
You searched for:"Lívia Barboza de Andrade"
We found (4) results for your search.-
Original Articles
Noninvasive ventilation as the first choice of ventilatory support in children
Rev Bras Ter Intensiva. 2019;31(3):333-339
Abstract
Original ArticlesNoninvasive ventilation as the first choice of ventilatory support in children
Rev Bras Ter Intensiva. 2019;31(3):333-339
DOI 10.5935/0103-507X.20190045
Views0ABSTRACT
Objective:
To describe the use of noninvasive ventilation to prevent tracheal intubation in children in a pediatric intensive care unit and to analyze the factors related to respiratory failure.
Methods:
A retrospective cohort study was performed from January 2016 to May 2018. The study population included children aged 1 to 14 years who were subjected to noninvasive ventilation as the first therapeutic choice for acute respiratory failure. Biological, clinical and managerial data were analyzed by applying a model with the variables that obtained significance ≤ 0.20 in a bivariate analysis. Logistic regression was performed using the ENTER method. The level of significance was set at 5%.
Results:
The children had a mean age of 68.7 ± 42.3 months, 96.6% had respiratory disease as a primary diagnosis, and 15.8% had comorbidities. Of the 209 patients, noninvasive ventilation was the first option for ventilatory support in 86.6% of the patients, and the fraction of inspired oxygen was ≥ 0.40 in 47% of the cases. The lethality rate was 1.4%. The data for the use of noninvasive ventilation showed a high success rate of 95.3% (84.32 – 106). The Pediatric Risk of Mortality (PRISM) score and the length of stay in the intensive care unit were the significant clinical variables for the success or failure of noninvasive ventilation.
Conclusion:
A high rate of effectiveness was found for the use of noninvasive ventilation for acute episodes of respiratory failure. A higher PRISM score on admission, comorbidities associated with respiratory symptoms and oxygen use ≥ 40% were independent factors related to noninvasive ventilation failure.
Keywords:ChildComorbidityIntensive care units, pediatricNoninvasive ventilationRespiratory insufficiencyVentilatory supportSee moreViews0

Abstract
Original ArticlesNoninvasive ventilation as the first choice of ventilatory support in children
Rev Bras Ter Intensiva. 2019;31(3):333-339
DOI 10.5935/0103-507X.20190045
Views0ABSTRACT
Objective:
To describe the use of noninvasive ventilation to prevent tracheal intubation in children in a pediatric intensive care unit and to analyze the factors related to respiratory failure.
Methods:
A retrospective cohort study was performed from January 2016 to May 2018. The study population included children aged 1 to 14 years who were subjected to noninvasive ventilation as the first therapeutic choice for acute respiratory failure. Biological, clinical and managerial data were analyzed by applying a model with the variables that obtained significance ≤ 0.20 in a bivariate analysis. Logistic regression was performed using the ENTER method. The level of significance was set at 5%.
Results:
The children had a mean age of 68.7 ± 42.3 months, 96.6% had respiratory disease as a primary diagnosis, and 15.8% had comorbidities. Of the 209 patients, noninvasive ventilation was the first option for ventilatory support in 86.6% of the patients, and the fraction of inspired oxygen was ≥ 0.40 in 47% of the cases. The lethality rate was 1.4%. The data for the use of noninvasive ventilation showed a high success rate of 95.3% (84.32 – 106). The Pediatric Risk of Mortality (PRISM) score and the length of stay in the intensive care unit were the significant clinical variables for the success or failure of noninvasive ventilation.
Conclusion:
A high rate of effectiveness was found for the use of noninvasive ventilation for acute episodes of respiratory failure. A higher PRISM score on admission, comorbidities associated with respiratory symptoms and oxygen use ≥ 40% were independent factors related to noninvasive ventilation failure.
