Critical care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(3):353-361
DOI 10.5935/0103-507X.20210051
To translate and cross-culturally adapt the Early Rehabilitation Index to Brazilian Portuguese and validate the Early Rehabilitation Barthel Index for use in the intensive care unit to assess functional status.
The following steps were performed: preparation, translation, reconciliation, back-translation, revision, harmonization, pretesting, and psychometric evaluation. After this initial process, the Portuguese version was applied by two evaluators to patients hospitalized in the intensive care unit for at least 48 hours. The reliability of the scale was assessed by internal consistency, interrater reliability, and floor and ceiling effects. To measure construct validity, the Early Rehabilitation Barthel Index was correlated with instruments typically used to assess functional status in the intensive care unit.
A total of 122 patients with a median age of 56 (46.8 - 66) years participated in the study. The Early Rehabilitation Barthel Index had adequate reliability, with a Cronbach’s alpha coefficient of 0.65. The interrater reliability was excellent, with an intraclass correlation coefficient of 0.94 (95%CI 0.92 - 0.96), and agreement was moderate to excellent, with a kappa agreement index of 0.54 to 1.0. The floor and ceiling effects were minimal. The validity of the Early Rehabilitation Barthel Index was observed through its correlations with the total Perme score (rho = 0.72), the Functional Status Score for the ICU (rho = 0.77), the Physical Function in the Intensive Care Test score (rho = 0.69), and the Medical Research Council sum score (rho = 0.58), in addition to handgrip strength (rho = 0.58) and knee extensor strength measured by hand-held dynamometry (rho = 0.55), all with p < 0.001.
The adapted versions of the Early Rehabilitation Index for Brazilian Portuguese and, in its entirety, the Early Rehabilitation Barthel Index are reliable and valid for assessing the functional status of patients at discharge from the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):353-361
DOI 10.5935/0103-507X.20210051
To translate and cross-culturally adapt the Early Rehabilitation Index to Brazilian Portuguese and validate the Early Rehabilitation Barthel Index for use in the intensive care unit to assess functional status.
The following steps were performed: preparation, translation, reconciliation, back-translation, revision, harmonization, pretesting, and psychometric evaluation. After this initial process, the Portuguese version was applied by two evaluators to patients hospitalized in the intensive care unit for at least 48 hours. The reliability of the scale was assessed by internal consistency, interrater reliability, and floor and ceiling effects. To measure construct validity, the Early Rehabilitation Barthel Index was correlated with instruments typically used to assess functional status in the intensive care unit.
A total of 122 patients with a median age of 56 (46.8 - 66) years participated in the study. The Early Rehabilitation Barthel Index had adequate reliability, with a Cronbach’s alpha coefficient of 0.65. The interrater reliability was excellent, with an intraclass correlation coefficient of 0.94 (95%CI 0.92 - 0.96), and agreement was moderate to excellent, with a kappa agreement index of 0.54 to 1.0. The floor and ceiling effects were minimal. The validity of the Early Rehabilitation Barthel Index was observed through its correlations with the total Perme score (rho = 0.72), the Functional Status Score for the ICU (rho = 0.77), the Physical Function in the Intensive Care Test score (rho = 0.69), and the Medical Research Council sum score (rho = 0.58), in addition to handgrip strength (rho = 0.58) and knee extensor strength measured by hand-held dynamometry (rho = 0.55), all with p < 0.001.
The adapted versions of the Early Rehabilitation Index for Brazilian Portuguese and, in its entirety, the Early Rehabilitation Barthel Index are reliable and valid for assessing the functional status of patients at discharge from the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):394-400
DOI 10.5935/0103-507X.20210064
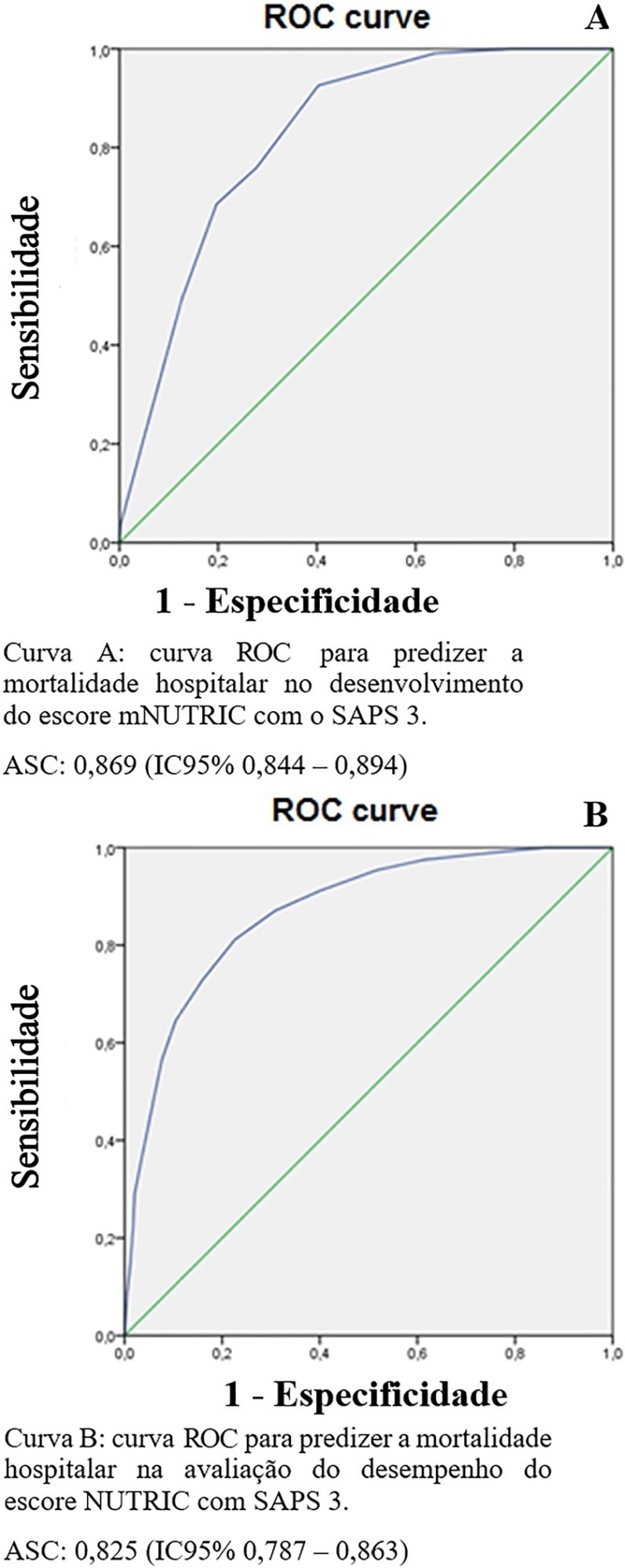
To evaluate the substitution of Acute Physiology and Chronic Health Evaluation II (APACHE II) by Simplified Acute Physiology Score 3 (SAPS 3) as a severity marker in the modified version of the NUTrition RIsk in the Critically ill score (mNUTRIC); without interleukin 6) based on an analysis of its discriminative ability for in-hospital mortality prediction.
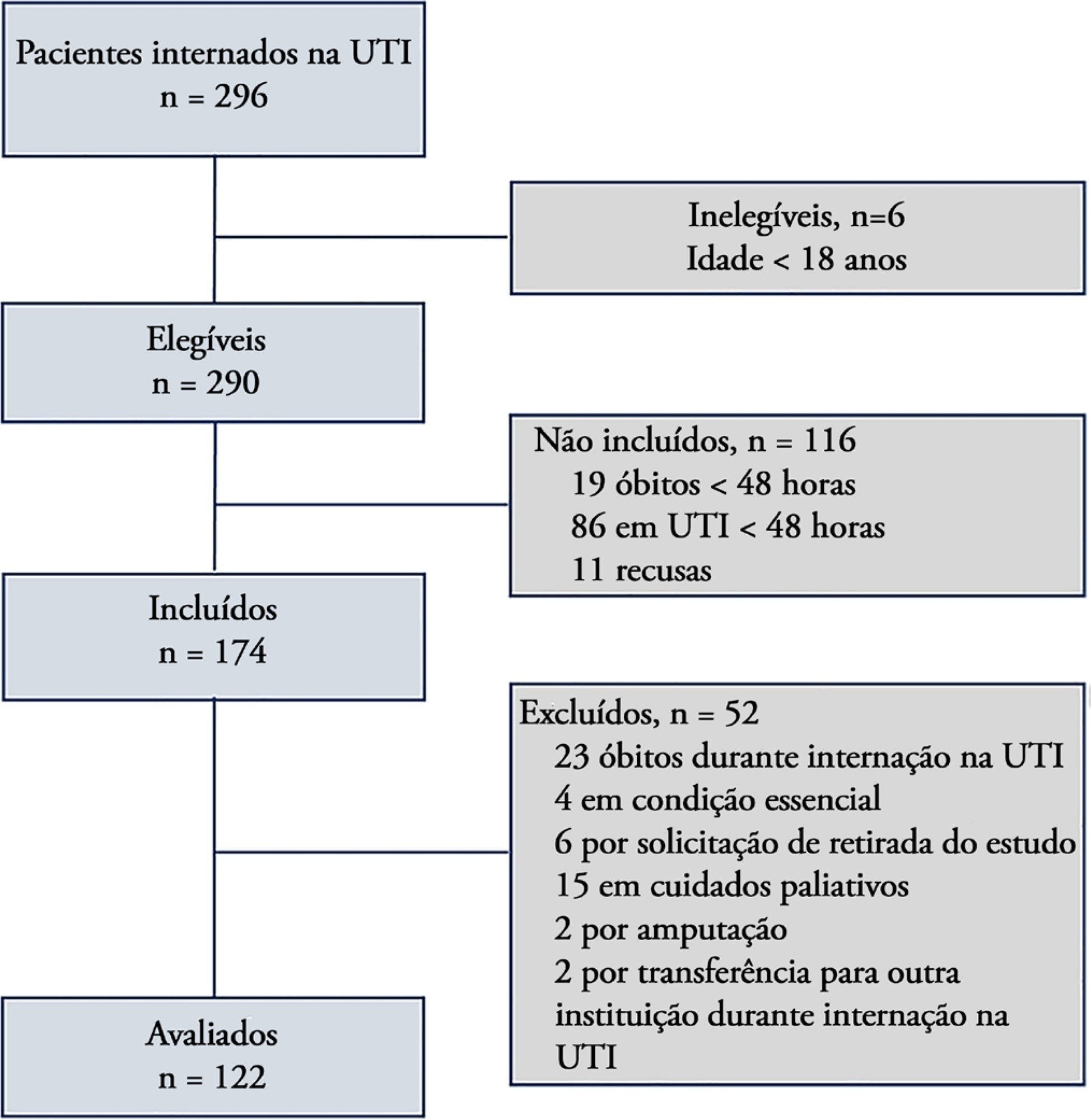
This retrospective cohort study evaluated 1,516 adult patients admitted to an intensive care unit of a private general hospital from April 2017 to January 2018. Performance evaluation included Fleiss’ Kappa and Pearson correlation analysis. The discriminative ability for estimating in-hospital mortality was assessed with the Receiver Operating Characteristic curve.
The sample was randomly divided into two-thirds for model development (n = 1,025; age 72 [57 - 83]; 52.4% male) and one-third for performance evaluation (n = 490; age 72 [57 - 83]; 50.8% male). The agreement with mNUTRIC was Kappa of 0.563 (p < 0.001), and the correlation between the instruments was Pearson correlation of 0.804 (p < 0.001). The tool showed good performance in predicting in-hospital mortality (area under the curve 0.825 [0.787 - 0.863] p < 0.001).
The substitution of APACHE II by SAPS 3 as a severity marker in the mNUTRIC score showed good performance in predicting in-hospital mortality. These data provide the first evidence regarding the validity of the substitution of APACHE II by SAPS 3 in the mNUTRIC as a marker of severity. Multicentric studies and additional analyses of nutritional adequacy parameters are required.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):394-400
DOI 10.5935/0103-507X.20210064
To evaluate the substitution of Acute Physiology and Chronic Health Evaluation II (APACHE II) by Simplified Acute Physiology Score 3 (SAPS 3) as a severity marker in the modified version of the NUTrition RIsk in the Critically ill score (mNUTRIC); without interleukin 6) based on an analysis of its discriminative ability for in-hospital mortality prediction.
This retrospective cohort study evaluated 1,516 adult patients admitted to an intensive care unit of a private general hospital from April 2017 to January 2018. Performance evaluation included Fleiss’ Kappa and Pearson correlation analysis. The discriminative ability for estimating in-hospital mortality was assessed with the Receiver Operating Characteristic curve.
The sample was randomly divided into two-thirds for model development (n = 1,025; age 72 [57 - 83]; 52.4% male) and one-third for performance evaluation (n = 490; age 72 [57 - 83]; 50.8% male). The agreement with mNUTRIC was Kappa of 0.563 (p < 0.001), and the correlation between the instruments was Pearson correlation of 0.804 (p < 0.001). The tool showed good performance in predicting in-hospital mortality (area under the curve 0.825 [0.787 - 0.863] p < 0.001).
The substitution of APACHE II by SAPS 3 as a severity marker in the mNUTRIC score showed good performance in predicting in-hospital mortality. These data provide the first evidence regarding the validity of the substitution of APACHE II by SAPS 3 in the mNUTRIC as a marker of severity. Multicentric studies and additional analyses of nutritional adequacy parameters are required.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):401-411
DOI 10.5935/0103-507X.20210050
To understand the perception of patients about medical communication as well as their needs during hospitalization in the intensive care unit.
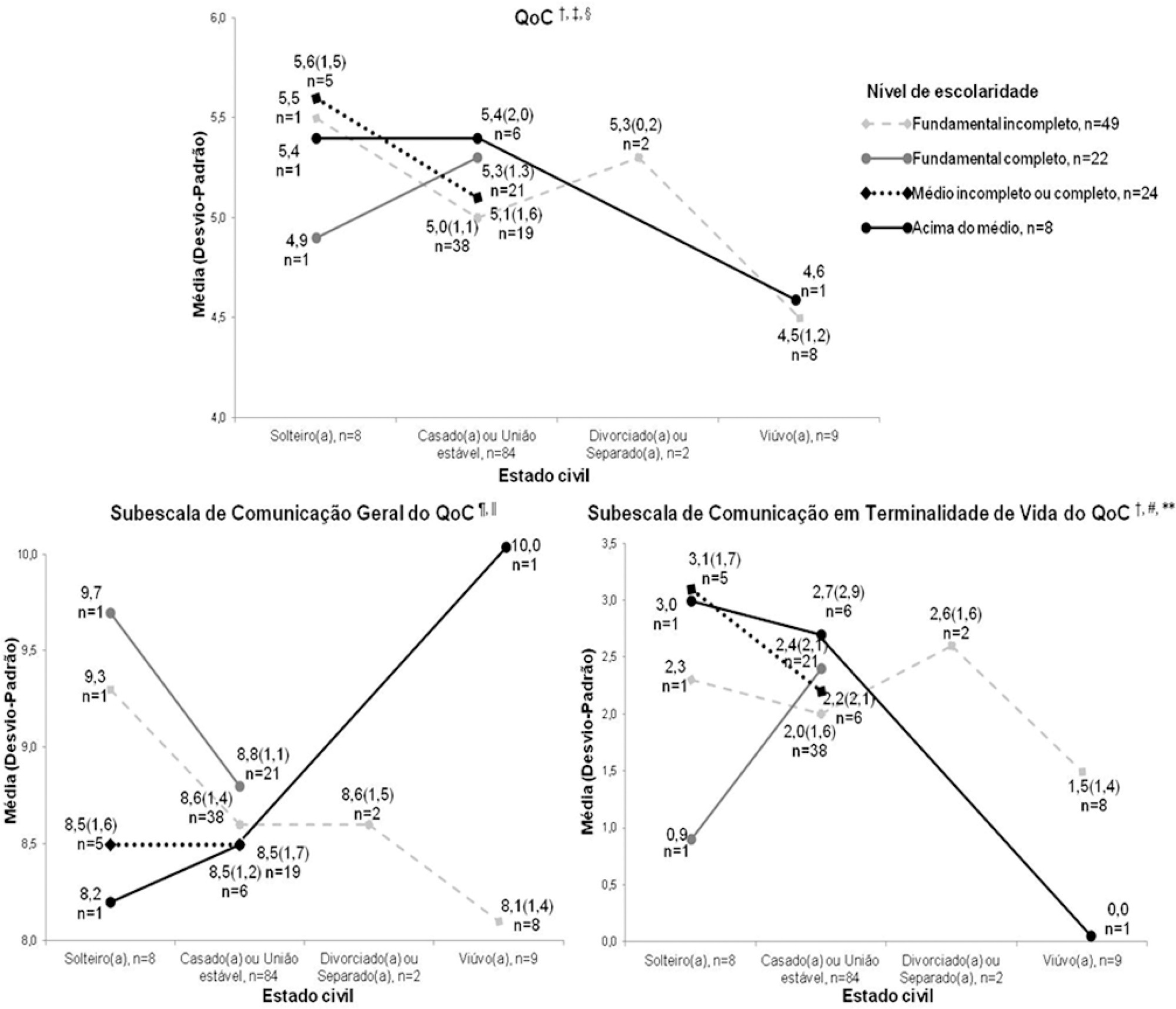
This study was cross-sectional descriptive and qualitative exploratory including 103 patients admitted to or recently discharged from the intensive care units of four hospitals in Greater Florianópolis, Santa Catarina state, Brazil. The patients’ sociodemographic and clinical variables were studied, as were the score they gave to the quality of medical communication through the Quality of Communication Questionnaire and their spontaneous comments with reflections or justifications for the scores given, and their responses on how they felt and what complementary help they would have liked to receive. The quantitative data were analyzed by descriptive and analytical statistics, and the qualitative data were analyzed by thematic content analysis.
The mean Quality of Communication Questionnaire score was 5.1 (standard deviation - SD = 1.3), with 8.6 (SD = 1.3) on the general communication subscale and 2.1 (SD = 1.8) on the end-of-life communication subscale. The patients had a variable understanding of medical language. Some physicians seemed to be “rushed”, according to some patients. Other patients would like to receive more frequent and detailed information and/or be respected and taken “more seriously” when they reported pain. Anxiety, sadness, and fear were among the reported feelings. Other needs included silence, more time for visits, the presence of a companion, psychological and social-work care, a bathroom that they could use, and better food in the intensive care unit.
The quality of medical communication with patients is good but could improve if physicians and the healthcare team had more time for patients. Other felt needs included respect, pain relief, and adjustments in the intensive care unit dynamics and environment.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):401-411
DOI 10.5935/0103-507X.20210050
To understand the perception of patients about medical communication as well as their needs during hospitalization in the intensive care unit.
This study was cross-sectional descriptive and qualitative exploratory including 103 patients admitted to or recently discharged from the intensive care units of four hospitals in Greater Florianópolis, Santa Catarina state, Brazil. The patients’ sociodemographic and clinical variables were studied, as were the score they gave to the quality of medical communication through the Quality of Communication Questionnaire and their spontaneous comments with reflections or justifications for the scores given, and their responses on how they felt and what complementary help they would have liked to receive. The quantitative data were analyzed by descriptive and analytical statistics, and the qualitative data were analyzed by thematic content analysis.
The mean Quality of Communication Questionnaire score was 5.1 (standard deviation - SD = 1.3), with 8.6 (SD = 1.3) on the general communication subscale and 2.1 (SD = 1.8) on the end-of-life communication subscale. The patients had a variable understanding of medical language. Some physicians seemed to be “rushed”, according to some patients. Other patients would like to receive more frequent and detailed information and/or be respected and taken “more seriously” when they reported pain. Anxiety, sadness, and fear were among the reported feelings. Other needs included silence, more time for visits, the presence of a companion, psychological and social-work care, a bathroom that they could use, and better food in the intensive care unit.
The quality of medical communication with patients is good but could improve if physicians and the healthcare team had more time for patients. Other felt needs included respect, pain relief, and adjustments in the intensive care unit dynamics and environment.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):469-476
DOI 10.5935/0103-507X.20210066
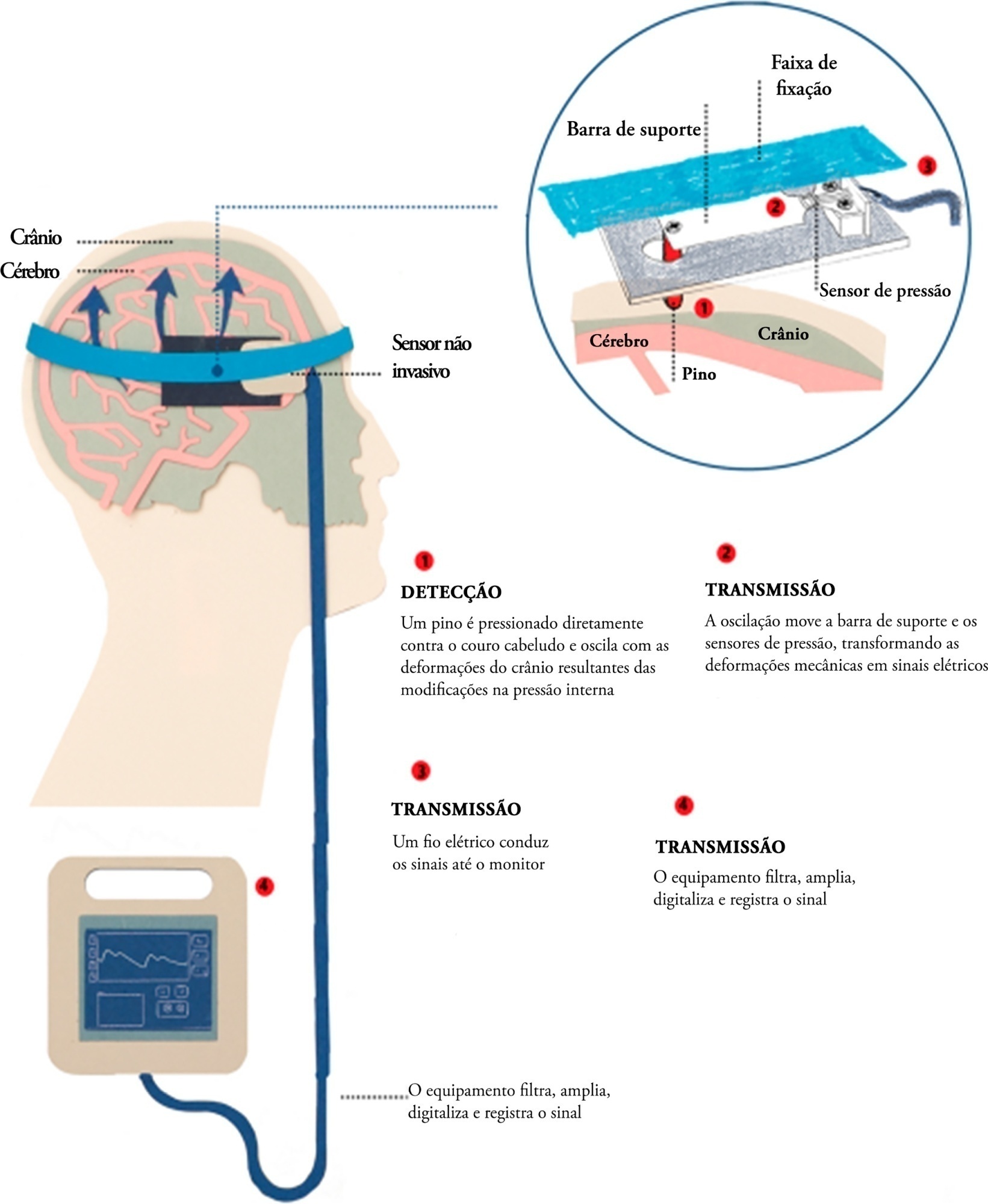
Brain injury caused by extracorporeal circulation during cardiovascular surgical procedures has been a recurring complication since the implementation of extracorporeal circulation five decades ago. There is no unique cause of brain injury due to the use of extracorporeal circulation, but it is known that brain injury affects about 70% of patients who undergo this procedure. Intracranial pressure assessment is one method that can guide the management of patients undergoing procedures associated with neurological disturbances. This study describes two cases of patients who underwent cardiovascular surgery with extracorporeal circulation in whom clinical protocols for neuroprotection in the postoperative phase were guided by intracranial pressure waveform findings obtained with a novel noninvasive intracranial pressure monitoring method.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):469-476
DOI 10.5935/0103-507X.20210066
Brain injury caused by extracorporeal circulation during cardiovascular surgical procedures has been a recurring complication since the implementation of extracorporeal circulation five decades ago. There is no unique cause of brain injury due to the use of extracorporeal circulation, but it is known that brain injury affects about 70% of patients who undergo this procedure. Intracranial pressure assessment is one method that can guide the management of patients undergoing procedures associated with neurological disturbances. This study describes two cases of patients who underwent cardiovascular surgery with extracorporeal circulation in whom clinical protocols for neuroprotection in the postoperative phase were guided by intracranial pressure waveform findings obtained with a novel noninvasive intracranial pressure monitoring method.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):206-218
DOI 10.5935/0103-507X.20210028
To describe fluid resuscitation practices in Brazilian intensive care units and to compare them with those of other countries participating in the Fluid-TRIPS.
This was a prospective, international, cross-sectional, observational study in a convenience sample of intensive care units in 27 countries (including Brazil) using the Fluid-TRIPS database compiled in 2014. We described the patterns of fluid resuscitation use in Brazil compared with those in other countries and identified the factors associated with fluid choice.
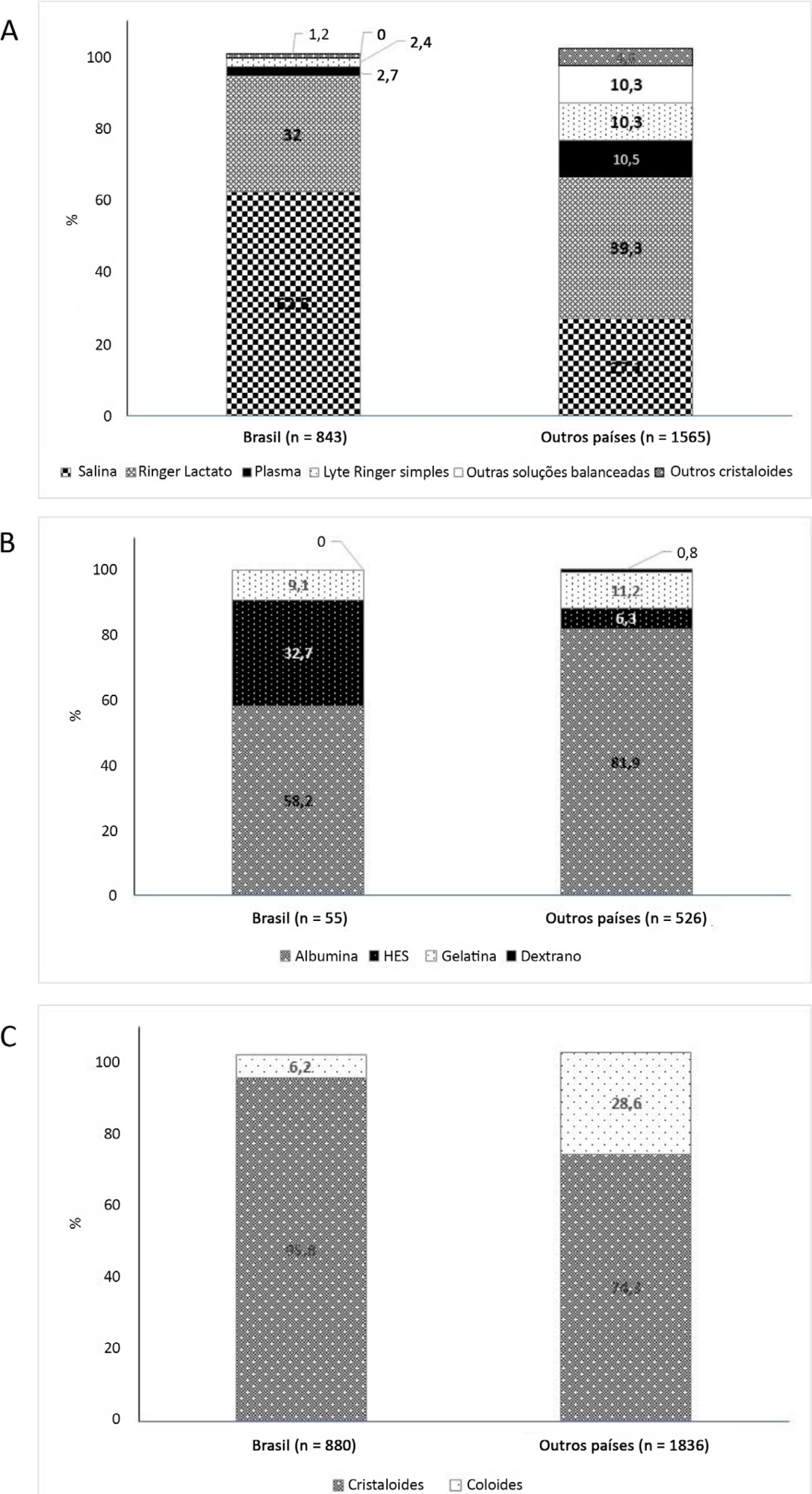
On the study day, 3,214 patients in Brazil and 3,493 patients in other countries were included, of whom 16.1% and 26.8% (p < 0.001) received fluids, respectively. The main indication for fluid resuscitation was impaired perfusion and/or low cardiac output (Brazil: 71.7% versus other countries: 56.4%, p < 0.001). In Brazil, the percentage of patients receiving crystalloid solutions was higher (97.7% versus 76.8%, p < 0.001), and 0.9% sodium chloride was the most commonly used crystalloid (62.5% versus 27.1%, p < 0.001). The multivariable analysis suggested that the albumin levels were associated with the use of both crystalloids and colloids, whereas the type of fluid prescriber was associated with crystalloid use only.
Our results suggest that crystalloids are more frequently used than colloids for fluid resuscitation in Brazil, and this discrepancy in frequencies is higher than that in other countries. Sodium chloride (0.9%) was the crystalloid most commonly prescribed. Serum albumin levels and the type of fluid prescriber were the factors associated with the choice of crystalloids or colloids for fluid resuscitation.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):206-218
DOI 10.5935/0103-507X.20210028
To describe fluid resuscitation practices in Brazilian intensive care units and to compare them with those of other countries participating in the Fluid-TRIPS.
This was a prospective, international, cross-sectional, observational study in a convenience sample of intensive care units in 27 countries (including Brazil) using the Fluid-TRIPS database compiled in 2014. We described the patterns of fluid resuscitation use in Brazil compared with those in other countries and identified the factors associated with fluid choice.
On the study day, 3,214 patients in Brazil and 3,493 patients in other countries were included, of whom 16.1% and 26.8% (p < 0.001) received fluids, respectively. The main indication for fluid resuscitation was impaired perfusion and/or low cardiac output (Brazil: 71.7% versus other countries: 56.4%, p < 0.001). In Brazil, the percentage of patients receiving crystalloid solutions was higher (97.7% versus 76.8%, p < 0.001), and 0.9% sodium chloride was the most commonly used crystalloid (62.5% versus 27.1%, p < 0.001). The multivariable analysis suggested that the albumin levels were associated with the use of both crystalloids and colloids, whereas the type of fluid prescriber was associated with crystalloid use only.
Our results suggest that crystalloids are more frequently used than colloids for fluid resuscitation in Brazil, and this discrepancy in frequencies is higher than that in other countries. Sodium chloride (0.9%) was the crystalloid most commonly prescribed. Serum albumin levels and the type of fluid prescriber were the factors associated with the choice of crystalloids or colloids for fluid resuscitation.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):219-230
DOI 10.5935/0103-507X.20210029
To assess the impact of intensive care unit bed availability, distractors and choice framing on intensive care unit admission decisions.
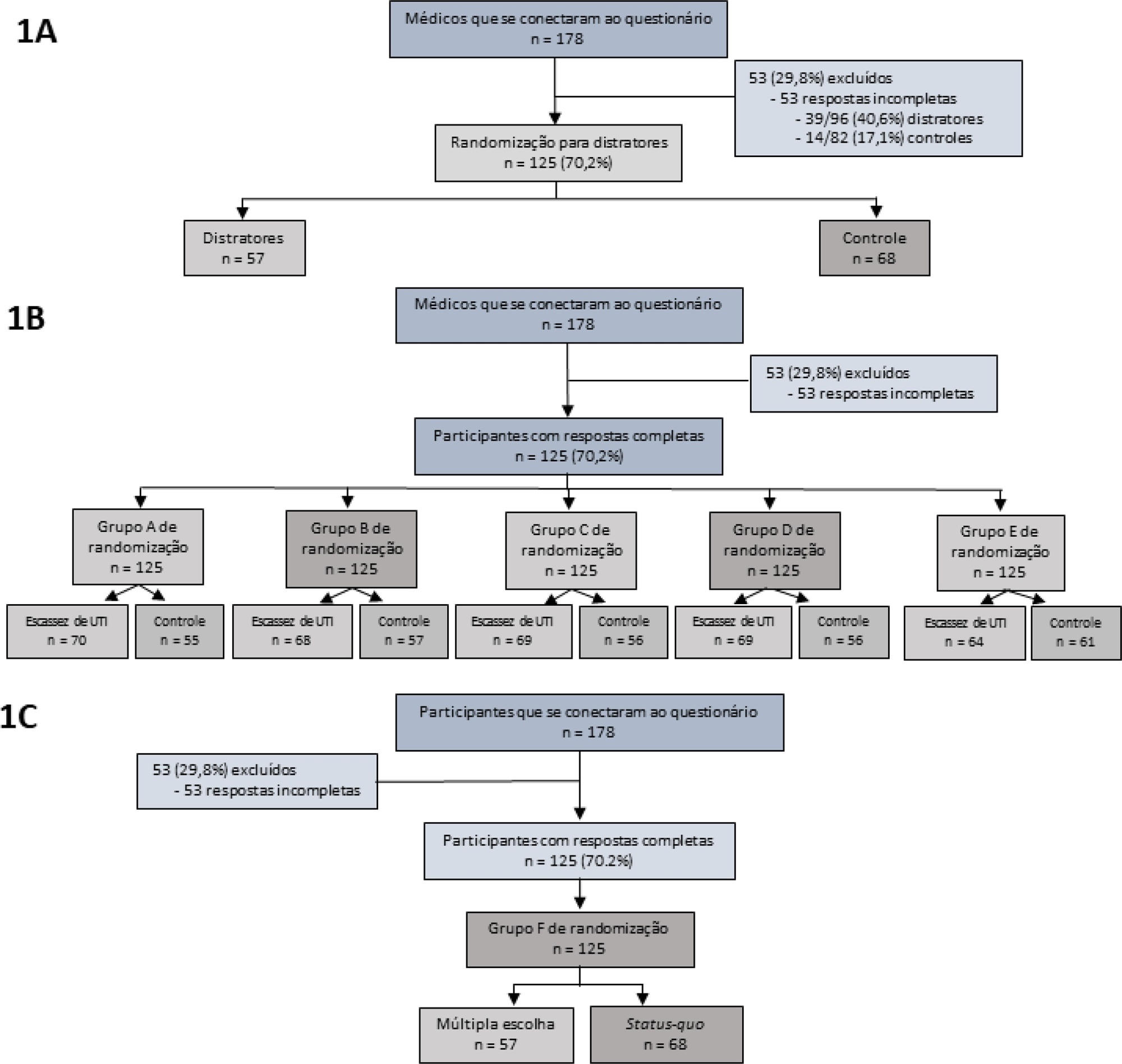
This study was a randomized factorial trial using patient-based vignettes. The vignettes were deemed archetypical for intensive care unit admission or refusal, as judged by a group of experts. Intensive care unit physicians were randomized to 1) an increased distraction (intervention) or a control group, 2) an intensive care unit bed scarcity or nonscarcity (availability) setting, and 3) a multiple-choice or omission (status quo) vignette scenario. The primary outcome was the proportion of appropriate intensive care unit allocations, defined as concordance with the allocation decision made by the group of experts.
We analyzed 125 physicians. Overall, distractors had no impact on the outcome; however, there was a differential drop-out rate, with fewer physicians in the intervention arm completing the questionnaire. Intensive care unit bed availability was associated with an inappropriate allocation of vignettes deemed inappropriate for intensive care unit admission (OR = 2.47; 95%CI 1.19 - 5.11) but not of vignettes appropriate for intensive care unit admission. There was a significant interaction with the presence of distractors (p = 0.007), with intensive care unit bed availability being associated with increased intensive care unit admission of vignettes inappropriate for intensive care unit admission in the distractor (intervention) arm (OR = 9.82; 95%CI 2.68 - 25.93) but not in the control group (OR = 1.02; 95%CI 0.38 - 2.72). Multiple choices were associated with increased inappropriate allocation in comparison to the omission group (OR = 5.18; 95%CI 1.37 - 19.61).
Intensive care unit bed availability and cognitive biases were associated with inappropriate intensive care unit allocation decisions. These findings may have implications for intensive care unit admission policies.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):219-230
DOI 10.5935/0103-507X.20210029
To assess the impact of intensive care unit bed availability, distractors and choice framing on intensive care unit admission decisions.
This study was a randomized factorial trial using patient-based vignettes. The vignettes were deemed archetypical for intensive care unit admission or refusal, as judged by a group of experts. Intensive care unit physicians were randomized to 1) an increased distraction (intervention) or a control group, 2) an intensive care unit bed scarcity or nonscarcity (availability) setting, and 3) a multiple-choice or omission (status quo) vignette scenario. The primary outcome was the proportion of appropriate intensive care unit allocations, defined as concordance with the allocation decision made by the group of experts.
We analyzed 125 physicians. Overall, distractors had no impact on the outcome; however, there was a differential drop-out rate, with fewer physicians in the intervention arm completing the questionnaire. Intensive care unit bed availability was associated with an inappropriate allocation of vignettes deemed inappropriate for intensive care unit admission (OR = 2.47; 95%CI 1.19 - 5.11) but not of vignettes appropriate for intensive care unit admission. There was a significant interaction with the presence of distractors (p = 0.007), with intensive care unit bed availability being associated with increased intensive care unit admission of vignettes inappropriate for intensive care unit admission in the distractor (intervention) arm (OR = 9.82; 95%CI 2.68 - 25.93) but not in the control group (OR = 1.02; 95%CI 0.38 - 2.72). Multiple choices were associated with increased inappropriate allocation in comparison to the omission group (OR = 5.18; 95%CI 1.37 - 19.61).
Intensive care unit bed availability and cognitive biases were associated with inappropriate intensive care unit allocation decisions. These findings may have implications for intensive care unit admission policies.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):243-250
DOI 10.5935/0103-507X.20210031
To relate functional independence to the degree of pulmonary impairment in adult patients 3 months after discharge from the intensive care unit.
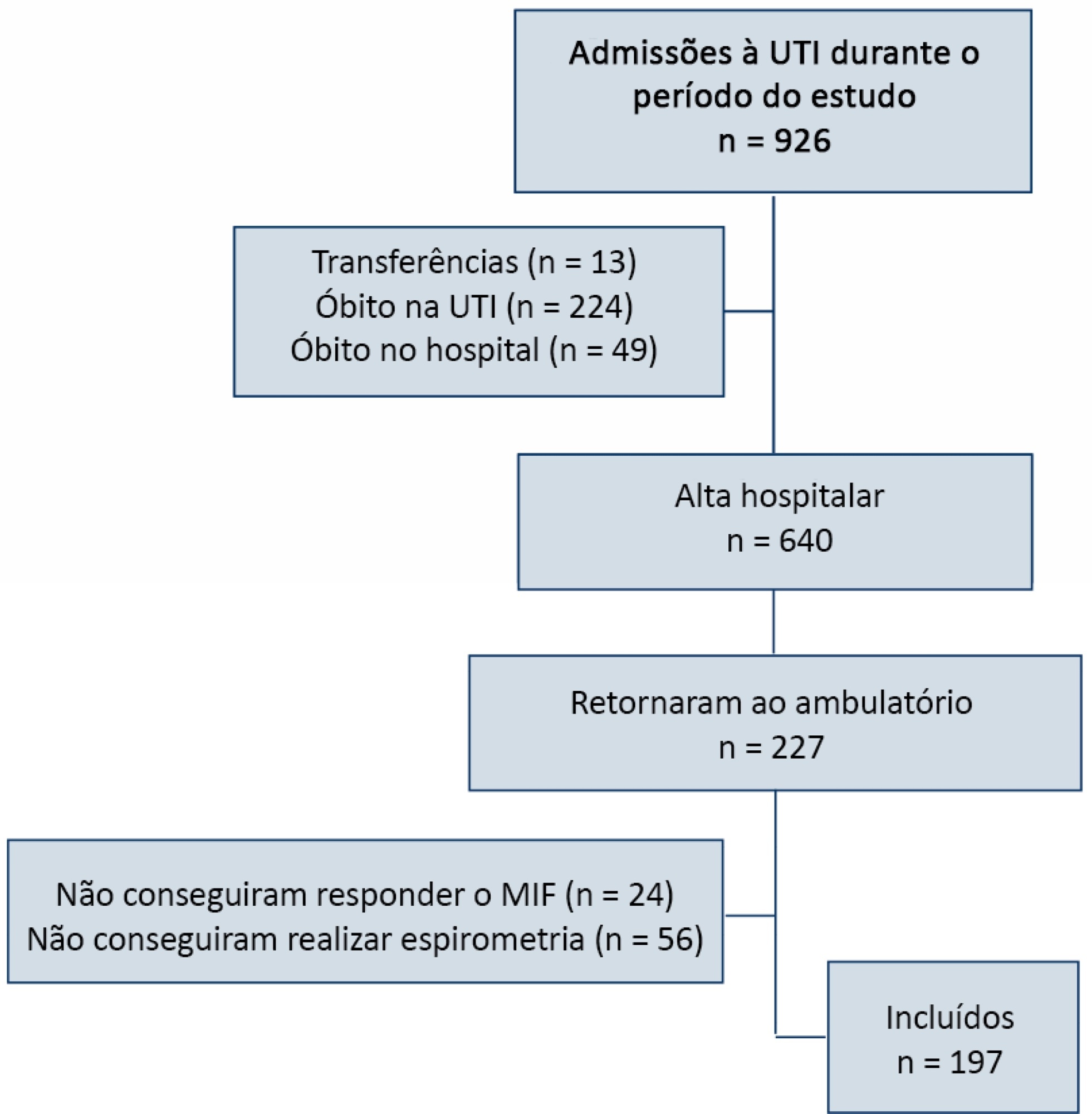
This was a retrospective cohort study conducted in one adult intensive care unit and a multi-professional post-intensive care unit outpatient clinic of a single center. Patients admitted to the intensive care unit from January 2012 to December 2013 who underwent (3 months later) spirometry and answered the Functional Independence Measure Questionnaire were included.
Patients were divided into groups according to the classification of functional independence and spirometry. The study included 197 patients who were divided into greater dependence (n = 4), lower dependence (n = 12) and independent (n = 181) groups. Comparing the three groups, regarding the classification of the Functional Independence Measure, patients with greater dependence had higher Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment values at intensive care unit admission with more advanced age, more days on mechanical ventilation, and longer stay in the intensive care unit and hospital. The majority of patients presented with pulmonary impairment, which was the obstructive pattern observed most frequently. When comparing functional independence with pulmonary function, it was observed that the lower the functional status, the worse the pulmonary function, with a significant difference being observed in peak expiratory flow (p = 0.030).
The majority of patients who returned to the outpatient clinic 3 months after discharge had good functional status but did present with pulmonary impairment, which is related to the degree of functional dependence.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):243-250
DOI 10.5935/0103-507X.20210031
To relate functional independence to the degree of pulmonary impairment in adult patients 3 months after discharge from the intensive care unit.
This was a retrospective cohort study conducted in one adult intensive care unit and a multi-professional post-intensive care unit outpatient clinic of a single center. Patients admitted to the intensive care unit from January 2012 to December 2013 who underwent (3 months later) spirometry and answered the Functional Independence Measure Questionnaire were included.
Patients were divided into groups according to the classification of functional independence and spirometry. The study included 197 patients who were divided into greater dependence (n = 4), lower dependence (n = 12) and independent (n = 181) groups. Comparing the three groups, regarding the classification of the Functional Independence Measure, patients with greater dependence had higher Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment values at intensive care unit admission with more advanced age, more days on mechanical ventilation, and longer stay in the intensive care unit and hospital. The majority of patients presented with pulmonary impairment, which was the obstructive pattern observed most frequently. When comparing functional independence with pulmonary function, it was observed that the lower the functional status, the worse the pulmonary function, with a significant difference being observed in peak expiratory flow (p = 0.030).
The majority of patients who returned to the outpatient clinic 3 months after discharge had good functional status but did present with pulmonary impairment, which is related to the degree of functional dependence.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):261-265
DOI 10.5935/0103-507X.20210033
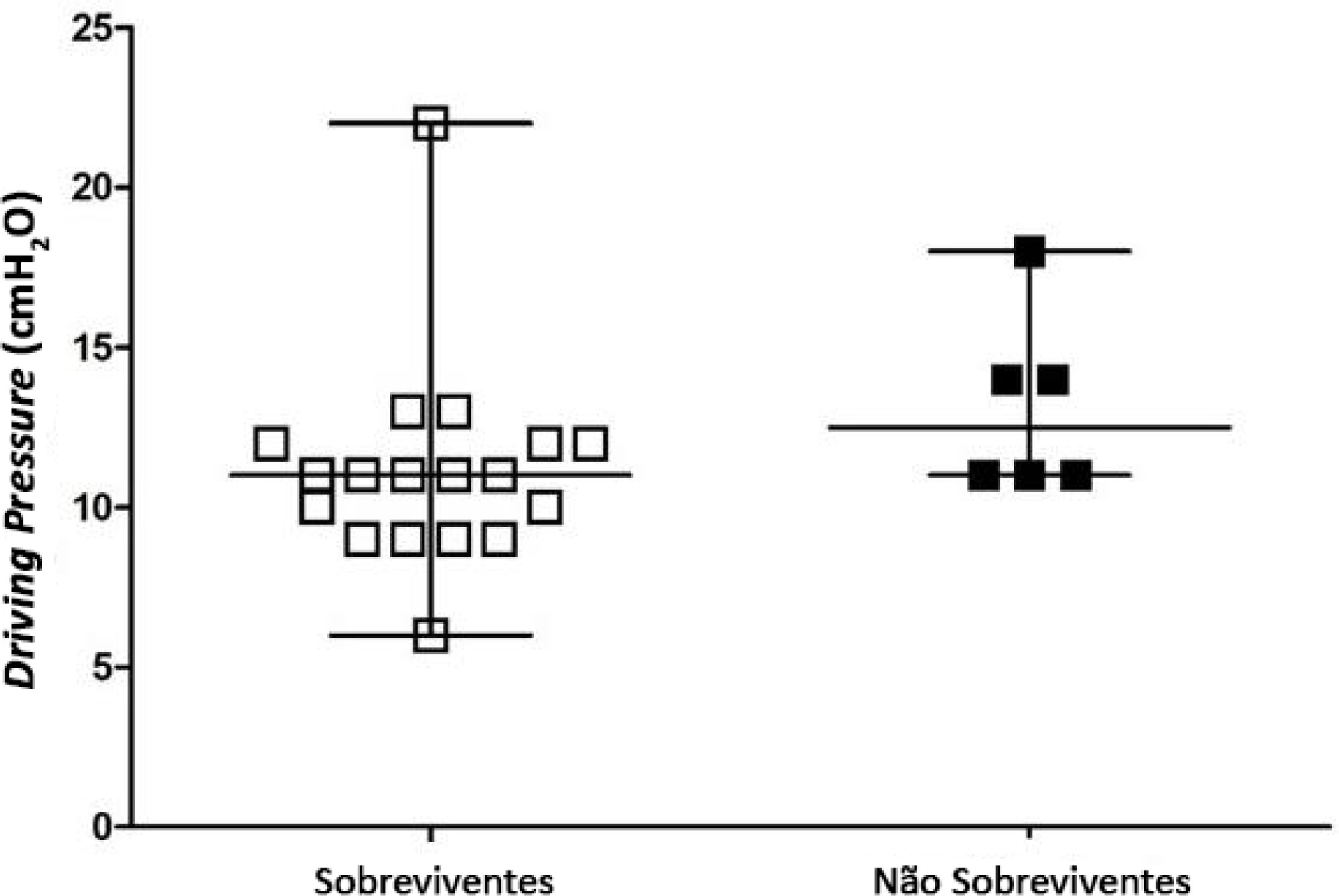
To identify the possible association between driving pressure and mechanical power values and oxygenation index on the first day of mechanical ventilation with the mortality of trauma patients without a diagnosis of acute respiratory distress syndrome.
Patients under pressure-controlled or volume-controlled ventilation were included, with data collection 24 hours after orotracheal intubation. Patient follow-up was performed for 30 days to obtain the clinical outcome. The patients were admitted to two intensive care units of the Hospital de Pronto Socorro de Porto Alegre from June to September 2019.
A total of 24 patients were evaluated. Driving pressure, mechanical power and oxygenation index were similar among patients who survived and those who died, with no statistically significant difference between groups.
Driving pressure, mechanical power and oxygenation index values obtained on the first day of mechanical ventilation were not associated with mortality of trauma patients without acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):261-265
DOI 10.5935/0103-507X.20210033
To identify the possible association between driving pressure and mechanical power values and oxygenation index on the first day of mechanical ventilation with the mortality of trauma patients without a diagnosis of acute respiratory distress syndrome.
Patients under pressure-controlled or volume-controlled ventilation were included, with data collection 24 hours after orotracheal intubation. Patient follow-up was performed for 30 days to obtain the clinical outcome. The patients were admitted to two intensive care units of the Hospital de Pronto Socorro de Porto Alegre from June to September 2019.
A total of 24 patients were evaluated. Driving pressure, mechanical power and oxygenation index were similar among patients who survived and those who died, with no statistically significant difference between groups.
Driving pressure, mechanical power and oxygenation index values obtained on the first day of mechanical ventilation were not associated with mortality of trauma patients without acute respiratory distress syndrome.