
You searched for:"Cassiano Teixeira"
We found (44) results for your search.-
Original Article
The 6-Minute Walk Test predicts long-term physical improvement among intensive care unit survivors: a prospective cohort study
- Regis Goulart Rosa
 ,
, - Camila Dietrich,
- Enio Luiz Tschiedel do Valle,
- Denise Souza,
- Luciana Tagliari, [ … ],
- Cassiano Teixeira
Abstract
Original ArticleThe 6-Minute Walk Test predicts long-term physical improvement among intensive care unit survivors: a prospective cohort study
Rev Bras Ter Intensiva. 2021;33(3):374-383
DOI 10.5935/0103-507X.20210056
- Regis Goulart Rosa ,
- Camila Dietrich,
- Enio Luiz Tschiedel do Valle,
- Denise Souza,
- Luciana Tagliari,
- Mariana Mattioni,
- Túlio Frederico Tonietto,
- Rosa da Rosa,
- Mirceli Goulart Barbosa,
- Gisele Agustini Lovatel,
- Pedro Dal Lago,
- Eubrando Silvestre Oliveira,
- Daniel Sganzerla,
- Juliana M. S. Andrade ,
- Paula Berto,
- Paulo Ricardo Cardoso,
- Evelin Carneiro Sanchez,
- Maicon Falavigna ,
- Juçara G. Maccari,
- Gabriela Rech,
- Caroline Robinson,
- Daniel Schneider,
- Patrícia de Leon,
- Lívia Biason,
- Cassiano Teixeira
Views1See moreABSTRACT
Objective:
To evaluate the ability of the 6-Minute Walk Test to predict long-term physical functional status improvement among intensive care unit survivors.
Methods:
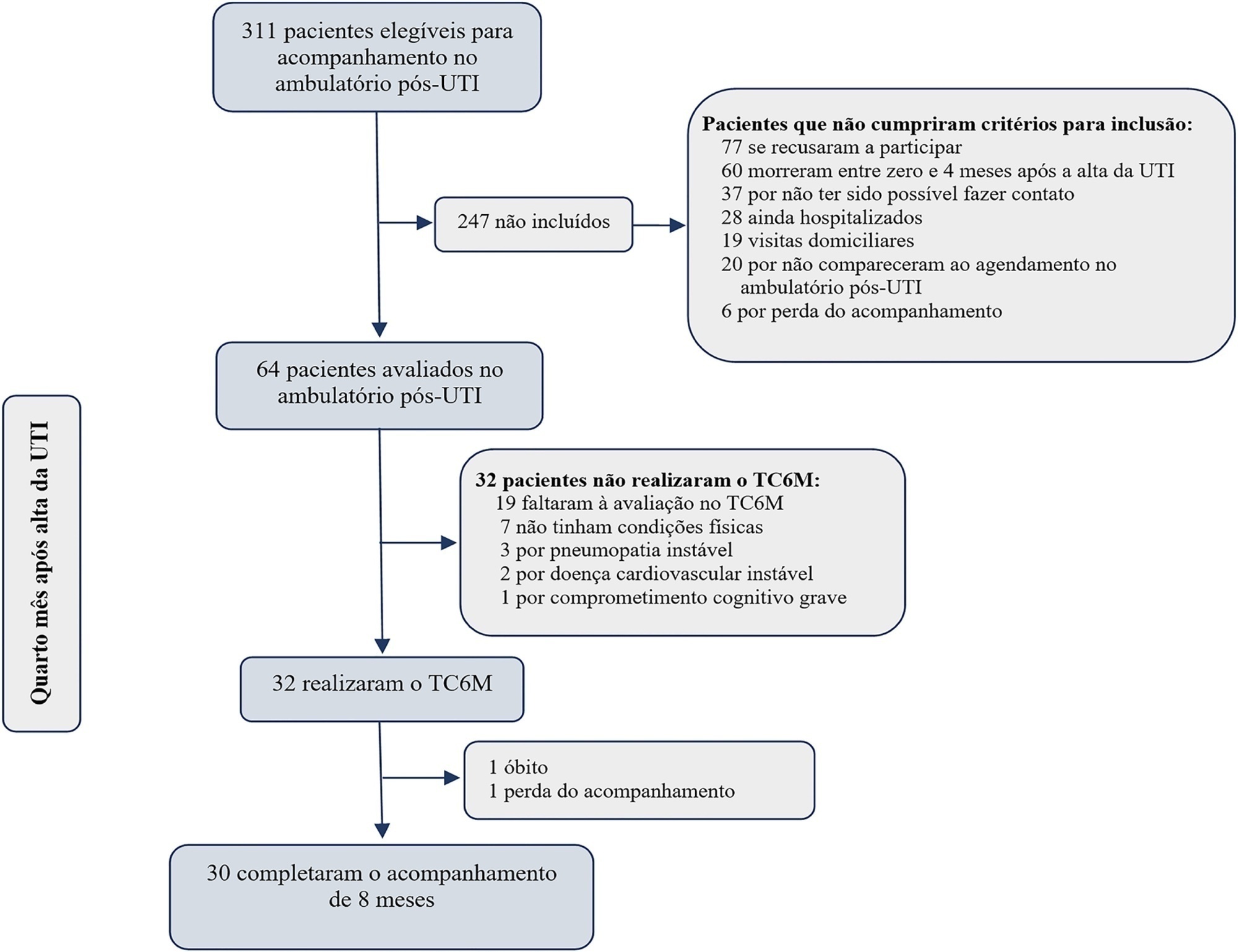
Thirty-two intensive care unit survivors were prospectively evaluated from February 2017 to August 2018 in a post-intensive care unit outpatient clinic in Brazil. Individuals with intensive care unit stays > 72 hours (emergency admissions) or > 120 hours (elective admissions) attending the post-intensive care unit clinic four months after intensive care unit discharge were consecutively enrolled. The association between the 6-Minute Walk Test distance at baseline and physical functional status was assessed over 8 months using the Barthel Index.
Results:
The mean 6-Minute Walk Test distance was significantly lower in intensive care unit survivors than in the general population (405m versus 557m; p < 0.001). Age (β = -4.0; p < 0.001) and muscle weakness (β = -99.7; p = 0.02) were associated with the 6-Minute Walk Test distance. A 6-Minute Walk Test distance was associated with improvement in physical functional status over the 8-month follow-up (odds ratio for each 10m of 1.07; 95%CI 1.01 - 1.16; p = 0.03). The area under the Receiver Operating Characteristic curve for the 6-Minute Walk Test prediction of physical functional status improvement was 0.72 (95%CI 0.53 - 0.88).
Conclusion:
The 6-Minute Walk Test performed 4 months after intensive care unit discharge predicted long-term physical functional status among intensive care unit survivors with moderate accuracy.
Views1

Abstract
Original ArticleThe 6-Minute Walk Test predicts long-term physical improvement among intensive care unit survivors: a prospective cohort study
Rev Bras Ter Intensiva. 2021;33(3):374-383
DOI 10.5935/0103-507X.20210056
- Regis Goulart Rosa ,
- Camila Dietrich,
- Enio Luiz Tschiedel do Valle,
- Denise Souza,
- Luciana Tagliari,
- Mariana Mattioni,
- Túlio Frederico Tonietto,
- Rosa da Rosa,
- Mirceli Goulart Barbosa,
- Gisele Agustini Lovatel,
- Pedro Dal Lago,
- Eubrando Silvestre Oliveira,
- Daniel Sganzerla,
- Juliana M. S. Andrade ,
- Paula Berto,
- Paulo Ricardo Cardoso,
- Evelin Carneiro Sanchez,
- Maicon Falavigna ,
- Juçara G. Maccari,
- Gabriela Rech,
- Caroline Robinson,
- Daniel Schneider,
- Patrícia de Leon,
- Lívia Biason,
- Cassiano Teixeira
Views1See moreABSTRACT
Objective:
To evaluate the ability of the 6-Minute Walk Test to predict long-term physical functional status improvement among intensive care unit survivors.
Methods:
Thirty-two intensive care unit survivors were prospectively evaluated from February 2017 to August 2018 in a post-intensive care unit outpatient clinic in Brazil. Individuals with intensive care unit stays > 72 hours (emergency admissions) or > 120 hours (elective admissions) attending the post-intensive care unit clinic four months after intensive care unit discharge were consecutively enrolled. The association between the 6-Minute Walk Test distance at baseline and physical functional status was assessed over 8 months using the Barthel Index.
Results:
The mean 6-Minute Walk Test distance was significantly lower in intensive care unit survivors than in the general population (405m versus 557m; p < 0.001). Age (β = -4.0; p < 0.001) and muscle weakness (β = -99.7; p = 0.02) were associated with the 6-Minute Walk Test distance. A 6-Minute Walk Test distance was associated with improvement in physical functional status over the 8-month follow-up (odds ratio for each 10m of 1.07; 95%CI 1.01 - 1.16; p = 0.03). The area under the Receiver Operating Characteristic curve for the 6-Minute Walk Test prediction of physical functional status improvement was 0.72 (95%CI 0.53 - 0.88).
Conclusion:
The 6-Minute Walk Test performed 4 months after intensive care unit discharge predicted long-term physical functional status among intensive care unit survivors with moderate accuracy.
- Regis Goulart Rosa
-
Review Article
What outcomes should be evaluated in critically ill patients?
Rev Bras Ter Intensiva. 2021;33(2):312-319
Abstract
Review ArticleWhat outcomes should be evaluated in critically ill patients?
Rev Bras Ter Intensiva. 2021;33(2):312-319
DOI 10.5935/0103-507X.20210040
Views2See moreABSTRACT
Randomized clinical trials in intensive care prioritize disease-focused outcomes rather than patient-centered outcomes. A paradigm shift considering the evaluation of measures after hospital discharge and measures focused on quality of life and common symptoms, such as pain and dyspnea, could better reflect the wishes of patients and their families. However, barriers related to the systematization of the interpretation of these outcomes, the heterogeneity of measurement instruments and the greater difficulty in performing the studies, to date, seem to hinder this change. In addition, the joint participation of patients, families, researchers, and clinicians in the definition of study outcomes is not yet a reality.
Views2Abstract
Review ArticleWhat outcomes should be evaluated in critically ill patients?
Rev Bras Ter Intensiva. 2021;33(2):312-319
DOI 10.5935/0103-507X.20210040
Views2See moreABSTRACT
Randomized clinical trials in intensive care prioritize disease-focused outcomes rather than patient-centered outcomes. A paradigm shift considering the evaluation of measures after hospital discharge and measures focused on quality of life and common symptoms, such as pain and dyspnea, could better reflect the wishes of patients and their families. However, barriers related to the systematization of the interpretation of these outcomes, the heterogeneity of measurement instruments and the greater difficulty in performing the studies, to date, seem to hinder this change. In addition, the joint participation of patients, families, researchers, and clinicians in the definition of study outcomes is not yet a reality.
-
Letter to the Editor
Is there room for children to visit adult intensive care units?
Rev Bras Ter Intensiva. 2021;33(1):176-178
Abstract
Letter to the EditorIs there room for children to visit adult intensive care units?
Rev Bras Ter Intensiva. 2021;33(1):176-178
DOI 10.5935/0103-507X.20210020
Views0TO THE EDITOR “ My husband has been in the ICU for more than 60 days and I fear that the time for his departure is coming. I was informed of the rule that the visit is allowed from 12 years old, but our daughter is 11. She will be 12 in 2 weeks, but […]See moreViews0Abstract
Letter to the EditorIs there room for children to visit adult intensive care units?
Rev Bras Ter Intensiva. 2021;33(1):176-178
DOI 10.5935/0103-507X.20210020
Views0TO THE EDITOR “ My husband has been in the ICU for more than 60 days and I fear that the time for his departure is coming. I was informed of the rule that the visit is allowed from 12 years old, but our daughter is 11. She will be 12 in 2 weeks, but […]See more
-
Original Article
Changes in cardiac arrest profiles after the implementation of a Rapid Response Team
- Marina Verçoza Viana ,
- Diego Silva Leite Nunes,
- Cassiano Teixeira ,
- Silvia Regina Rios Vieira,
- Grazziela Torres, [ … ],
- Marcio Manozzo Boniatti
Abstract
Original ArticleChanges in cardiac arrest profiles after the implementation of a Rapid Response Team
Rev Bras Ter Intensiva. 2021;33(1):96-101
DOI 10.5935/0103-507X.20210010
- Marina Verçoza Viana ,
- Diego Silva Leite Nunes,
- Cassiano Teixeira ,
- Silvia Regina Rios Vieira,
- Grazziela Torres,
- Janete Salles Brauner,
- Helena Müller,
- Thais Crivellaro Dutra Butelli,
- Marcio Manozzo Boniatti
Views1See moreABSTRACT
Objective:
To evaluate changes in the characteristics of in-hospital cardiac arrest after the implementation of a Rapid Response Team.
Methods:
This was a prospective observational study of in-hospital cardiac arrest that occurred from January 2013 to December 2017. The exclusion criterion was in-hospital cardiac arrest in the intensive care unit, emergency room or operating room. The Rapid Response Team was implemented in July 2014 in the study hospital. Patients were classified into two groups: a Pre-Rapid Response Team (in-hospital cardiac arrest before Rapid Response Team implementation) and a Post-Rapid Response Team (in-hospital cardiac arrest after Rapid Response Team implementation). Patients were followed until hospital discharge or death.
Results:
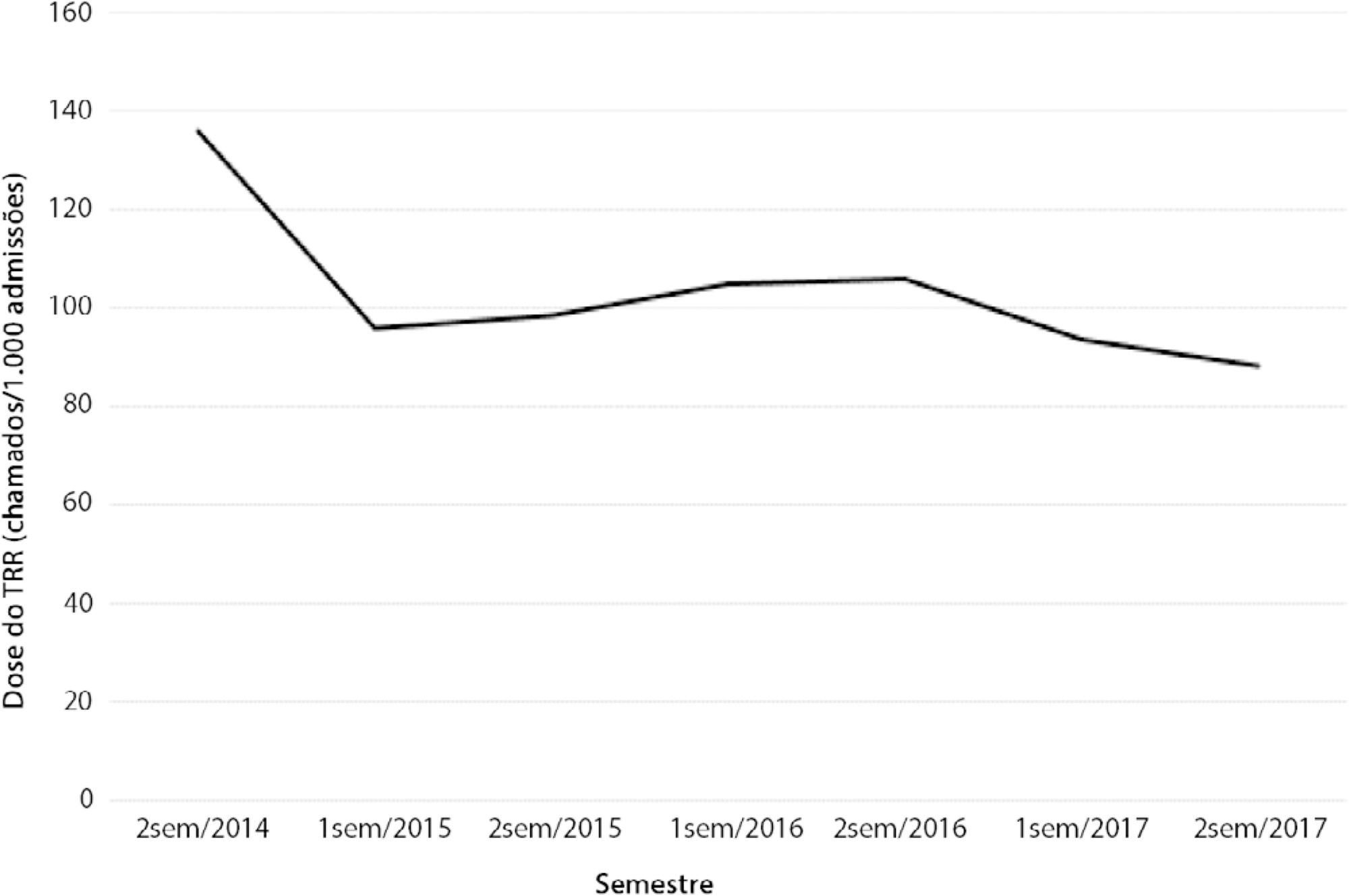
We had a total of 308 cardiac arrests (64.6 ± 15.2 years, 60.3% men, 13.9% with initial shockable rhythm). There was a decrease from 4.2 to 2.5 in-hospital cardiac arrest/1000 admissions after implementation of the Rapid Response Team, and we had approximately 124 calls/1000 admissions. Pre-Rapid Response Team cardiac arrest was associated with more hypoxia (29.4 versus 14.3%; p = 0.006) and an altered respiratory rate (14.7 versus 4.2%; p = 0.004) compared with post-Rapid Response Team cardiac arrest. Cardiac arrest due to hypoxia was more common before Rapid Response Team implementation (61.2 versus 38.1%, p < 0.001). In multivariate analysis, return of spontaneous circulation was associated with shockable rhythm (OR 2.97; IC95% 1.04 - 8.43) and witnessed cardiac arrest (OR 2.52; IC95% 1.39 - 4.59) but not with Rapid Response Team implementation (OR 1.40; IC95% 0.70 - 2.81) or premonitory signs (OR 0.71; IC95% 0.39 - 1.28). In multivariate analysis, in-hospital mortality was associated with non-shockable rhythm (OR 5.34; IC95% 2.28 - 12.53) and age (OR 1.03; IC95% 1.01 - 1.05) but not with Rapid Response Team implementation (OR 0.89; IC95% 0.40 - 2.02).
Conclusion:
Even though Rapid Response Team implementation is associated with a reduction in in-hospital cardiac arrest, it was not associated with the mortality of in-hospital cardiac arrest victims. A significant decrease in cardiac arrests due to respiratory causes was noted after Rapid Response Team implementation.
Views1Abstract
Original ArticleChanges in cardiac arrest profiles after the implementation of a Rapid Response Team
Rev Bras Ter Intensiva. 2021;33(1):96-101
DOI 10.5935/0103-507X.20210010
- Marina Verçoza Viana ,
- Diego Silva Leite Nunes,
- Cassiano Teixeira ,
- Silvia Regina Rios Vieira,
- Grazziela Torres,
- Janete Salles Brauner,
- Helena Müller,
- Thais Crivellaro Dutra Butelli,
- Marcio Manozzo Boniatti
Views1See moreABSTRACT
Objective:
To evaluate changes in the characteristics of in-hospital cardiac arrest after the implementation of a Rapid Response Team.
Methods:
This was a prospective observational study of in-hospital cardiac arrest that occurred from January 2013 to December 2017. The exclusion criterion was in-hospital cardiac arrest in the intensive care unit, emergency room or operating room. The Rapid Response Team was implemented in July 2014 in the study hospital. Patients were classified into two groups: a Pre-Rapid Response Team (in-hospital cardiac arrest before Rapid Response Team implementation) and a Post-Rapid Response Team (in-hospital cardiac arrest after Rapid Response Team implementation). Patients were followed until hospital discharge or death.
Results:
We had a total of 308 cardiac arrests (64.6 ± 15.2 years, 60.3% men, 13.9% with initial shockable rhythm). There was a decrease from 4.2 to 2.5 in-hospital cardiac arrest/1000 admissions after implementation of the Rapid Response Team, and we had approximately 124 calls/1000 admissions. Pre-Rapid Response Team cardiac arrest was associated with more hypoxia (29.4 versus 14.3%; p = 0.006) and an altered respiratory rate (14.7 versus 4.2%; p = 0.004) compared with post-Rapid Response Team cardiac arrest. Cardiac arrest due to hypoxia was more common before Rapid Response Team implementation (61.2 versus 38.1%, p < 0.001). In multivariate analysis, return of spontaneous circulation was associated with shockable rhythm (OR 2.97; IC95% 1.04 - 8.43) and witnessed cardiac arrest (OR 2.52; IC95% 1.39 - 4.59) but not with Rapid Response Team implementation (OR 1.40; IC95% 0.70 - 2.81) or premonitory signs (OR 0.71; IC95% 0.39 - 1.28). In multivariate analysis, in-hospital mortality was associated with non-shockable rhythm (OR 5.34; IC95% 2.28 - 12.53) and age (OR 1.03; IC95% 1.01 - 1.05) but not with Rapid Response Team implementation (OR 0.89; IC95% 0.40 - 2.02).
Conclusion:
Even though Rapid Response Team implementation is associated with a reduction in in-hospital cardiac arrest, it was not associated with the mortality of in-hospital cardiac arrest victims. A significant decrease in cardiac arrests due to respiratory causes was noted after Rapid Response Team implementation.
- Marina Verçoza Viana
-
Special Article
Brazilian guidelines for the management of brain-dead potential organ donors. The task force of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Transplantes de Órgãos, Brazilian Research in Critical Care Network, and the General Coordination of the National Transplant System
- Glauco Adrieno Westphal ,
- Caroline Cabral Robinson,
- Alexandre Biasi Cavalcanti ,
- Anderson Ricardo Roman Gonçalves,
- Cátia Moreira Guterres, [ … ],
- Maicon Falavigna
Abstract
Special ArticleBrazilian guidelines for the management of brain-dead potential organ donors. The task force of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Transplantes de Órgãos, Brazilian Research in Critical Care Network, and the General Coordination of the National Transplant System
Rev Bras Ter Intensiva. 2021;33(1):1-11
DOI 10.5935/0103-507X.20210001
- Glauco Adrieno Westphal ,
- Caroline Cabral Robinson,
- Alexandre Biasi Cavalcanti ,
- Anderson Ricardo Roman Gonçalves,
- Cátia Moreira Guterres,
- Cassiano Teixeira ,
- Cinara Stein,
- Cristiano Augusto Franke,
- Daiana Barbosa da Silva,
- Daniela Ferreira Salomão Pontes,
- Diego Silva Leite Nunes,
- Edson Abdala,
- Felipe Dal-Pizzol ,
- Fernando Augusto Bozza ,
- Flávia Ribeiro Machado,
- Joel de Andrade,
- Luciane Nascimento Cruz,
- Luciano César Pontes Azevedo,
- Miriam Cristine Vahl Machado,
- Regis Goulart Rosa ,
- Roberto Ceratti Manfro,
- Rosana Reis Nothen,
- Suzana Margareth Lobo,
- Tatiana Helena Rech ,
- Thiago Costa Lisboa,
- Verônica Colpani,
- Maicon Falavigna
Views5See moreAbstract
Objective:
To contribute to updating the recommendations for brain-dead potential organ donor management.
Methods:
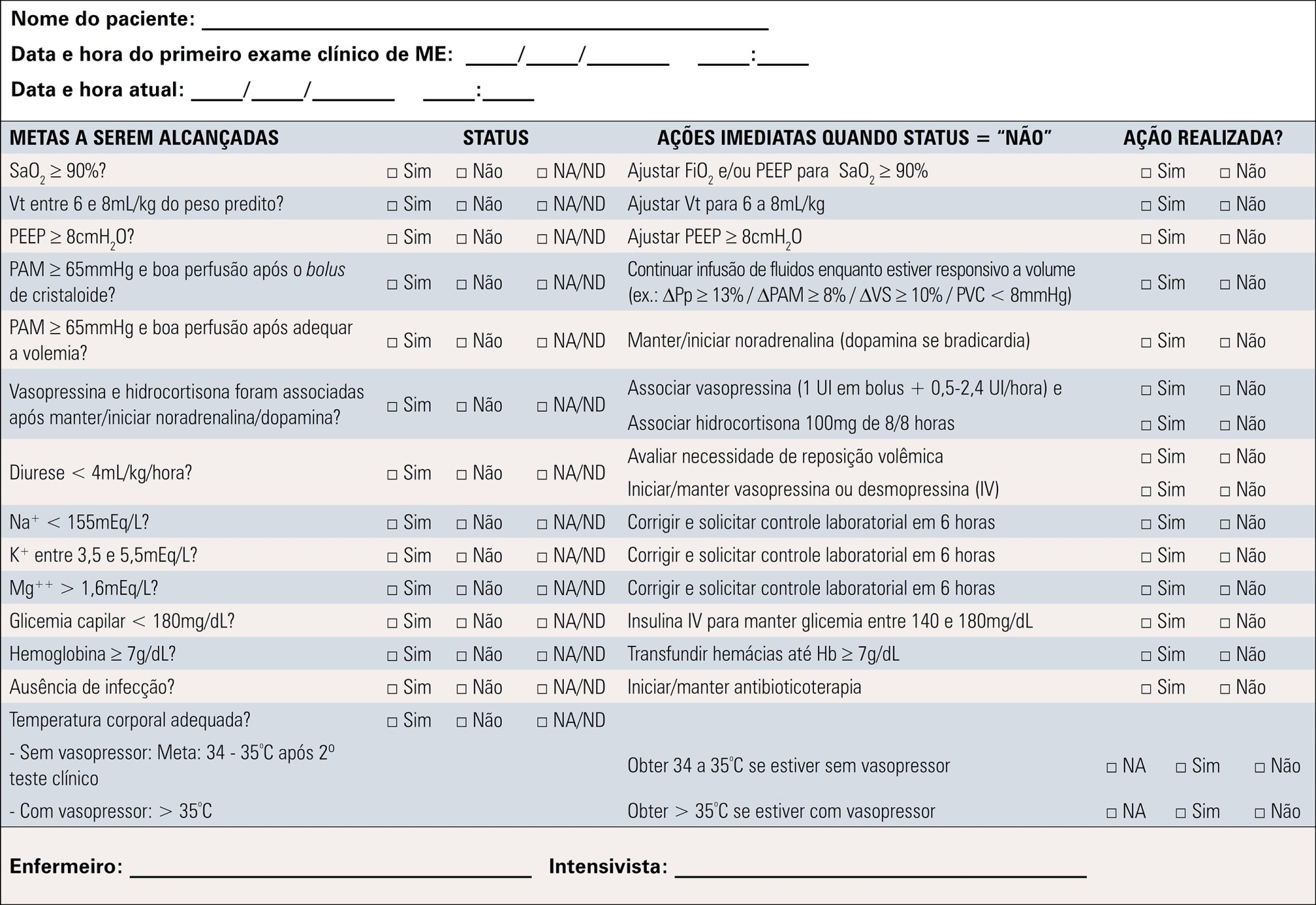
A group of 27 experts, including intensivists, transplant coordinators, transplant surgeons, and epidemiologists, answered questions related to the following topics were divided into mechanical ventilation, hemodynamics, endocrine-metabolic management, infection, body temperature, blood transfusion, and checklists use. The outcomes considered were cardiac arrests, number of organs removed or transplanted as well as function / survival of transplanted organs. The quality of evidence of the recommendations was assessed using the Grading of Recommendations Assessment, Development, and Evaluation system to classify the recommendations.
Results:
A total of 19 recommendations were drawn from the expert panel. Of these, 7 were classified as strong, 11 as weak and 1 was considered a good clinical practice.
Conclusion:
Despite the agreement among panel members on most recommendations, the grade of recommendation was mostly weak.
Views5Abstract
Special ArticleBrazilian guidelines for the management of brain-dead potential organ donors. The task force of the Associação de Medicina Intensiva Brasileira, Associação Brasileira de Transplantes de Órgãos, Brazilian Research in Critical Care Network, and the General Coordination of the National Transplant System
Rev Bras Ter Intensiva. 2021;33(1):1-11
DOI 10.5935/0103-507X.20210001
- Glauco Adrieno Westphal ,
- Caroline Cabral Robinson,
- Alexandre Biasi Cavalcanti ,
- Anderson Ricardo Roman Gonçalves,
- Cátia Moreira Guterres,
- Cassiano Teixeira ,
- Cinara Stein,
- Cristiano Augusto Franke,
- Daiana Barbosa da Silva,
- Daniela Ferreira Salomão Pontes,
- Diego Silva Leite Nunes,
- Edson Abdala,
- Felipe Dal-Pizzol ,
- Fernando Augusto Bozza ,
- Flávia Ribeiro Machado,
- Joel de Andrade,
- Luciane Nascimento Cruz,
- Luciano César Pontes Azevedo,
- Miriam Cristine Vahl Machado,
- Regis Goulart Rosa ,
- Roberto Ceratti Manfro,
- Rosana Reis Nothen,
- Suzana Margareth Lobo,
- Tatiana Helena Rech ,
- Thiago Costa Lisboa,
- Verônica Colpani,
- Maicon Falavigna
Views5See moreAbstract
Objective:
To contribute to updating the recommendations for brain-dead potential organ donor management.
Methods:
A group of 27 experts, including intensivists, transplant coordinators, transplant surgeons, and epidemiologists, answered questions related to the following topics were divided into mechanical ventilation, hemodynamics, endocrine-metabolic management, infection, body temperature, blood transfusion, and checklists use. The outcomes considered were cardiac arrests, number of organs removed or transplanted as well as function / survival of transplanted organs. The quality of evidence of the recommendations was assessed using the Grading of Recommendations Assessment, Development, and Evaluation system to classify the recommendations.
Results:
A total of 19 recommendations were drawn from the expert panel. Of these, 7 were classified as strong, 11 as weak and 1 was considered a good clinical practice.
Conclusion:
Despite the agreement among panel members on most recommendations, the grade of recommendation was mostly weak.
- Glauco Adrieno Westphal
-
Special Article
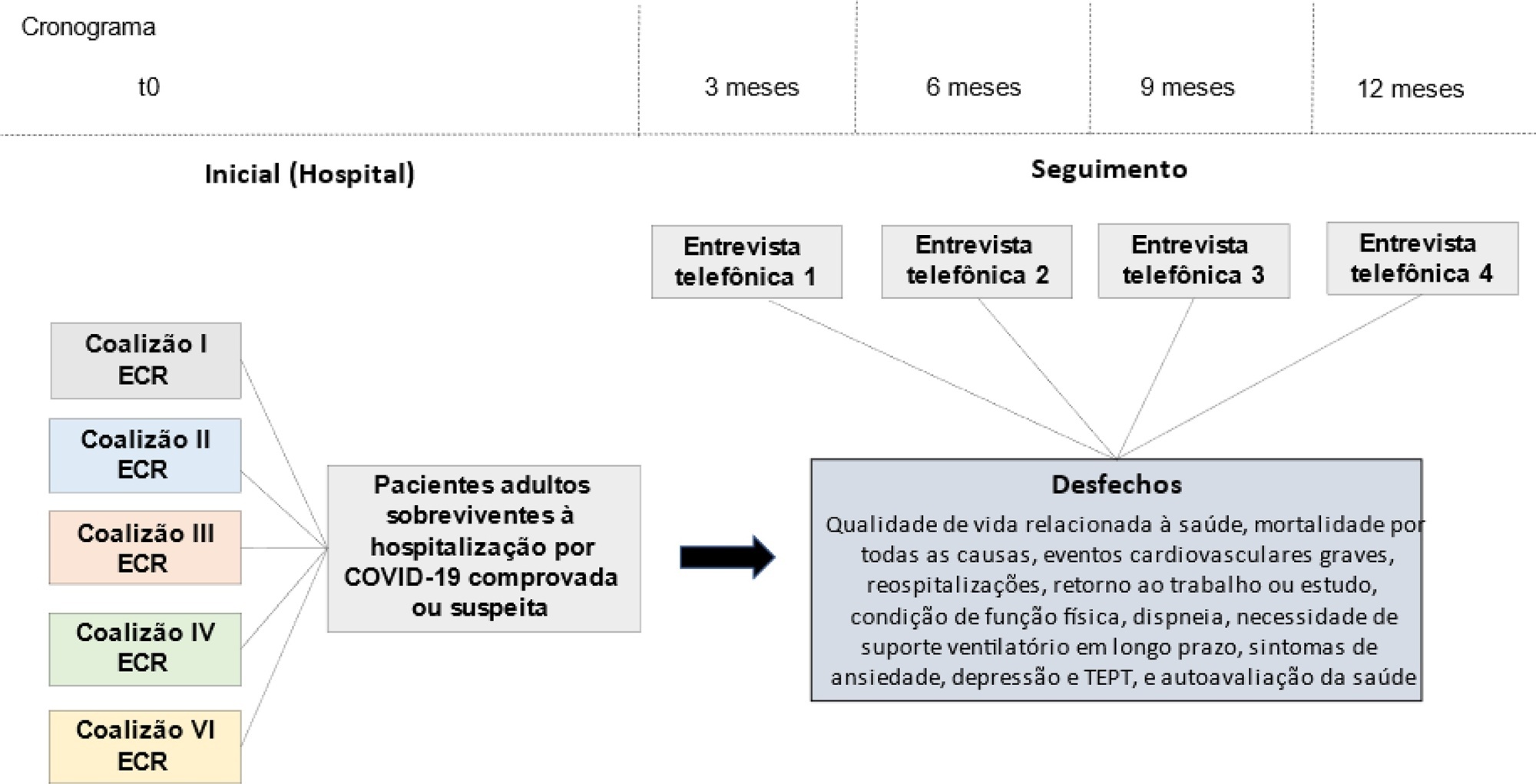
Quality of life and long-term outcomes after hospitalization for COVID-19: Protocol for a prospective cohort study (Coalition VII)
- Regis Goulart Rosa ,
- Caroline Cabral Robinson,
- Viviane Cordeiro Veiga ,
- Alexandre Biasi Cavalcanti ,
- Luciano César Pontes de Azevedo, [ … ],
- Maicon Falavigna
Abstract
Special ArticleQuality of life and long-term outcomes after hospitalization for COVID-19: Protocol for a prospective cohort study (Coalition VII)
Rev Bras Ter Intensiva. 2021;33(1):31-37
DOI 10.5935/0103-507X.20210003
- Regis Goulart Rosa ,
- Caroline Cabral Robinson,
- Viviane Cordeiro Veiga ,
- Alexandre Biasi Cavalcanti ,
- Luciano César Pontes de Azevedo,
- Flávia Ribeiro Machado,
- Otavio Berwanger,
- Álvaro Avezum,
- Renato Delascio Lopes,
- Thiago Costa Lisboa,
- Cassiano Teixeira ,
- Fernando Godinho Zampieri ,
- Bruno Martins Tomazini,
- Letícia Kawano-Dourado,
- Daniel Schneider,
- Denise de Souza,
- Rosa da Rosa Minho dos Santos,
- Sabrina Souza da Silva,
- Geraldine Trott,
- Bruna dos Passos Gimenes,
- Ana Paula de Souza,
- Bruna Machado Barroso,
- Lauren Sezerá Costa,
- Liége Gregoletto Brognoli,
- Melissa Pezzetti Pelliccioli,
- Nicole dos Santos Studier,
- Raíne Fogliati de Carli Schardosim,
- Tainá Aparecida Haubert,
- Victoria Emanuele Lobo Pallaoro,
- Debora Mariani de Oliveira,
- Pedro Isaacsson Velho,
- Gregory Saraiva Medeiros,
- Marcelo Basso Gazzana,
- Alexandre Prehn Zavascki,
- Paulo Márcio Pitrez,
- Roselaine Pinheiro de Oliveira,
- Carisi Anne Polanczyk,
- Luiz Antônio Nasi,
- Luciano Serpa Hammes,
- Maicon Falavigna
Views0See moreAbstract
Introduction:
The long-term effects caused by COVID-19 are unknown. The present study aims to assess factors associated with health-related quality of life and long-term outcomes among survivors of hospitalization for COVID-19 in Brazil.
Methods:
This is a multicenter prospective cohort study nested in five randomized clinical trials designed to assess the effects of specific COVID-19 treatments in over 50 centers in Brazil. Adult survivors of hospitalization due to proven or suspected SARS-CoV-2 infection will be followed-up for a period of 1 year by means of structured telephone interviews. The primary outcome is the 1-year utility score of health-related quality of life assessed by the EuroQol-5D3L. Secondary outcomes include all-cause mortality, major cardiovascular events, rehospitalizations, return to work or study, physical functional status assessed by the Lawton-Brody Instrumental Activities of Daily Living, dyspnea assessed by the modified Medical Research Council dyspnea scale, need for long-term ventilatory support, symptoms of anxiety and depression assessed by the Hospital Anxiety and Depression Scale, symptoms of posttraumatic stress disorder assessed by the Impact of Event Scale-Revised, and self-rated health assessed by the EuroQol-5D3L Visual Analog Scale. Generalized estimated equations will be performed to test the association between five sets of variables (1- demographic characteristics, 2- premorbid state of health, 3- characteristics of acute illness, 4- specific COVID-19 treatments received, and 5- time-updated postdischarge variables) and outcomes.
Ethics and dissemination:
The study protocol was approved by the Research Ethics Committee of all participant institutions. The results will be disseminated through conferences and peer-reviewed journals.
Views0Abstract
Special ArticleQuality of life and long-term outcomes after hospitalization for COVID-19: Protocol for a prospective cohort study (Coalition VII)
Rev Bras Ter Intensiva. 2021;33(1):31-37
DOI 10.5935/0103-507X.20210003
- Regis Goulart Rosa ,
- Caroline Cabral Robinson,
- Viviane Cordeiro Veiga ,
- Alexandre Biasi Cavalcanti ,
- Luciano César Pontes de Azevedo,
- Flávia Ribeiro Machado,
- Otavio Berwanger,
- Álvaro Avezum,
- Renato Delascio Lopes,
- Thiago Costa Lisboa,
- Cassiano Teixeira ,
- Fernando Godinho Zampieri ,
- Bruno Martins Tomazini,
- Letícia Kawano-Dourado,
- Daniel Schneider,
- Denise de Souza,
- Rosa da Rosa Minho dos Santos,
- Sabrina Souza da Silva,
- Geraldine Trott,
- Bruna dos Passos Gimenes,
- Ana Paula de Souza,
- Bruna Machado Barroso,
- Lauren Sezerá Costa,
- Liége Gregoletto Brognoli,
- Melissa Pezzetti Pelliccioli,
- Nicole dos Santos Studier,
- Raíne Fogliati de Carli Schardosim,
- Tainá Aparecida Haubert,
- Victoria Emanuele Lobo Pallaoro,
- Debora Mariani de Oliveira,
- Pedro Isaacsson Velho,
- Gregory Saraiva Medeiros,
- Marcelo Basso Gazzana,
- Alexandre Prehn Zavascki,
- Paulo Márcio Pitrez,
- Roselaine Pinheiro de Oliveira,
- Carisi Anne Polanczyk,
- Luiz Antônio Nasi,
- Luciano Serpa Hammes,
- Maicon Falavigna
Views0See moreAbstract
Introduction:
The long-term effects caused by COVID-19 are unknown. The present study aims to assess factors associated with health-related quality of life and long-term outcomes among survivors of hospitalization for COVID-19 in Brazil.