Keywords:ChildComorbidityIntensive care units, pediatricNoninvasive ventilationRespiratory insufficiencyVentilatory supportSee more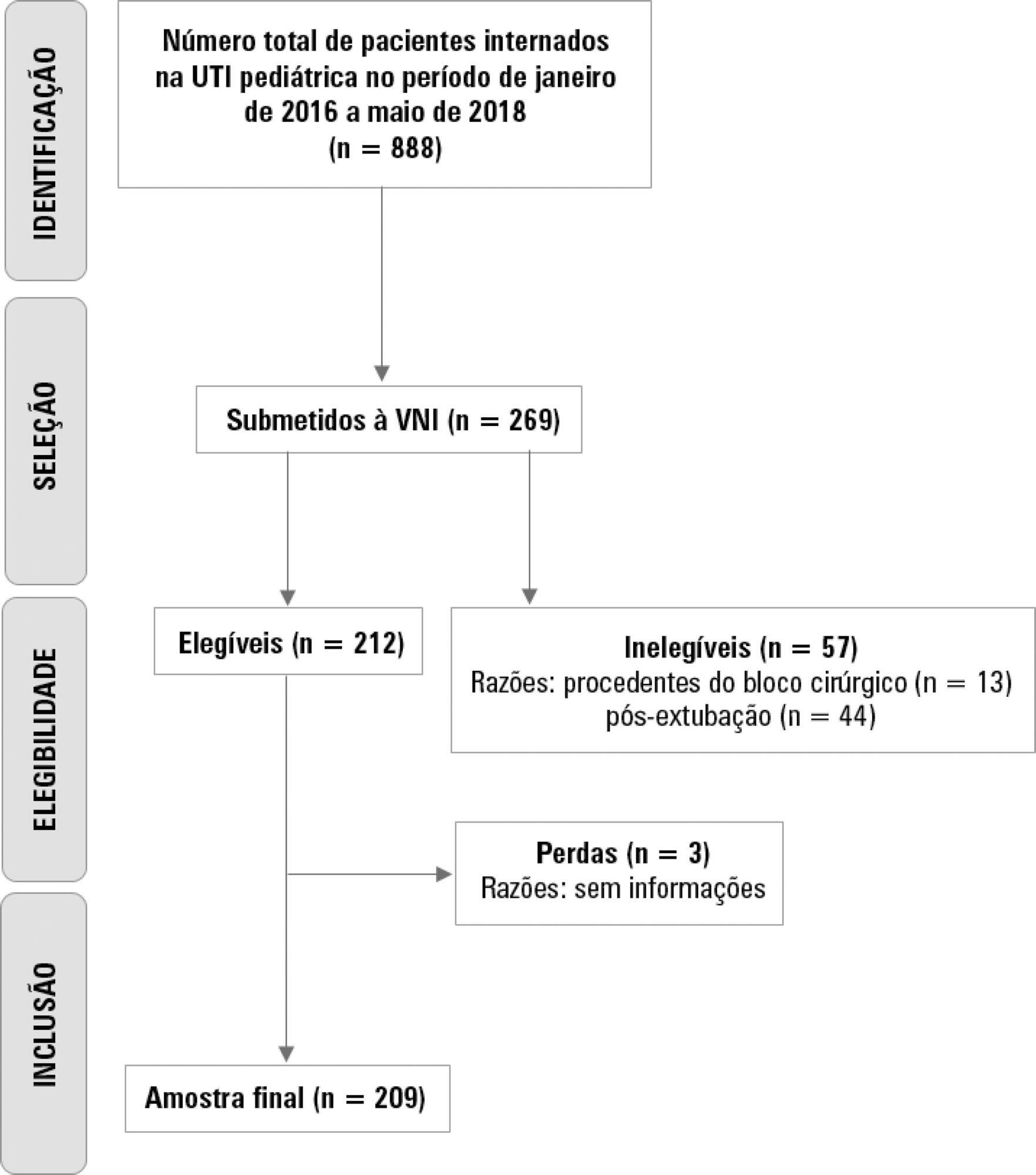
-
Original Article
Brazilian version of the Pediatric Functional Status Scale: translation and cross-cultural adaptation
Rev Bras Ter Intensiva. 2018;30(3):301-307
Abstract
Original ArticleBrazilian version of the Pediatric Functional Status Scale: translation and cross-cultural adaptation
Rev Bras Ter Intensiva. 2018;30(3):301-307
DOI 10.5935/0103-507X.20180043
Views0ABSTRACT
Objective:
To translate and cross-culturally adapt the Functional Status Scale for hospitalized children into Brazilian Portuguese.
Methods:
A methodological study of the translation and cross-cultural adaptation of the Functional Status Scale was conducted, according to the stages of translation, synthesis of translations, back-translation, synthesis of back-translations, expert committee analysis and pre-test with a sample of the target population. During the evaluation by the committee of experts, semantic, content and item analyses were performed.
