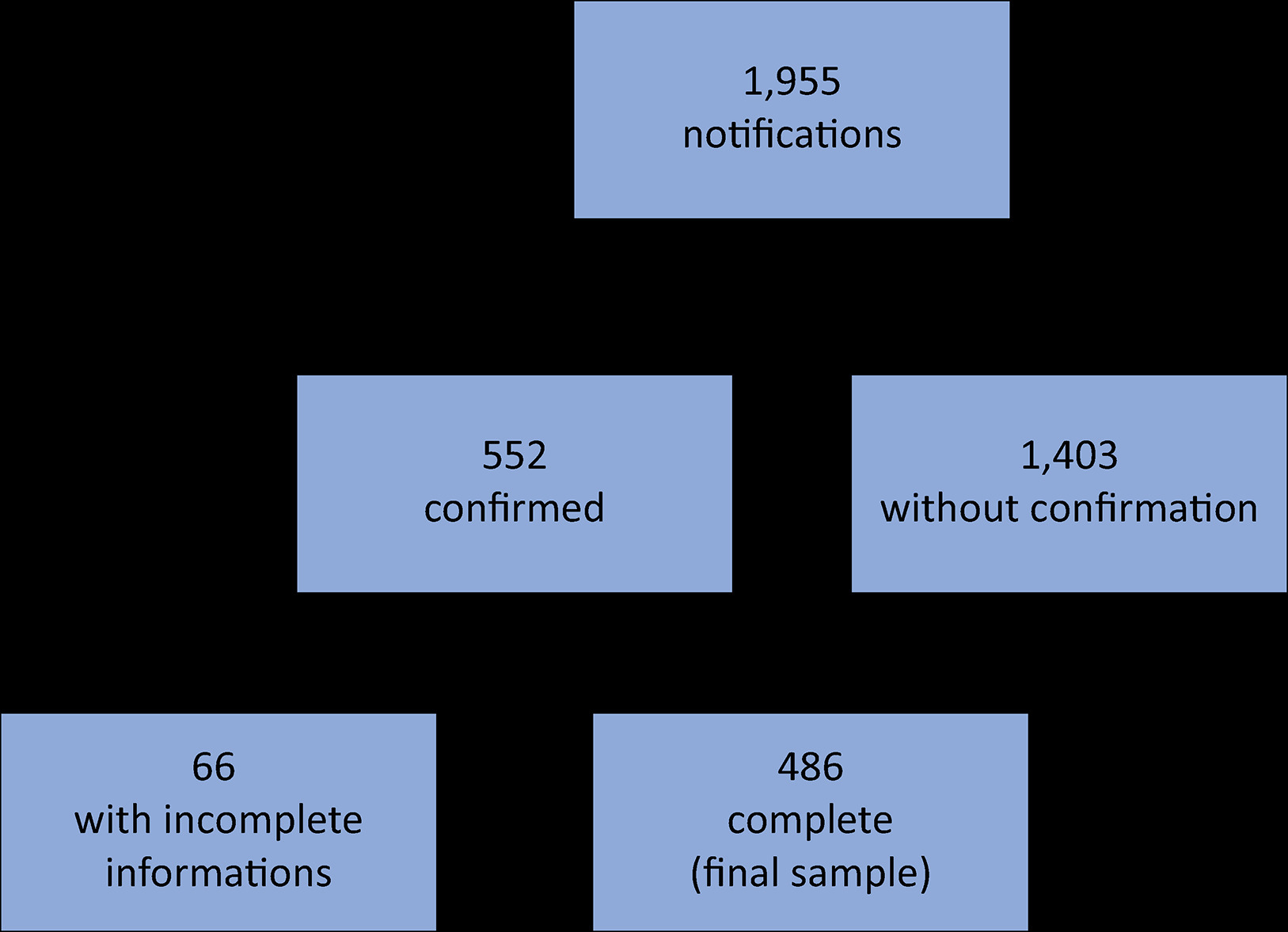
This was a retrospective cohort study using secondary data of hospitalized children and adolescents (zero to 18 years old) with COVID-19 reported in Paraíba from April 2020 to July 2021, totaling 486 records. Descriptive analysis, logistic regression and multilevel regression were performed, utilizing a significance level of 5%.
According to logistic regression without hierarchical levels, there was an increased chance of admission to the intensive care unit for male patients (OR = 1.98; 95%CI 1.18 - 3.32), patients with respiratory distress (OR = 2.43; 95%CI 1.29 - 4.56), patients with dyspnea (OR = 3.57; 95%CI 1.77 - 7.18) and patients living in large cities (OR = 2.70; 95%CI 1.07 - 6.77). The likelihood of requiring intensive care was observed to decrease with increasing age (OR = 0.94; 95%CI = 0.90 - 0.97), the presence of cough (OR = 0.32; 95%CI 0.18 - 0.59) or fever (OR = 0.42; 95%CI 0.23 - 0.74) and increasing Gini index (OR = 0.003; 95%CI 0.000 - 0.243). According to the multilevel analysis, the odds of admission to the intensive care unit increased in male patients (OR = 1.70; 95%CI = 1.68-1.71) and with increasing population size of the municipality per 100,000 inhabitants (OR = 1.01; 95%CI 1.01-1.03); additionally, the odds of admission to the intensive care unit decreased for mixed-race versus non-brown-skinned patients (OR = 0.981; 95%CI 0.97 - 0.99) and increasing Gini index (OR = 0.02; 95%CI 0.02 - 0.02).
The effects of patient characteristics and social context on the need for intensive care in children and adolescents with SARS-CoV-2 infection were better estimated with the inclusion of a multilevel regression model.
Abstract
Crit Care Sci. 2024;36:e20240068en
DOI 10.62675/2965-2774.20240068-en
To identify factors associated with hospitalization in the intensive care unit in children and adolescents with COVID-19.
This was a retrospective cohort study using secondary data of hospitalized children and adolescents (zero to 18 years old) with COVID-19 reported in Paraíba from April 2020 to July 2021, totaling 486 records. Descriptive analysis, logistic regression and multilevel regression were performed, utilizing a significance level of 5%.
According to logistic regression without hierarchical levels, there was an increased chance of admission to the intensive care unit for male patients (OR = 1.98; 95%CI 1.18 - 3.32), patients with respiratory distress (OR = 2.43; 95%CI 1.29 - 4.56), patients with dyspnea (OR = 3.57; 95%CI 1.77 - 7.18) and patients living in large cities (OR = 2.70; 95%CI 1.07 - 6.77). The likelihood of requiring intensive care was observed to decrease with increasing age (OR = 0.94; 95%CI = 0.90 - 0.97), the presence of cough (OR = 0.32; 95%CI 0.18 - 0.59) or fever (OR = 0.42; 95%CI 0.23 - 0.74) and increasing Gini index (OR = 0.003; 95%CI 0.000 - 0.243). According to the multilevel analysis, the odds of admission to the intensive care unit increased in male patients (OR = 1.70; 95%CI = 1.68-1.71) and with increasing population size of the municipality per 100,000 inhabitants (OR = 1.01; 95%CI 1.01-1.03); additionally, the odds of admission to the intensive care unit decreased for mixed-race versus non-brown-skinned patients (OR = 0.981; 95%CI 0.97 - 0.99) and increasing Gini index (OR = 0.02; 95%CI 0.02 - 0.02).
The effects of patient characteristics and social context on the need for intensive care in children and adolescents with SARS-CoV-2 infection were better estimated with the inclusion of a multilevel regression model.