Physical therapy modalities Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2009;21(4):446-452
DOI 10.1590/S0103-507X2009000400016
This study aimed to review the literature addressing motor physical therapy for intensive care unit adult patients. A literature search was conducted in the databases, PubMed, MedLine (International Literature and Health), LILACS (Latin American and Caribbean Health Sciences) and Cochrane between 1995 and December 2008 using the keywords: physical therapy, mobilization and intensive care unit. For comparison purposes we selected randomized controlled trials and prospective studies, addressing the subject motor physical therapy for intensive care unit adult patients. Pediatric and experimental studies, systematic reviews and meta-analysis were excluded. Of the 121 articles identified, only 4 met the inclusion criteria. Among these, three focused early motor physical therapy in patients with a range of diagnoses, showing that these patients left the bed and walked earlier, and stayed shorter both in the intensive care unit and hospital. Furthermore, patients on early motor physical therapy had shorter mechanical ventilation duration. Another paper compares the use of electrical stimulation associated with physical therapy in chronic obstructive pulmonary disease patients, showing increased muscle strength and shorter time for these patients bed to chair transference as compared with those only receiving physiotherapy. The risks of immobilization in mechanically ventilated critically ill patients are not fully understood. However, it is clear that the survivors show impaired quality of life due to persistent weakness and fatigue. Early mobilization is a new area, with little evidence so far. However, recent studies have confirmed that mechanically ventilated patients mobilization is safe and feasible, reducing both the intensive care unit and hospital stay. However, more studies are warranted to identify the exercise type, duration, intensity and impact for of early motor therapy in specific groups of patients.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):446-452
DOI 10.1590/S0103-507X2009000400016
This study aimed to review the literature addressing motor physical therapy for intensive care unit adult patients. A literature search was conducted in the databases, PubMed, MedLine (International Literature and Health), LILACS (Latin American and Caribbean Health Sciences) and Cochrane between 1995 and December 2008 using the keywords: physical therapy, mobilization and intensive care unit. For comparison purposes we selected randomized controlled trials and prospective studies, addressing the subject motor physical therapy for intensive care unit adult patients. Pediatric and experimental studies, systematic reviews and meta-analysis were excluded. Of the 121 articles identified, only 4 met the inclusion criteria. Among these, three focused early motor physical therapy in patients with a range of diagnoses, showing that these patients left the bed and walked earlier, and stayed shorter both in the intensive care unit and hospital. Furthermore, patients on early motor physical therapy had shorter mechanical ventilation duration. Another paper compares the use of electrical stimulation associated with physical therapy in chronic obstructive pulmonary disease patients, showing increased muscle strength and shorter time for these patients bed to chair transference as compared with those only receiving physiotherapy. The risks of immobilization in mechanically ventilated critically ill patients are not fully understood. However, it is clear that the survivors show impaired quality of life due to persistent weakness and fatigue. Early mobilization is a new area, with little evidence so far. However, recent studies have confirmed that mechanically ventilated patients mobilization is safe and feasible, reducing both the intensive care unit and hospital stay. However, more studies are warranted to identify the exercise type, duration, intensity and impact for of early motor therapy in specific groups of patients.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):155-161
DOI 10.1590/S0103-507X2009000200007
OBJECTIVES: Patients unable to perform breathing functions may be submitted to invasive mechanical ventilation. Chest physiotherapy acts directly on the treatment of these patients for the purpose of improving their lung function. The objective of this study was to evaluate the effects of manual rib-cage compression versus the positive end expiratory pressure-zero end expiratory pressure (PEEP-ZEEP) maneuver, on compliance of the respiratory system and oxygenation in patients under invasive mechanical ventilation. METHODS: A double centric, prospective, randomized and crossover study, with patients under invasive mechanical ventilation, in controlled mode for more than 48 hours was carried out. The protocols of chest physiothe-rapy were randomly applied at an interval of 24 hours. Data of respiratory system compliance and oxygenation were collected before application of the protocols and 30 minutes after. RESULTS: Twelve patients completed the study. Intragroup analysis, for both techniques showed a statistically significant difference in tidal volume (p=0.002), static compliance (p=0.002) and dynamic compliance (p=0.002). In relation to oxygenation, in the group of manual rib-cage compression, peripheral oxygen saturation increased with a significant difference (p=0.011). CONCLUSIONS: Manual rib-cage compression and PEEP-ZEEP maneuver have positive clinical effects. In relation to oxygenation we found a favorable behavior of peripheral oxygen saturation in the group of manual rib-cage compression.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):155-161
DOI 10.1590/S0103-507X2009000200007
OBJECTIVES: Patients unable to perform breathing functions may be submitted to invasive mechanical ventilation. Chest physiotherapy acts directly on the treatment of these patients for the purpose of improving their lung function. The objective of this study was to evaluate the effects of manual rib-cage compression versus the positive end expiratory pressure-zero end expiratory pressure (PEEP-ZEEP) maneuver, on compliance of the respiratory system and oxygenation in patients under invasive mechanical ventilation. METHODS: A double centric, prospective, randomized and crossover study, with patients under invasive mechanical ventilation, in controlled mode for more than 48 hours was carried out. The protocols of chest physiothe-rapy were randomly applied at an interval of 24 hours. Data of respiratory system compliance and oxygenation were collected before application of the protocols and 30 minutes after. RESULTS: Twelve patients completed the study. Intragroup analysis, for both techniques showed a statistically significant difference in tidal volume (p=0.002), static compliance (p=0.002) and dynamic compliance (p=0.002). In relation to oxygenation, in the group of manual rib-cage compression, peripheral oxygen saturation increased with a significant difference (p=0.011). CONCLUSIONS: Manual rib-cage compression and PEEP-ZEEP maneuver have positive clinical effects. In relation to oxygenation we found a favorable behavior of peripheral oxygen saturation in the group of manual rib-cage compression.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):183-189
DOI 10.1590/S0103-507X2009000200011
OBJECTIVES: This research aimed to evaluate the repercussions of specific chest physiotherapy procedures in mean airway resistance and in dynamic compliance in preterm infants in mechanical ventilation. METHODS: Eighteen preterm infants in conventional mechanical ventilation were submitted to one session of chest physiotherapy (manual chest compression during expiration + intermittent aspiration of intratracheal cannula). Mean airway resistance and dynamic compliance measurements were taken prior to, 10, 40 and 70 minutes after intervention using a pneumotachograph with graphic display (Newport Navigator GM-250®), coupled to a flow transducer (Varfley-Bicore®). For analysis of results the infants were divided into 2 groups; less than 5 days (group mechanical ventilation <5) and 5 days or more (group mechanical ventilation >5) on mechanical ventilation. Values were analyzed by Friedman Test, with Dunn's Multiple Comparisons Test (p<0,05 significant). RESULTS: In group mechanical ventilation <5 a significant reduction of mean airway resistance was observed at the 10th minute after intervention (p<0,05). There were no significant alterations in dynamic compliance. The group mechanical ventilation >5 mean airway resistance had a significant reduction at the 10th (p<0,001), 40th (p<0,05) and 70th (p<0,05) minute after intervention. The dynamic compliance improved significantly only at the 10th minute (p<0,05). CONCLUSIONS: The airway clearance techniques used in preterm neonates under conventional mechanical ventilation >5 improved mean airway resistance and dynamic compliance, with best results for the mean airway resistance.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):183-189
DOI 10.1590/S0103-507X2009000200011
OBJECTIVES: This research aimed to evaluate the repercussions of specific chest physiotherapy procedures in mean airway resistance and in dynamic compliance in preterm infants in mechanical ventilation. METHODS: Eighteen preterm infants in conventional mechanical ventilation were submitted to one session of chest physiotherapy (manual chest compression during expiration + intermittent aspiration of intratracheal cannula). Mean airway resistance and dynamic compliance measurements were taken prior to, 10, 40 and 70 minutes after intervention using a pneumotachograph with graphic display (Newport Navigator GM-250®), coupled to a flow transducer (Varfley-Bicore®). For analysis of results the infants were divided into 2 groups; less than 5 days (group mechanical ventilation <5) and 5 days or more (group mechanical ventilation >5) on mechanical ventilation. Values were analyzed by Friedman Test, with Dunn's Multiple Comparisons Test (p<0,05 significant). RESULTS: In group mechanical ventilation <5 a significant reduction of mean airway resistance was observed at the 10th minute after intervention (p<0,05). There were no significant alterations in dynamic compliance. The group mechanical ventilation >5 mean airway resistance had a significant reduction at the 10th (p<0,001), 40th (p<0,05) and 70th (p<0,05) minute after intervention. The dynamic compliance improved significantly only at the 10th minute (p<0,05). CONCLUSIONS: The airway clearance techniques used in preterm neonates under conventional mechanical ventilation >5 improved mean airway resistance and dynamic compliance, with best results for the mean airway resistance.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):339-343
DOI 10.1590/S0103-507X2008000400004
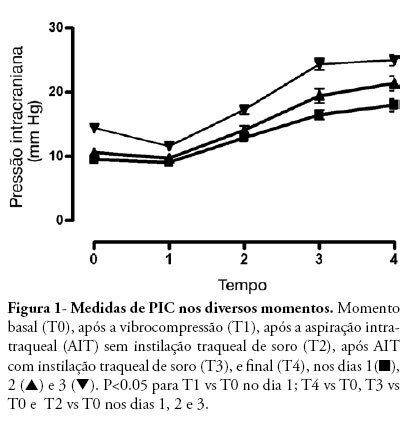
OBJECTIVE: After brain injury intracranial hypertension is the major cause of mortality, in addition to the possibility of functional, behavioral and cognitive sequels. Scarcity of studies on the effects of respiratory physiotherapy on these patients may lead to contradictory performances. This study aimed to assess the effects of customary respiratory physiotherapy maneuvers on intracranial and cerebral perfusion pressures in patients with severe brain injury. METHODS: Clinical, prospective trial with patients with severe traumatic brain injury, mechanically ventilated and with a continued measurement of intracranial pressure. The effects of manual vibrocompression maneuvers and intratracheal aspiration with or without saline infusion on the measurements of intracranial and cerebral perfusion pressures, between the first and third day after cerebral injury were evaluated. RESULTS: Data were collected from 11 patients, 41 years of age (median) and APACHE II of 19.5 ± 5. The manual vibrocompression maneuver did not cause an increase of intracranial pressure on any of the days assessed. Intracranial pressure significantly increased after intratracheal aspiration maneuvers in relation to the basal measurement (day1, 9.5 ± 0.9 mm Hg vs 18.0 ± 3.2 mm Hg; day 2, 10.6 ± 1.7 mm Hg vs 21.4 ± 3.8 mm Hg; day 3, 14.4 ± 1.0 vs 24.9 ± 2.7 mm Hg; p<0.05 for all). However, these elevations were transient (about 27 seconds) and accompanied by compensatory increases of the cerebral perfusion pressure. CONCLUSION: The manual vibrocompression maneuver did not increase intracranial pressure or cerebral perfusion pressure in patients with severe brain injury. Intratracheal aspiration induced a significant and transient increase of the intracranial and cerebral perfusion pressures.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):339-343
DOI 10.1590/S0103-507X2008000400004
OBJECTIVE: After brain injury intracranial hypertension is the major cause of mortality, in addition to the possibility of functional, behavioral and cognitive sequels. Scarcity of studies on the effects of respiratory physiotherapy on these patients may lead to contradictory performances. This study aimed to assess the effects of customary respiratory physiotherapy maneuvers on intracranial and cerebral perfusion pressures in patients with severe brain injury. METHODS: Clinical, prospective trial with patients with severe traumatic brain injury, mechanically ventilated and with a continued measurement of intracranial pressure. The effects of manual vibrocompression maneuvers and intratracheal aspiration with or without saline infusion on the measurements of intracranial and cerebral perfusion pressures, between the first and third day after cerebral injury were evaluated. RESULTS: Data were collected from 11 patients, 41 years of age (median) and APACHE II of 19.5 ± 5. The manual vibrocompression maneuver did not cause an increase of intracranial pressure on any of the days assessed. Intracranial pressure significantly increased after intratracheal aspiration maneuvers in relation to the basal measurement (day1, 9.5 ± 0.9 mm Hg vs 18.0 ± 3.2 mm Hg; day 2, 10.6 ± 1.7 mm Hg vs 21.4 ± 3.8 mm Hg; day 3, 14.4 ± 1.0 vs 24.9 ± 2.7 mm Hg; p<0.05 for all). However, these elevations were transient (about 27 seconds) and accompanied by compensatory increases of the cerebral perfusion pressure. CONCLUSION: The manual vibrocompression maneuver did not increase intracranial pressure or cerebral perfusion pressure in patients with severe brain injury. Intratracheal aspiration induced a significant and transient increase of the intracranial and cerebral perfusion pressures.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)