Results:
The semantic, idiomatic, cultural and conceptual equivalences between the translated version and the original version were obtained, resulting in the Brazilian version of the Functional Status Scale. After the analysis by the expert committee, there were no problems regarding the cultural or conceptual equivalences because the items were pertinent to the Brazilian culture and few terms were modified. In the pre-test stage, the scale was applied by two evaluators to a sample of 25 children. Clarity and ease in answering the scale items were observed. Good inter-observer reliability was obtained, with an intraclass correlation coefficient of 0.85 (0.59 – 0.95).
Conclusions:
The Functional Status Scale for pediatric use was translated and culturally adapted into Portuguese spoken in Brazil. The translated items were pertinent to the Brazilian culture and evaluated the dimensions proposed by the original instrument. Validation studies of this instrument are suggested to make it feasible for use in different regions of Brazil.
Keywords:ChildIntensive care unitsintensive therapySemanticsSurveys and questionnairesTranslationsValidation studiesSee moreViews0Abstract
Original ArticleBrazilian version of the Pediatric Functional Status Scale: translation and cross-cultural adaptation
Rev Bras Ter Intensiva. 2018;30(3):301-307
DOI 10.5935/0103-507X.20180043
Views0ABSTRACT
Objective:
To translate and cross-culturally adapt the Functional Status Scale for hospitalized children into Brazilian Portuguese.
Methods:
A methodological study of the translation and cross-cultural adaptation of the Functional Status Scale was conducted, according to the stages of translation, synthesis of translations, back-translation, synthesis of back-translations, expert committee analysis and pre-test with a sample of the target population. During the evaluation by the committee of experts, semantic, content and item analyses were performed.
Results:
The semantic, idiomatic, cultural and conceptual equivalences between the translated version and the original version were obtained, resulting in the Brazilian version of the Functional Status Scale. After the analysis by the expert committee, there were no problems regarding the cultural or conceptual equivalences because the items were pertinent to the Brazilian culture and few terms were modified. In the pre-test stage, the scale was applied by two evaluators to a sample of 25 children. Clarity and ease in answering the scale items were observed. Good inter-observer reliability was obtained, with an intraclass correlation coefficient of 0.85 (0.59 – 0.95).
Conclusions:
The Functional Status Scale for pediatric use was translated and culturally adapted into Portuguese spoken in Brazil. The translated items were pertinent to the Brazilian culture and evaluated the dimensions proposed by the original instrument. Validation studies of this instrument are suggested to make it feasible for use in different regions of Brazil.
Keywords:ChildIntensive care unitsintensive therapySemanticsSurveys and questionnairesTranslationsValidation studiesSee more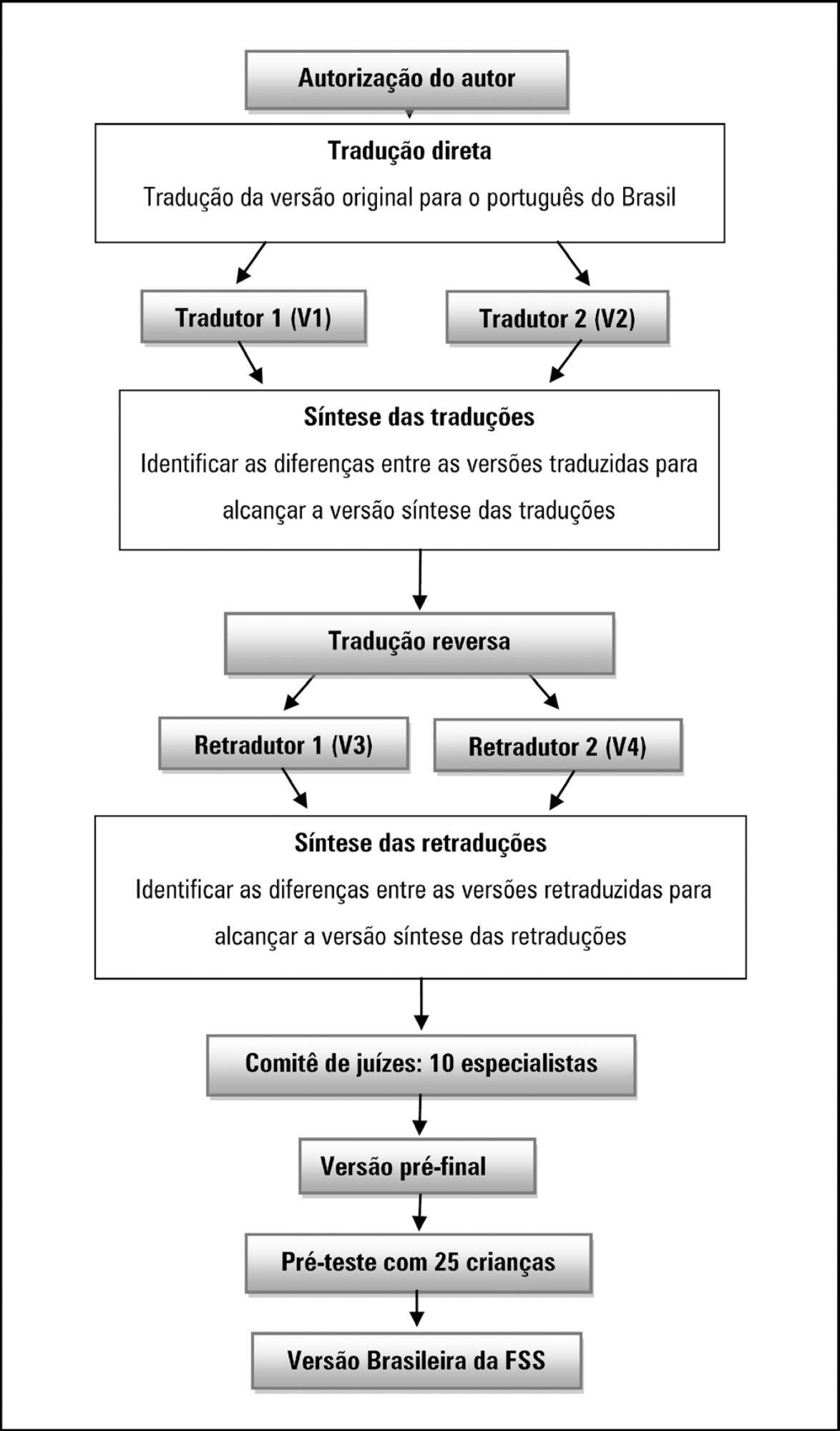
-
Original Articles
Translation and cross-cultural adaptation of the Cornell Assessment of Pediatric Delirium scale for the Portuguese language
Rev Bras Ter Intensiva. 2018;30(2):195-200
Abstract
Original ArticlesTranslation and cross-cultural adaptation of the Cornell Assessment of Pediatric Delirium scale for the Portuguese language
Rev Bras Ter Intensiva. 2018;30(2):195-200
DOI 10.5935/0103-507X.20180033
Views0See moreABSTRACT
Objective:
This study sought to translate the Cornell Assessment of Pediatric Delirium from English into Brazilian Portuguese and cross-culturally adapt it for use in Brazil.
Methods:
Following the authorization granted by its main author, the processes of translation and cross-cultural adaptation were performed with regard to the Cornell Assessment of Pediatric Delirium in accordance with the following internationally recommended steps: translation of the original into Portuguese by two native speakers of the target language; synthesis of the translated versions; back-translation by two native speakers of the original language; review and harmonization of the back-translation; a review of the Portuguese version of the Cornell Assessment of Pediatric Delirium by an expert panel composed of specialists; pretesting including assessments of clarity, comprehensibility, and acceptability of the translated version using a sample of the target population; and finishing modifications to achieve the final version.
Results:
The translation and cross-cultural adaptation of the Cornell Assessment of Pediatric Delirium followed international recommendations. The linguistic and semantic issues that emerged during the process were discussed by the expert panel, which unanimously agreed to slight modifications. During pretesting, the Cornell Assessment of Pediatric Delirium was administered to 30 eligible children, twice per day; the final version was easy to understand, could be completed quickly, and showed a high inter-rater correlation coefficient (0.955).
Conclusions:
The translation of the Cornell Assessment of Pediatric Delirium into Brazilian Portuguese and its cross-cultural adaptation were successful and preserved the linguistic and semantic properties of the original instrument. The Cornell Assessment of Pediatric Delirium proved to be easy to understand and could be completed quickly. Additional studies are needed to test the validity and psychometric properties of this version in Brazil.
Views0Abstract
Original ArticlesTranslation and cross-cultural adaptation of the Cornell Assessment of Pediatric Delirium scale for the Portuguese language
Rev Bras Ter Intensiva. 2018;30(2):195-200
DOI 10.5935/0103-507X.20180033
Views0See moreABSTRACT
Objective:
This study sought to translate the Cornell Assessment of Pediatric Delirium from English into Brazilian Portuguese and cross-culturally adapt it for use in Brazil.
Methods:
Following the authorization granted by its main author, the processes of translation and cross-cultural adaptation were performed with regard to the Cornell Assessment of Pediatric Delirium in accordance with the following internationally recommended steps: translation of the original into Portuguese by two native speakers of the target language; synthesis of the translated versions; back-translation by two native speakers of the original language; review and harmonization of the back-translation; a review of the Portuguese version of the Cornell Assessment of Pediatric Delirium by an expert panel composed of specialists; pretesting including assessments of clarity, comprehensibility, and acceptability of the translated version using a sample of the target population; and finishing modifications to achieve the final version.
Results:
The translation and cross-cultural adaptation of the Cornell Assessment of Pediatric Delirium followed international recommendations. The linguistic and semantic issues that emerged during the process were discussed by the expert panel, which unanimously agreed to slight modifications. During pretesting, the Cornell Assessment of Pediatric Delirium was administered to 30 eligible children, twice per day; the final version was easy to understand, could be completed quickly, and showed a high inter-rater correlation coefficient (0.955).
Conclusions:
The translation of the Cornell Assessment of Pediatric Delirium into Brazilian Portuguese and its cross-cultural adaptation were successful and preserved the linguistic and semantic properties of the original instrument. The Cornell Assessment of Pediatric Delirium proved to be easy to understand and could be completed quickly. Additional studies are needed to test the validity and psychometric properties of this version in Brazil.
-
Special Article
I Brazilian guidelines for respiratory physiotherapy in pediatric and neonatal intensive care units
Rev Bras Ter Intensiva. 2012;24(2):119-129
Abstract
Special ArticleI Brazilian guidelines for respiratory physiotherapy in pediatric and neonatal intensive care units
Rev Bras Ter Intensiva. 2012;24(2):119-129
DOI 10.1590/S0103-507X2012000200005
Views0Developing guidelines for the role of the physiotherapist in neonatal and pediatric intensive care units is essential because these professionals are responsible for the rehabilitation of critically ill patients. Rehabilitation includes the evaluation and prevention of functional kinetic alterations, application of treatment interventions (respiratory and/or motor physiotherapy), control and application of medical gases, care of mechanical ventilation, weaning and extubation, tracheal gas insufflation, inflation/deflation of the endotracheal cuff protocol, and surfactant application, aiming to allow patients to have a full recovery and return to their functional activities. In this article, we present guidelines that are intended to guide the physiotherapist in some of the prevention/treatment interventions in respiratory therapy (airway clearance, lung expansion, position in bed, airway suction, drug inhalation, and cough assist), which help in the rehabilitation process of newborns and children in intensive care units during mechanical ventilation and up to 12 hours following extubation.
Keywords:ChildIntensive care, neonatalPhysical therapy modalitiesRehabilitationRespiration, artificialRespiratory therapySee moreViews0Abstract
Special ArticleI Brazilian guidelines for respiratory physiotherapy in pediatric and neonatal intensive care units
Rev Bras Ter Intensiva. 2012;24(2):119-129
DOI 10.1590/S0103-507X2012000200005
Views0Developing guidelines for the role of the physiotherapist in neonatal and pediatric intensive care units is essential because these professionals are responsible for the rehabilitation of critically ill patients. Rehabilitation includes the evaluation and prevention of functional kinetic alterations, application of treatment interventions (respiratory and/or motor physiotherapy), control and application of medical gases, care of mechanical ventilation, weaning and extubation, tracheal gas insufflation, inflation/deflation of the endotracheal cuff protocol, and surfactant application, aiming to allow patients to have a full recovery and return to their functional activities. In this article, we present guidelines that are intended to guide the physiotherapist in some of the prevention/treatment interventions in respiratory therapy (airway clearance, lung expansion, position in bed, airway suction, drug inhalation, and cough assist), which help in the rehabilitation process of newborns and children in intensive care units during mechanical ventilation and up to 12 hours following extubation.
Keywords:ChildIntensive care, neonatalPhysical therapy modalitiesRehabilitationRespiration, artificialRespiratory therapySee more
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis