Respiratory rate Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2024;36:e20240203en
DOI 10.62675/2965-2774.20240203-en
To assess whether the respiratory oxygenation index (ROX index) measured after the start of high-flow nasal cannula oxygen therapy can help identify the need for intubation in patients with acute respiratory failure due to coronavirus disease 2019.
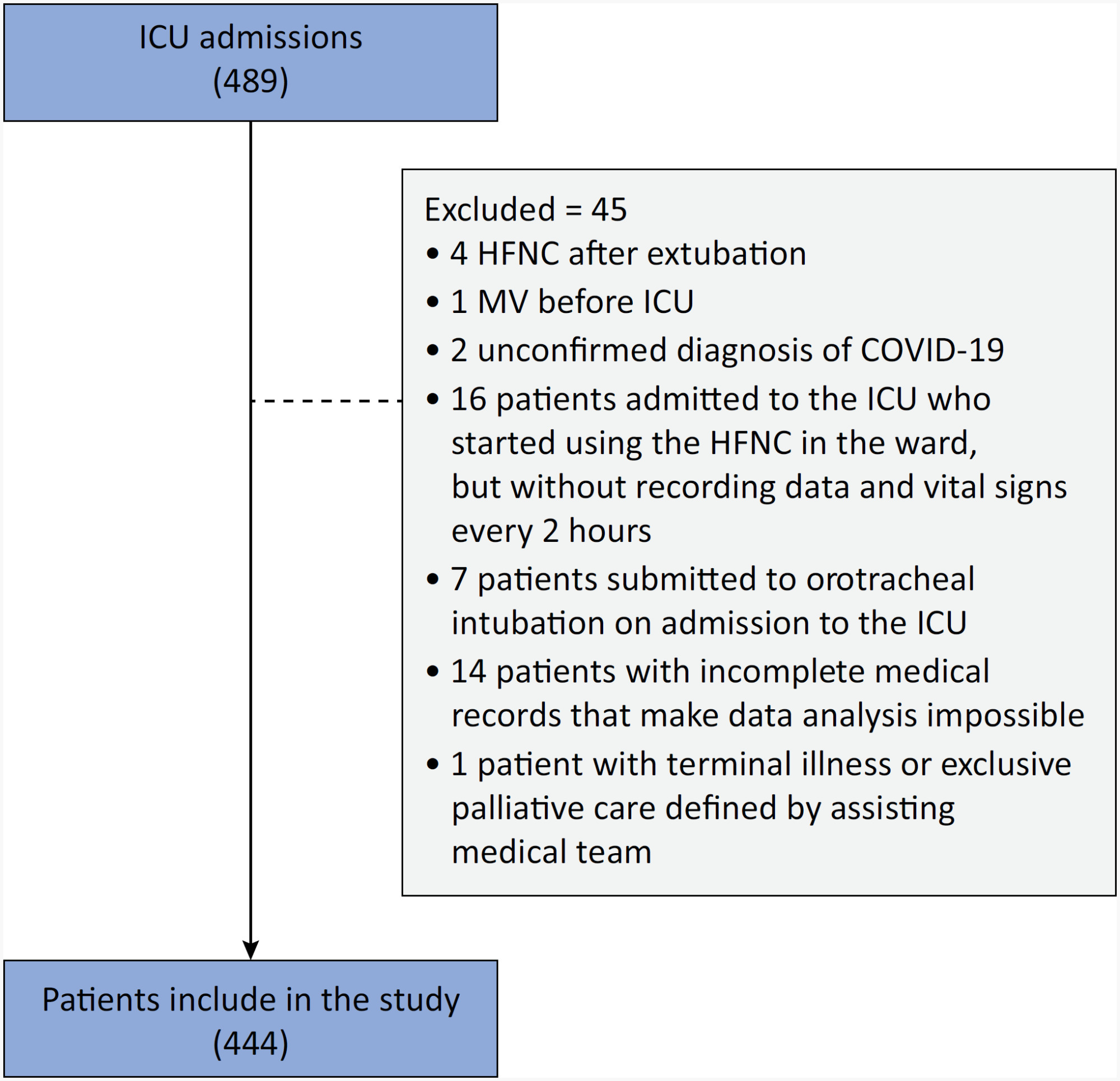
This retrospective, observational, multicenter study was conducted at the intensive care units of six Brazilian hospitals from March to December 2020. The primary outcome was the need for intubation up to 7 days after starting the high-flow nasal cannula.
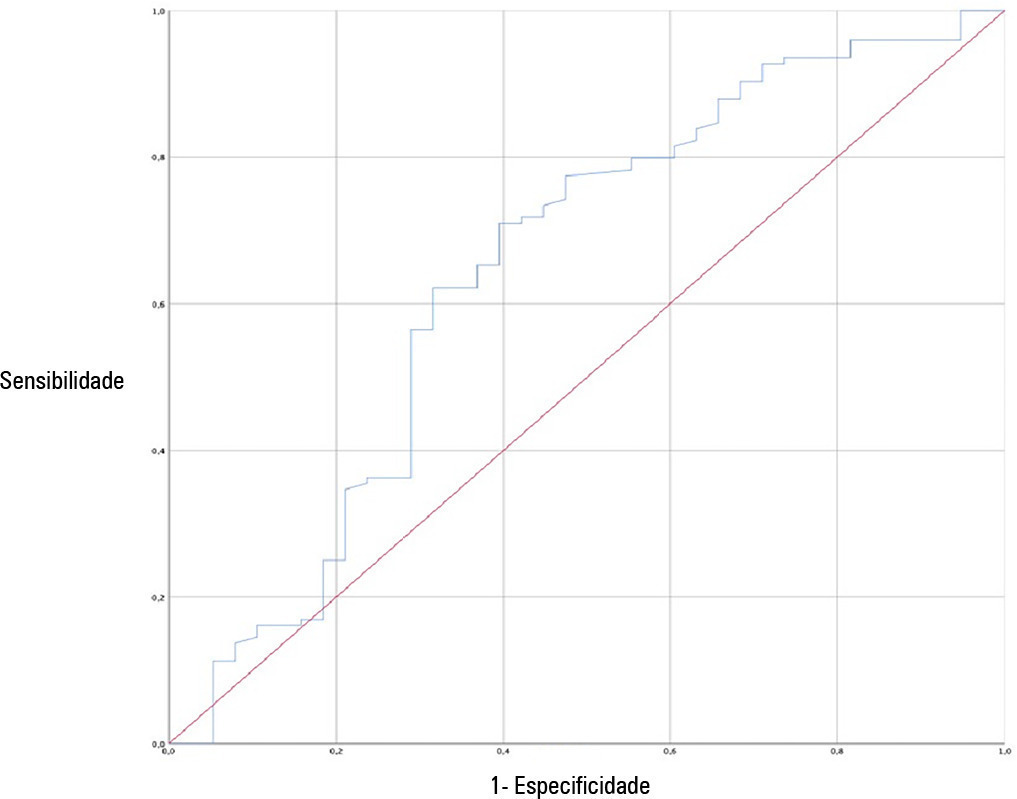
A total of 444 patients were included in the study, and 261 (58.7%) were subjected to intubation. An analysis of the area under the receiver operating characteristic curve (AUROC) showed that the ability to discriminate between successful and failed high-flow nasal cannula oxygen therapy within 7 days was greater for the ROX index measured at 24 hours (AUROC 0.80; 95%CI 0.76 - 0.84). The median interval between high-flow nasal cannula initiation and intubation was 24 hours (24 - 72), and the most accurate predictor of intubation obtained before 24 hours was the ROX index measured at 12 hours (AUROC 0.75; 95%CI 0.70 - 0.79). Kaplan-Meier curves revealed a greater probability of intubation within 7 days in patients with a ROX index ≤ 5.54 at 12 hours (hazard ratio 3.07; 95%CI 2.24 - 4.20) and ≤ 5.96 at 24 hours (hazard ratio 5.15; 95%CI 3.65 - 7.27).
The ROX index can aid in the early identification of patients with acute respiratory failure due to COVID-19 who will progress to the failure of high-flow nasal cannula supportive therapy and the need for intubation.
Abstract
Crit Care Sci. 2024;36:e20240203en
DOI 10.62675/2965-2774.20240203-en
To assess whether the respiratory oxygenation index (ROX index) measured after the start of high-flow nasal cannula oxygen therapy can help identify the need for intubation in patients with acute respiratory failure due to coronavirus disease 2019.
This retrospective, observational, multicenter study was conducted at the intensive care units of six Brazilian hospitals from March to December 2020. The primary outcome was the need for intubation up to 7 days after starting the high-flow nasal cannula.
A total of 444 patients were included in the study, and 261 (58.7%) were subjected to intubation. An analysis of the area under the receiver operating characteristic curve (AUROC) showed that the ability to discriminate between successful and failed high-flow nasal cannula oxygen therapy within 7 days was greater for the ROX index measured at 24 hours (AUROC 0.80; 95%CI 0.76 - 0.84). The median interval between high-flow nasal cannula initiation and intubation was 24 hours (24 - 72), and the most accurate predictor of intubation obtained before 24 hours was the ROX index measured at 12 hours (AUROC 0.75; 95%CI 0.70 - 0.79). Kaplan-Meier curves revealed a greater probability of intubation within 7 days in patients with a ROX index ≤ 5.54 at 12 hours (hazard ratio 3.07; 95%CI 2.24 - 4.20) and ≤ 5.96 at 24 hours (hazard ratio 5.15; 95%CI 3.65 - 7.27).
The ROX index can aid in the early identification of patients with acute respiratory failure due to COVID-19 who will progress to the failure of high-flow nasal cannula supportive therapy and the need for intubation.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):351-359
DOI 10.5935/0103-507X.20220383-en
To develop a simple, robust, safe and efficient invasive mechanical ventilator that can be used in remote areas of the world or war zones where the practical utility of more sophisticated equipment is limited by considerations of maintainability, availability of parts, transportation and/or cost.
The device implements the pressure-controlled continuous mandatory ventilation mode, complemented by a simple assist-control mode. Continuous positive airway pressure is also possible. The consumption of compressed gases is minimized by avoiding a continuous flow of oxygen or air. Respiratory rates and inspiration/expiration time ratios are electronically determined, and an apnea/power loss alarm is provided.
The pressure profiles were measured for a range of conditions and found to be adjustable within a ± 2.5cmH2O error margin and stable well within this range over a 41-hour period. Respiratory cycle timing parameters were precise within a few percentage points over the same period. The device was tested for durability for an equivalent period of four months. Chemical and biological tests failed to identify any contamination of the gas by volatile organic compounds or microorganisms. A ventilation test on a large animal, in comparison with a well established ventilator, showed that the animal could be adequately ventilated over a period of 60 minutes, without any noticeable negative aftereffects during the subsequent 24-hour period.
This ventilator design may be viable, after further animal tests and formal approval by the competent authorities, for clinical application in the abovementioned atypical circumstances.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):351-359
DOI 10.5935/0103-507X.20220383-en
To develop a simple, robust, safe and efficient invasive mechanical ventilator that can be used in remote areas of the world or war zones where the practical utility of more sophisticated equipment is limited by considerations of maintainability, availability of parts, transportation and/or cost.
The device implements the pressure-controlled continuous mandatory ventilation mode, complemented by a simple assist-control mode. Continuous positive airway pressure is also possible. The consumption of compressed gases is minimized by avoiding a continuous flow of oxygen or air. Respiratory rates and inspiration/expiration time ratios are electronically determined, and an apnea/power loss alarm is provided.
The pressure profiles were measured for a range of conditions and found to be adjustable within a ± 2.5cmH2O error margin and stable well within this range over a 41-hour period. Respiratory cycle timing parameters were precise within a few percentage points over the same period. The device was tested for durability for an equivalent period of four months. Chemical and biological tests failed to identify any contamination of the gas by volatile organic compounds or microorganisms. A ventilation test on a large animal, in comparison with a well established ventilator, showed that the animal could be adequately ventilated over a period of 60 minutes, without any noticeable negative aftereffects during the subsequent 24-hour period.
This ventilator design may be viable, after further animal tests and formal approval by the competent authorities, for clinical application in the abovementioned atypical circumstances.

Abstract
Rev Bras Ter Intensiva. 2022;34(3):360-366
DOI 10.5935/0103-507X.20220477-en
To investigate the applicability of the Respiratory Rate-Oxygenation Index to identify the risk of high-flow nasal cannula failure in post-extubation pneumonia patients.
This was a 2-year retrospective observational study conducted in a reference hospital in Bogotá, Colombia. All patients in whom post-extubation high-flow nasal cannula therapy was used as a bridge to extubation were included in the study. The Respiratory Rate-Oxygenation Index was calculated to assess the risk of post-extubation high-flow nasal cannula failure.
A total of 162 patients were included in the study. Of these, 23.5% developed high-flow nasal cannula failure. The Respiratory Rate-Oxygenation Index was significantly lower in patients who had high-flow nasal cannula failure [median (IQR): 10.0 (7.7 - 14.4) versus 12.6 (10.1 - 15.6); p = 0.006]. Respiratory Rate-Oxygenation Index > 4.88 showed a crude OR of 0.23 (95%CI 0.17 - 0.30) and an adjusted OR of 0.89 (95%CI 0.81 - 0.98) stratified by severity and comorbidity. After logistic regression analysis, the Respiratory Rate-Oxygenation Index had an adjusted OR of 0.90 (95%CI 0.82 - 0.98; p = 0.026). The area under the Receiver Operating Characteristic curve for extubation failure was 0.64 (95%CI 0.53 - 0.75; p = 0.06). The Respiratory Rate-Oxygenation Index did not show differences between patients who survived and those who died during the intensive care unit stay.
The Respiratory Rate-Oxygenation Index is an accessible tool to identify patients at risk of failing high-flow nasal cannula post-extubation treatment. Prospective studies are needed to broaden the utility in this scenario.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):360-366
DOI 10.5935/0103-507X.20220477-en
To investigate the applicability of the Respiratory Rate-Oxygenation Index to identify the risk of high-flow nasal cannula failure in post-extubation pneumonia patients.
This was a 2-year retrospective observational study conducted in a reference hospital in Bogotá, Colombia. All patients in whom post-extubation high-flow nasal cannula therapy was used as a bridge to extubation were included in the study. The Respiratory Rate-Oxygenation Index was calculated to assess the risk of post-extubation high-flow nasal cannula failure.
A total of 162 patients were included in the study. Of these, 23.5% developed high-flow nasal cannula failure. The Respiratory Rate-Oxygenation Index was significantly lower in patients who had high-flow nasal cannula failure [median (IQR): 10.0 (7.7 - 14.4) versus 12.6 (10.1 - 15.6); p = 0.006]. Respiratory Rate-Oxygenation Index > 4.88 showed a crude OR of 0.23 (95%CI 0.17 - 0.30) and an adjusted OR of 0.89 (95%CI 0.81 - 0.98) stratified by severity and comorbidity. After logistic regression analysis, the Respiratory Rate-Oxygenation Index had an adjusted OR of 0.90 (95%CI 0.82 - 0.98; p = 0.026). The area under the Receiver Operating Characteristic curve for extubation failure was 0.64 (95%CI 0.53 - 0.75; p = 0.06). The Respiratory Rate-Oxygenation Index did not show differences between patients who survived and those who died during the intensive care unit stay.
The Respiratory Rate-Oxygenation Index is an accessible tool to identify patients at risk of failing high-flow nasal cannula post-extubation treatment. Prospective studies are needed to broaden the utility in this scenario.