Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Cassiano Teixeira"
We found (45) results for your search.Abstract
Rev Bras Ter Intensiva. 2018;30(4):405-413
DOI 10.5935/0103-507X.20180063
To establish the prevalence of physical, cognitive and psychiatric disabilities, associated factors and their relationship with the qualities of life of intensive care survivors in Brazil.
A prospective multicenter cohort study is currently being conducted at 10 adult medical-surgical intensive care units representative of the 5 Brazilian geopolitical regions. Patients aged ≥ 18 years who are discharged from the participating intensive care units and stay 72 hours or more in the intensive care unit for medical or emergency surgery admissions or 120 hours or more for elective surgery admissions are consecutively included. Patients are followed up for a period of one year by means of structured telephone interviews conducted at 3, 6 and 12 months after discharge from the intensive care unit. The outcomes are functional dependence, cognitive dysfunction, anxiety and depression symptoms, posttraumatic stress symptoms, health-related quality of life, rehospitalization and long-term mortality.
The present study has the potential to contribute to current knowledge of the prevalence and factors associated with postintensive care syndrome among adult intensive care survivors in Brazil. In addition, an association might be established between postintensive care syndrome and health-related quality of life.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):405-413
DOI 10.5935/0103-507X.20180063
To establish the prevalence of physical, cognitive and psychiatric disabilities, associated factors and their relationship with the qualities of life of intensive care survivors in Brazil.
A prospective multicenter cohort study is currently being conducted at 10 adult medical-surgical intensive care units representative of the 5 Brazilian geopolitical regions. Patients aged ≥ 18 years who are discharged from the participating intensive care units and stay 72 hours or more in the intensive care unit for medical or emergency surgery admissions or 120 hours or more for elective surgery admissions are consecutively included. Patients are followed up for a period of one year by means of structured telephone interviews conducted at 3, 6 and 12 months after discharge from the intensive care unit. The outcomes are functional dependence, cognitive dysfunction, anxiety and depression symptoms, posttraumatic stress symptoms, health-related quality of life, rehospitalization and long-term mortality.
The present study has the potential to contribute to current knowledge of the prevalence and factors associated with postintensive care syndrome among adult intensive care survivors in Brazil. In addition, an association might be established between postintensive care syndrome and health-related quality of life.

Abstract
Rev Bras Ter Intensiva. 2015;27(4):406-411
DOI 10.5935/0103-507X.20150068
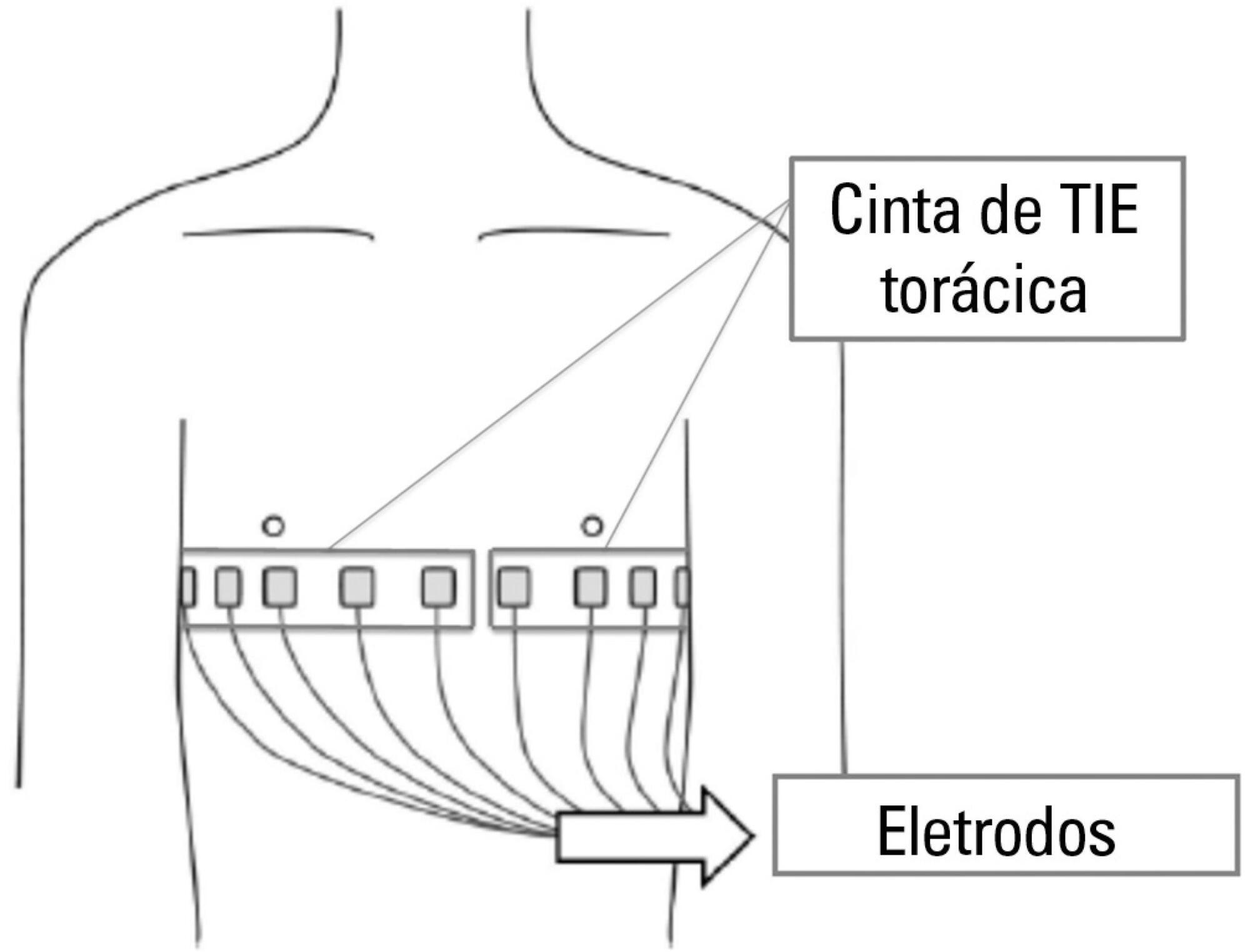
Thoracic electrical impedance tomography is a real-time, noninvasive monitoring tool of the regional pulmonary ventilation distribution. Its bedside use in patients with acute respiratory distress syndrome has the potential to aid in alveolar recruitment maneuvers, which are often necessary in cases of refractory hypoxemia. In this case report, we describe the monitoring results and interpretation of thoracic electrical impedance tomography used during alveolar recruitment maneuvers in a patient with acute respiratory distress syndrome, with transient application of high alveolar pressures and optimal positive end-expiratory pressure titration. Furthermore, we provide a brief literature review regarding the use of alveolar recruitment maneuvers and monitoring using thoracic electrical impedance tomography in patients with acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):406-411
DOI 10.5935/0103-507X.20150068
Thoracic electrical impedance tomography is a real-time, noninvasive monitoring tool of the regional pulmonary ventilation distribution. Its bedside use in patients with acute respiratory distress syndrome has the potential to aid in alveolar recruitment maneuvers, which are often necessary in cases of refractory hypoxemia. In this case report, we describe the monitoring results and interpretation of thoracic electrical impedance tomography used during alveolar recruitment maneuvers in a patient with acute respiratory distress syndrome, with transient application of high alveolar pressures and optimal positive end-expiratory pressure titration. Furthermore, we provide a brief literature review regarding the use of alveolar recruitment maneuvers and monitoring using thoracic electrical impedance tomography in patients with acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):410-425
DOI 10.1590/S0103-507X2011000400005
Brain death (BD) alters the pathophysiology of patients and may damage the kidneys, the lungs, the heart and the liver. To obtain better quality transplant organs, intensive care physicians in charge of the maintenance of deceased donors should attentively monitor these organs. Careful hemodynamic, ventilatory and bronchial clearance management minimizes the loss of kidneys and lungs. The evaluation of cardiac function and morphology supports the transplant viability assessment of the heart. The monitoring of liver function, the management of the patient's metabolic status and the evaluation of viral serology are fundamental for organ selection by the transplant teams and for the care of the transplant recipient
Abstract
Rev Bras Ter Intensiva. 2011;23(4):410-425
DOI 10.1590/S0103-507X2011000400005
Brain death (BD) alters the pathophysiology of patients and may damage the kidneys, the lungs, the heart and the liver. To obtain better quality transplant organs, intensive care physicians in charge of the maintenance of deceased donors should attentively monitor these organs. Careful hemodynamic, ventilatory and bronchial clearance management minimizes the loss of kidneys and lungs. The evaluation of cardiac function and morphology supports the transplant viability assessment of the heart. The monitoring of liver function, the management of the patient's metabolic status and the evaluation of viral serology are fundamental for organ selection by the transplant teams and for the care of the transplant recipient
Abstract
Crit Care Sci. 2023;35(4):421-422
DOI 10.5935/2965-2774.20230202-pt
Abstract
Crit Care Sci. 2023;35(4):421-422
DOI 10.5935/2965-2774.20230202-pt
Abstract
Rev Bras Ter Intensiva. 2019;31(3):425-427
DOI 10.5935/0103-507X.20190046
Abstract
Rev Bras Ter Intensiva. 2019;31(3):425-427
DOI 10.5935/0103-507X.20190046
Abstract
Rev Bras Ter Intensiva. 2022;34(4):492-498
DOI 10.5935/0103-507X.20220169-en
To describe the rate and factors related to nonreturn to work in the third month after discharge from the intensive care unit and the impact of unemployment, loss of income and health care expenses for survivors.
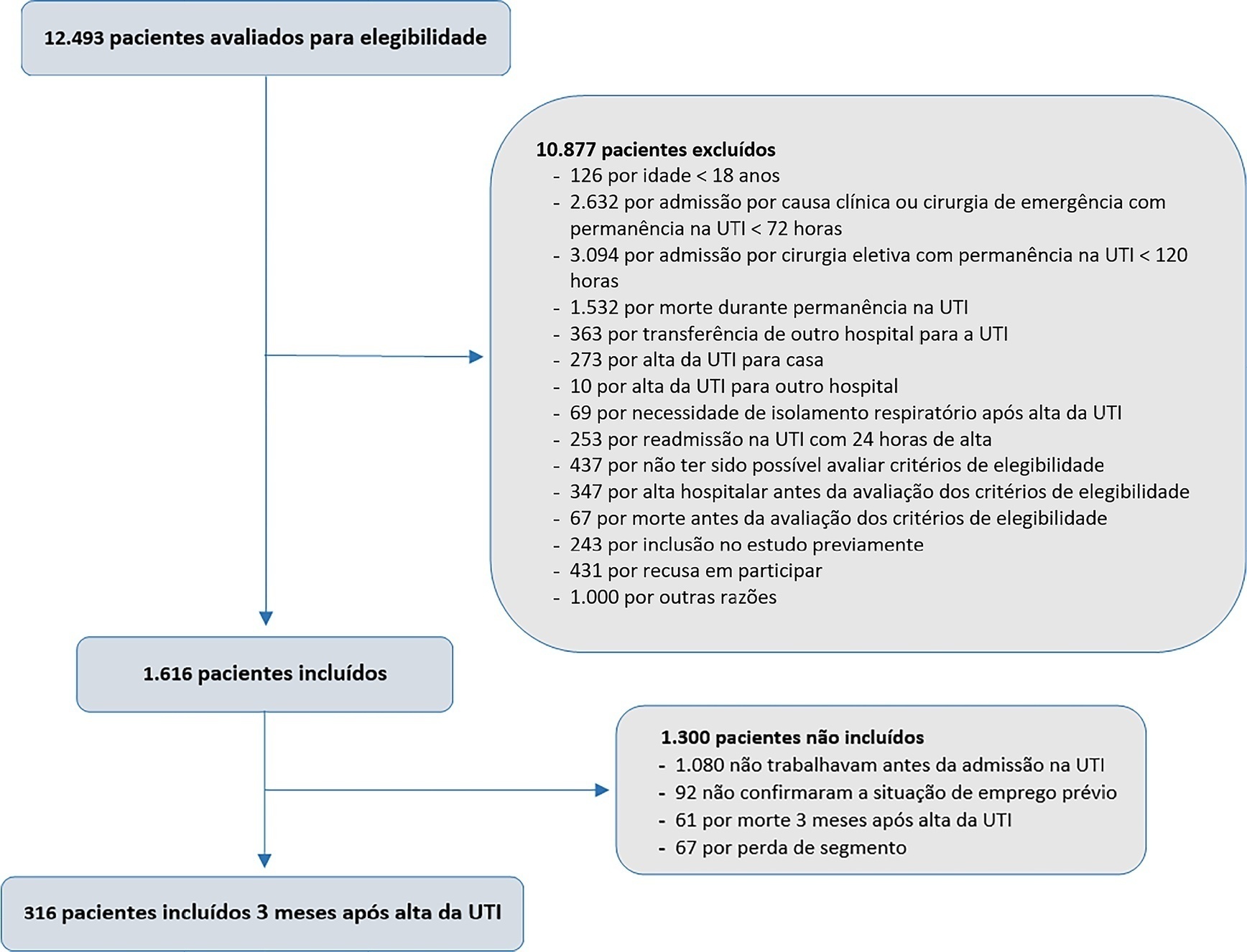
This was a prospective multicenter cohort study that included survivors of severe acute illness who were hospitalized between 2015 and 2018, previously employed, and who stayed more than 72 hours in the intensive care unit. Outcomes were assessed by telephone interview in the third month after discharge.
Of the 316 patients included in the study who had previously worked, 193 (61.1%) did not return to work within 3 months after discharge from the intensive care unit. The following factors were associated with nonreturn to work: low educational level (prevalence ratio 1.39; 95%CI 1.10 - 1.74; p = 0.006), previous employment relationship (prevalence ratio 1.32; 95%CI 1 10 - 1.58; p = 0.003), need for mechanical ventilation (prevalence ratio 1.20; 95%CI 1.01 - 1.42; p = 0.04) and physical dependence in the third month after discharge (prevalence ratio 1.27; 95%CI 1.08 - 1.48; p = 0.003). Survivors who were unable to return to work more often had reduced family income (49.7% versus 33.3%; p = 0.008) and increased health expenditures (66.9% versus 48.3%; p = 0.002). compared to those who returned to work in the third month after discharge from the intensive care unit.
Intensive care unit survivors often do not return to work until the third month after discharge from the intensive care unit. Low educational level, formal job, need for ventilatory support and physical dependence in the third month after discharge were related to nonreturn to work. Failure to return to work was also associated with reduced family income and increased health care costs after discharge.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):492-498
DOI 10.5935/0103-507X.20220169-en
To describe the rate and factors related to nonreturn to work in the third month after discharge from the intensive care unit and the impact of unemployment, loss of income and health care expenses for survivors.
This was a prospective multicenter cohort study that included survivors of severe acute illness who were hospitalized between 2015 and 2018, previously employed, and who stayed more than 72 hours in the intensive care unit. Outcomes were assessed by telephone interview in the third month after discharge.
Of the 316 patients included in the study who had previously worked, 193 (61.1%) did not return to work within 3 months after discharge from the intensive care unit. The following factors were associated with nonreturn to work: low educational level (prevalence ratio 1.39; 95%CI 1.10 - 1.74; p = 0.006), previous employment relationship (prevalence ratio 1.32; 95%CI 1 10 - 1.58; p = 0.003), need for mechanical ventilation (prevalence ratio 1.20; 95%CI 1.01 - 1.42; p = 0.04) and physical dependence in the third month after discharge (prevalence ratio 1.27; 95%CI 1.08 - 1.48; p = 0.003). Survivors who were unable to return to work more often had reduced family income (49.7% versus 33.3%; p = 0.008) and increased health expenditures (66.9% versus 48.3%; p = 0.002). compared to those who returned to work in the third month after discharge from the intensive care unit.
Intensive care unit survivors often do not return to work until the third month after discharge from the intensive care unit. Low educational level, formal job, need for ventilatory support and physical dependence in the third month after discharge were related to nonreturn to work. Failure to return to work was also associated with reduced family income and increased health care costs after discharge.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):497-503
DOI 10.5935/0103-507X.20190087
To evaluate whether electromyographical findings could predict intensive care unit mortality among mechanically ventilated septic patients under profound sedation.
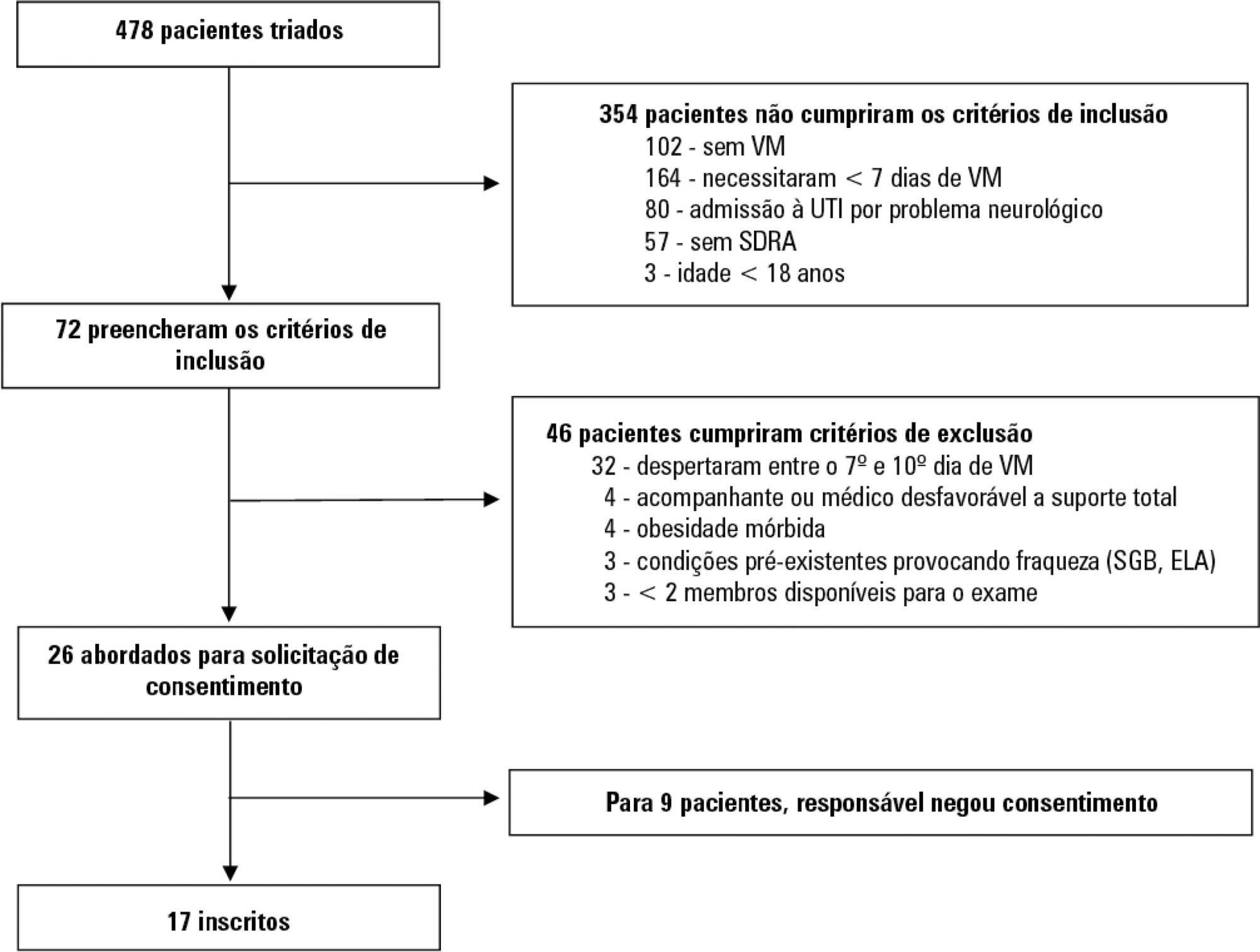
A prospective cohort study that consecutively enrolled moderate-severe acute respiratory distress syndrome (partial pressure of oxygen/fraction of inspired oxygen < 200) patients who were ≥ 18 years of age, dependent on mechanical ventilation for ≥ 7 days, and under profound sedation (Richmond Agitation Sedation Scale ≤ -4) was conducted. Electromyographic studies of the limbs were performed in all patients between the 7th and the 10th day of mechanical ventilation. Sensory nerve action potentials were recorded from the median and sural nerves. The compound muscle action potentials were recorded from the median (abductor pollicis brevis muscle) and common peroneal (extensor digitorum brevis muscle) nerves.
Seventeen patients were enrolled during the seven months of the study. Nine patients (53%) had electromyographic signs of critical illness myopathy or neuropathy. The risk of death during the intensive care unit stay was increased in patients with electromyographical signs of critical illness myopathy or neuropathy in comparison to those without these diagnostics (77.7% versus 12.5%, log-rank p = 0.02).
Electromyographical signs of critical illness myopathy or neuropathy between the 7th and the 10th day of mechanical ventilation may be associated with intensive care unit mortality among moderate-severe acute respiratory distress syndrome patients under profound sedation, in whom clinical strength assessment is not possible.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):497-503
DOI 10.5935/0103-507X.20190087
To evaluate whether electromyographical findings could predict intensive care unit mortality among mechanically ventilated septic patients under profound sedation.
A prospective cohort study that consecutively enrolled moderate-severe acute respiratory distress syndrome (partial pressure of oxygen/fraction of inspired oxygen < 200) patients who were ≥ 18 years of age, dependent on mechanical ventilation for ≥ 7 days, and under profound sedation (Richmond Agitation Sedation Scale ≤ -4) was conducted. Electromyographic studies of the limbs were performed in all patients between the 7th and the 10th day of mechanical ventilation. Sensory nerve action potentials were recorded from the median and sural nerves. The compound muscle action potentials were recorded from the median (abductor pollicis brevis muscle) and common peroneal (extensor digitorum brevis muscle) nerves.
Seventeen patients were enrolled during the seven months of the study. Nine patients (53%) had electromyographic signs of critical illness myopathy or neuropathy. The risk of death during the intensive care unit stay was increased in patients with electromyographical signs of critical illness myopathy or neuropathy in comparison to those without these diagnostics (77.7% versus 12.5%, log-rank p = 0.02).
Electromyographical signs of critical illness myopathy or neuropathy between the 7th and the 10th day of mechanical ventilation may be associated with intensive care unit mortality among moderate-severe acute respiratory distress syndrome patients under profound sedation, in whom clinical strength assessment is not possible.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):555-560
DOI 10.5935/0103-507X.20190074
Patients with acute respiratory distress syndrome require ventilation strategies that have been shown to be important for reducing short-term mortality, such as protective ventilation and prone position ventilation. However, patients who survive have a prolonged stay in both the intensive care unit and the hospital, and they experience a reduction in overall satisfaction with life (independence, acceptance and positive outlook) as well as decreased mental health (including anxiety, depression and posttraumatic stress disorder symptoms), physical health (impaired physical state and activities of daily living; fatigue and muscle weakness), social health and the ability to participate in social activities (including relationships with friends and family, hobbies and social gatherings).
Abstract
Rev Bras Ter Intensiva. 2019;31(4):555-560
DOI 10.5935/0103-507X.20190074
Patients with acute respiratory distress syndrome require ventilation strategies that have been shown to be important for reducing short-term mortality, such as protective ventilation and prone position ventilation. However, patients who survive have a prolonged stay in both the intensive care unit and the hospital, and they experience a reduction in overall satisfaction with life (independence, acceptance and positive outlook) as well as decreased mental health (including anxiety, depression and posttraumatic stress disorder symptoms), physical health (impaired physical state and activities of daily living; fatigue and muscle weakness), social health and the ability to participate in social activities (including relationships with friends and family, hobbies and social gatherings).