Methods:
This is a multicenter prospective cohort study nested in five randomized clinical trials designed to assess the effects of specific COVID-19 treatments in over 50 centers in Brazil. Adult survivors of hospitalization due to proven or suspected SARS-CoV-2 infection will be followed-up for a period of 1 year by means of structured telephone interviews. The primary outcome is the 1-year utility score of health-related quality of life assessed by the EuroQol-5D3L. Secondary outcomes include all-cause mortality, major cardiovascular events, rehospitalizations, return to work or study, physical functional status assessed by the Lawton-Brody Instrumental Activities of Daily Living, dyspnea assessed by the modified Medical Research Council dyspnea scale, need for long-term ventilatory support, symptoms of anxiety and depression assessed by the Hospital Anxiety and Depression Scale, symptoms of posttraumatic stress disorder assessed by the Impact of Event Scale-Revised, and self-rated health assessed by the EuroQol-5D3L Visual Analog Scale. Generalized estimated equations will be performed to test the association between five sets of variables (1- demographic characteristics, 2- premorbid state of health, 3- characteristics of acute illness, 4- specific COVID-19 treatments received, and 5- time-updated postdischarge variables) and outcomes.
Ethics and dissemination:
The study protocol was approved by the Research Ethics Committee of all participant institutions. The results will be disseminated through conferences and peer-reviewed journals.
- Regis Goulart Rosa
-
Review Article
The medical decision-making process in the time of the coronavirus pandemic
- Cassiano Teixeira ,
- Regis Goulart Rosa ,
- Edison Moraes Rodrigues Filho,
- Eduardo de Oliveira Fernandes
Abstract
Review ArticleThe medical decision-making process in the time of the coronavirus pandemic
Rev Bras Ter Intensiva. 2020;32(2):308-311
DOI 10.5935/0103-507X.20200033
- Cassiano Teixeira ,
- Regis Goulart Rosa ,
- Edison Moraes Rodrigues Filho,
- Eduardo de Oliveira Fernandes
Views0ABSTRACT
The disease pandemic caused by the novel coronavirus has triggered significant changes in the medical decision-making process relating to critically ill patients. Admissions to intensive care units have suddenly increased, but many of these patients do not present with clinical manifestations related to the viral infection but rather exacerbation of preexisting diseases. In this context, we must prevent intuitive decision-making and insecurity from leading us to exhaust the available critical-care beds before they are truly necessary, while still recognizing the importance of rapid decision-making in emergency situations. One of the best ways to achieve this goal may be by practicing metacognition and establishing ways for regular feedback to be provided to professionals engaged in inherently rapid decision-making processes.
Keywords:BetacoronavirusCatastrophic illnessClinical decision-makingCoronavirusCoronavirus infectiousFeedbackIntensive care unitsMetacognitionPandemicsSee moreViews0Abstract
Review ArticleThe medical decision-making process in the time of the coronavirus pandemic
Rev Bras Ter Intensiva. 2020;32(2):308-311
DOI 10.5935/0103-507X.20200033
- Cassiano Teixeira ,
- Regis Goulart Rosa ,
- Edison Moraes Rodrigues Filho,
- Eduardo de Oliveira Fernandes
Views0ABSTRACT
The disease pandemic caused by the novel coronavirus has triggered significant changes in the medical decision-making process relating to critically ill patients. Admissions to intensive care units have suddenly increased, but many of these patients do not present with clinical manifestations related to the viral infection but rather exacerbation of preexisting diseases. In this context, we must prevent intuitive decision-making and insecurity from leading us to exhaust the available critical-care beds before they are truly necessary, while still recognizing the importance of rapid decision-making in emergency situations. One of the best ways to achieve this goal may be by practicing metacognition and establishing ways for regular feedback to be provided to professionals engaged in inherently rapid decision-making processes.
Keywords:BetacoronavirusCatastrophic illnessClinical decision-makingCoronavirusCoronavirus infectiousFeedbackIntensive care unitsMetacognitionPandemicsSee more - Cassiano Teixeira
-
Review Articles
Acute respiratory distress syndrome: how do patients fare after the intensive care unit?
Rev Bras Ter Intensiva. 2019;31(4):555-560
Abstract
Review ArticlesAcute respiratory distress syndrome: how do patients fare after the intensive care unit?
Rev Bras Ter Intensiva. 2019;31(4):555-560
DOI 10.5935/0103-507X.20190074
Views0See moreABSTRACT
Patients with acute respiratory distress syndrome require ventilation strategies that have been shown to be important for reducing short-term mortality, such as protective ventilation and prone position ventilation. However, patients who survive have a prolonged stay in both the intensive care unit and the hospital, and they experience a reduction in overall satisfaction with life (independence, acceptance and positive outlook) as well as decreased mental health (including anxiety, depression and posttraumatic stress disorder symptoms), physical health (impaired physical state and activities of daily living; fatigue and muscle weakness), social health and the ability to participate in social activities (including relationships with friends and family, hobbies and social gatherings).
Views0Abstract
Review ArticlesAcute respiratory distress syndrome: how do patients fare after the intensive care unit?
Rev Bras Ter Intensiva. 2019;31(4):555-560
DOI 10.5935/0103-507X.20190074
Views0See moreABSTRACT
Patients with acute respiratory distress syndrome require ventilation strategies that have been shown to be important for reducing short-term mortality, such as protective ventilation and prone position ventilation. However, patients who survive have a prolonged stay in both the intensive care unit and the hospital, and they experience a reduction in overall satisfaction with life (independence, acceptance and positive outlook) as well as decreased mental health (including anxiety, depression and posttraumatic stress disorder symptoms), physical health (impaired physical state and activities of daily living; fatigue and muscle weakness), social health and the ability to participate in social activities (including relationships with friends and family, hobbies and social gatherings).
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis