Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Márcio Soares"
We found (32) results for your search.Abstract
Rev Bras Ter Intensiva. 2010;22(1):11-18
DOI 10.1590/S0103-507X2010000100004
OBJECTIVE: This study aimed to evaluate the outcome of cirrhotic patients admitted to Intensive Care Unit. METHODS: We conducted a prospective cohort of cirrhotic patients admitted to two intensive care unit between June 1999 to September 2004. We collected demographic, comorbid conditions, diagnosis, vital signs, laboratory data, prognostic scores and evolution in intensive care unit and hospital. The patients were divided in groups: non surgical, non liver surgery, surgery for portal hypertension, liver surgery, liver transplantation, and urgent surgery. RESULTS: We studied 304 patients, which 190 (62.5%) were male. The median of age was 54 (47-61) years. The mortality rate in intensive care unit and hospital were 29.3 and 39.8%, respectively, more elevated than in the other patients admitted critically ill patients (19.6 and 28.3%; p<0.001). Non surgical patients and those submitted to urgent surgery presented high mortality rate in the intensive care unit (64.3 and 65.4%) and in the hospital (80.4 and 76.9%). The variables related to hospital mortality were [Odds ratio (confidence interval 95%)]: mean arterial pressure [0.985 (0.974-0.997)]; mechanical ventilation in the first 24 h [4.080 (1.990-8.364)]; confirmed infection in the first 24 h [7.899 (2.814-22.175)]; acute renal failure [5.509 (1.708-17.766)] and APACHE II score (points) [1.078 (1.017-1.143)]. CONCLUSIONS: Cirrhotic patients had higher mortality rate compared to non cirrhotic critically ill patients. Those admitted after urgent surgery and non surgical had higher mortality rate.
Abstract
Rev Bras Ter Intensiva. 2010;22(1):11-18
DOI 10.1590/S0103-507X2010000100004
OBJECTIVE: This study aimed to evaluate the outcome of cirrhotic patients admitted to Intensive Care Unit. METHODS: We conducted a prospective cohort of cirrhotic patients admitted to two intensive care unit between June 1999 to September 2004. We collected demographic, comorbid conditions, diagnosis, vital signs, laboratory data, prognostic scores and evolution in intensive care unit and hospital. The patients were divided in groups: non surgical, non liver surgery, surgery for portal hypertension, liver surgery, liver transplantation, and urgent surgery. RESULTS: We studied 304 patients, which 190 (62.5%) were male. The median of age was 54 (47-61) years. The mortality rate in intensive care unit and hospital were 29.3 and 39.8%, respectively, more elevated than in the other patients admitted critically ill patients (19.6 and 28.3%; p<0.001). Non surgical patients and those submitted to urgent surgery presented high mortality rate in the intensive care unit (64.3 and 65.4%) and in the hospital (80.4 and 76.9%). The variables related to hospital mortality were [Odds ratio (confidence interval 95%)]: mean arterial pressure [0.985 (0.974-0.997)]; mechanical ventilation in the first 24 h [4.080 (1.990-8.364)]; confirmed infection in the first 24 h [7.899 (2.814-22.175)]; acute renal failure [5.509 (1.708-17.766)] and APACHE II score (points) [1.078 (1.017-1.143)]. CONCLUSIONS: Cirrhotic patients had higher mortality rate compared to non cirrhotic critically ill patients. Those admitted after urgent surgery and non surgical had higher mortality rate.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):114-120
DOI 10.1590/S0103-507X2006000200002
BACKGROUND AND OBJECTIVES: Information on the outcomes of patients who were refused to the ICU is limited. The aims of this study were to compare the clinical characteristics of patients who were admitted with those of patients who were refused to the ICU and to identify clinical parameters associated with triage procedures. METHODS: Observational prospective cohort study. The following data were collected using a standard questionnaire: comorbidities, acute illness, vital status, laboratory data and APACHE II score. The end-points of interest were admission to the ICU and vital status at hospital discharge. RESULTS: A total of 455 patients were studied; 254 (56%) were admitted and 201 (44%) were not. The main reason for the refuse of admission was the lack of ICU beds (82%). Patients who were not admitted had a higher mortality (85% vs. 61%; p < 0.001). In multivariable analysis, the following variables were associated to non-admission [odds ratio, (95% confidence interval)]: metastatic cancer [5.6(1.7-18.7)], arterial systolic pressure < 90 mmHg [5.2(3.0-8.8)], age > 70 years [4.0(2.4-6.5)], hepatic cirrhosis [3.7(1.8-7.6)], and Glasgow coma scale < 5 [3.6(1.9-6.9)]. The variables associated with ICU admission were: mechanical ventilation [0.5(0.3-0.7)] and acute coronary syndromes [0.1(0.03-0.6)]. CONCLUSIONS: Refusal of ICU admission is frequent and generally as a consequence of ICU beds shortage. Patients who were not admitted had a higher mortality. Clinical characteristics associated with the refusal of admission were identified suggesting that they are used in clinical decision-making for ICU triage.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):114-120
DOI 10.1590/S0103-507X2006000200002
BACKGROUND AND OBJECTIVES: Information on the outcomes of patients who were refused to the ICU is limited. The aims of this study were to compare the clinical characteristics of patients who were admitted with those of patients who were refused to the ICU and to identify clinical parameters associated with triage procedures. METHODS: Observational prospective cohort study. The following data were collected using a standard questionnaire: comorbidities, acute illness, vital status, laboratory data and APACHE II score. The end-points of interest were admission to the ICU and vital status at hospital discharge. RESULTS: A total of 455 patients were studied; 254 (56%) were admitted and 201 (44%) were not. The main reason for the refuse of admission was the lack of ICU beds (82%). Patients who were not admitted had a higher mortality (85% vs. 61%; p < 0.001). In multivariable analysis, the following variables were associated to non-admission [odds ratio, (95% confidence interval)]: metastatic cancer [5.6(1.7-18.7)], arterial systolic pressure < 90 mmHg [5.2(3.0-8.8)], age > 70 years [4.0(2.4-6.5)], hepatic cirrhosis [3.7(1.8-7.6)], and Glasgow coma scale < 5 [3.6(1.9-6.9)]. The variables associated with ICU admission were: mechanical ventilation [0.5(0.3-0.7)] and acute coronary syndromes [0.1(0.03-0.6)]. CONCLUSIONS: Refusal of ICU admission is frequent and generally as a consequence of ICU beds shortage. Patients who were not admitted had a higher mortality. Clinical characteristics associated with the refusal of admission were identified suggesting that they are used in clinical decision-making for ICU triage.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):115-123
DOI 10.1590/S0103-507X2008000200001
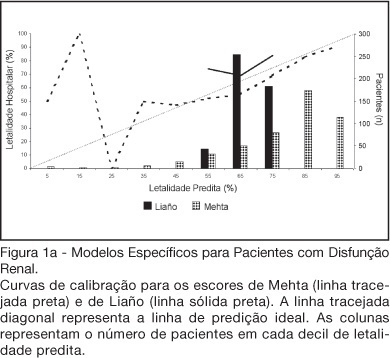
BACKGROUND AND OBJECTIVES: There is no consensus about prognostic scores for use in patients with acute kidney injury (AKI). The aim of this study was to evaluate the performance of six prognostic scores in predicting hospital mortality in patients with AKI and need for renal replacement therapy (RRT). METHODS: Prospective cohort of patients admitted to the intensive care units (ICU) of three tertiary care hospitals that required RRT for AKI over a 32-month period. Patients with end-stage renal disease and those with ICU stay < 24h were excluded. Data from the first 24h of ICU admission were used to calculate SAPS II and APACHE II scores, and data from the first 24h of RRT were used in the calculation of LOD, ODIN, Liaño and Mehta scores. Discrimination was evaluated using the area under ROC curve (AUROC) and calibration using the Hosmer-Lemeshow goodness-of-fit test. The hospital mortality was the end-point of interest. RESULTS: 467 patients were evaluated. Hospital mortality rate was 75%. Mean SAPS II and APACHE II scores were 48.5 ±11.2 and 27.4 ± 6.3 points, and median LOD score was 7 (5-8) points. Except for Mehta score (p = 0.001), calibration was appropriate in all models. However, discrimination was uniformly unsatisfactory; AUROC ranged from 0.60 for ODIN to 0.72 for SAPS II and Mehta scores. In addition, except for Mehta, all models tended to underestimate hospital mortality. CONCLUSIONS: Organ dysfunction, general and renal-specific severity-of-illness scores were inaccurate in predicting outcome in ICU patients in need for RRT.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):115-123
DOI 10.1590/S0103-507X2008000200001
BACKGROUND AND OBJECTIVES: There is no consensus about prognostic scores for use in patients with acute kidney injury (AKI). The aim of this study was to evaluate the performance of six prognostic scores in predicting hospital mortality in patients with AKI and need for renal replacement therapy (RRT). METHODS: Prospective cohort of patients admitted to the intensive care units (ICU) of three tertiary care hospitals that required RRT for AKI over a 32-month period. Patients with end-stage renal disease and those with ICU stay < 24h were excluded. Data from the first 24h of ICU admission were used to calculate SAPS II and APACHE II scores, and data from the first 24h of RRT were used in the calculation of LOD, ODIN, Liaño and Mehta scores. Discrimination was evaluated using the area under ROC curve (AUROC) and calibration using the Hosmer-Lemeshow goodness-of-fit test. The hospital mortality was the end-point of interest. RESULTS: 467 patients were evaluated. Hospital mortality rate was 75%. Mean SAPS II and APACHE II scores were 48.5 ±11.2 and 27.4 ± 6.3 points, and median LOD score was 7 (5-8) points. Except for Mehta score (p = 0.001), calibration was appropriate in all models. However, discrimination was uniformly unsatisfactory; AUROC ranged from 0.60 for ODIN to 0.72 for SAPS II and Mehta scores. In addition, except for Mehta, all models tended to underestimate hospital mortality. CONCLUSIONS: Organ dysfunction, general and renal-specific severity-of-illness scores were inaccurate in predicting outcome in ICU patients in need for RRT.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):170-177
DOI 10.5935/0103-507X.20150029
The aim of this study was to investigate whether plasma serotonin levels or acetylcholinesterase activities determined upon intensive care unit admission could predict the occurrence of acute brain dysfunction in intensive care unit patients.
A prospective cohort study was conducted with a sample of 77 non-consecutive patients observed between May 2009 and September 2010. Delirium was determined using the Confusion Assessment Method for the Intensive Care Unit tool, and the acetylcholinesterase and serotonin measurements were determined from blood samples collected up to a maximum of 24 h after the admission of the patient to the intensive care unit.
In the present study, 38 (49.6%) patients developed delirium during their intensive care unit stays. Neither serum acetylcholinesterase activity nor serotonin level was independently associated with delirium. No significant correlations of acetylcholinesterase activity or serotonin level with delirium/coma-free days were observed, but in the patients who developed delirium, there was a strong negative correlation between the acetylcholinesterase level and the number of delirium/coma-free days, indicating that higher acetylcholinesterase levels are associated with fewer days alive without delirium or coma. No associations were found between the biomarkers and mortality.
Neither serum acetylcholinesterase activity nor serotonin level was associated with delirium or acute brain dysfunction in critically ill patients. Sepsis did not modify these relationships.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):170-177
DOI 10.5935/0103-507X.20150029
The aim of this study was to investigate whether plasma serotonin levels or acetylcholinesterase activities determined upon intensive care unit admission could predict the occurrence of acute brain dysfunction in intensive care unit patients.
A prospective cohort study was conducted with a sample of 77 non-consecutive patients observed between May 2009 and September 2010. Delirium was determined using the Confusion Assessment Method for the Intensive Care Unit tool, and the acetylcholinesterase and serotonin measurements were determined from blood samples collected up to a maximum of 24 h after the admission of the patient to the intensive care unit.
In the present study, 38 (49.6%) patients developed delirium during their intensive care unit stays. Neither serum acetylcholinesterase activity nor serotonin level was independently associated with delirium. No significant correlations of acetylcholinesterase activity or serotonin level with delirium/coma-free days were observed, but in the patients who developed delirium, there was a strong negative correlation between the acetylcholinesterase level and the number of delirium/coma-free days, indicating that higher acetylcholinesterase levels are associated with fewer days alive without delirium or coma. No associations were found between the biomarkers and mortality.
Neither serum acetylcholinesterase activity nor serotonin level was associated with delirium or acute brain dysfunction in critically ill patients. Sepsis did not modify these relationships.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):173-177
DOI 10.1590/S0103-507X2008000200010
BACKGROUND AND OBJECTIVES: The debate on efficacy and patient safety related to the use of drotrecogin alfa (DrotAA) is timely, principally due to the negative results observed in clinical studies performed after the PROWESS study, and the economic cost-related impact of the drug on the healthcare system. The aim of this study was to review the main studies on the use of DrotAA in patients with severe sepsis. The focus was on drug efficacy-and patient safety-related issues. CONTENTS: Articles were selected by a MedLine search for studies on the use of DrotAA in patients with sepsis using the following key words: activated protein C; drotrecogin alfa; sepsis; septic shock; Xigris®. Additional references were retrieved from the studies initially selected. CONCLUSIONS: Mortality and bleeding complications associated with the use of DrotAA were more frequent in large observational studies than those reported in randomized trials. In the light of the current knowledge, routine use of DrotAA should be reevaluated until well-designed confirmatory clinical trials can clarify the true efficacy and safety of the drug and help identify the subgroup of patients that can benefit from use of DrotAA. Physicians should be cautious with the rapid transfer of evidences not well-documented, to the guidelines and recommendations practiced in the care and treatment of patients with severe sepsis.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):173-177
DOI 10.1590/S0103-507X2008000200010
BACKGROUND AND OBJECTIVES: The debate on efficacy and patient safety related to the use of drotrecogin alfa (DrotAA) is timely, principally due to the negative results observed in clinical studies performed after the PROWESS study, and the economic cost-related impact of the drug on the healthcare system. The aim of this study was to review the main studies on the use of DrotAA in patients with severe sepsis. The focus was on drug efficacy-and patient safety-related issues. CONTENTS: Articles were selected by a MedLine search for studies on the use of DrotAA in patients with sepsis using the following key words: activated protein C; drotrecogin alfa; sepsis; septic shock; Xigris®. Additional references were retrieved from the studies initially selected. CONCLUSIONS: Mortality and bleeding complications associated with the use of DrotAA were more frequent in large observational studies than those reported in randomized trials. In the light of the current knowledge, routine use of DrotAA should be reevaluated until well-designed confirmatory clinical trials can clarify the true efficacy and safety of the drug and help identify the subgroup of patients that can benefit from use of DrotAA. Physicians should be cautious with the rapid transfer of evidences not well-documented, to the guidelines and recommendations practiced in the care and treatment of patients with severe sepsis.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):176-182
DOI 10.5935/0103-507X.20140026
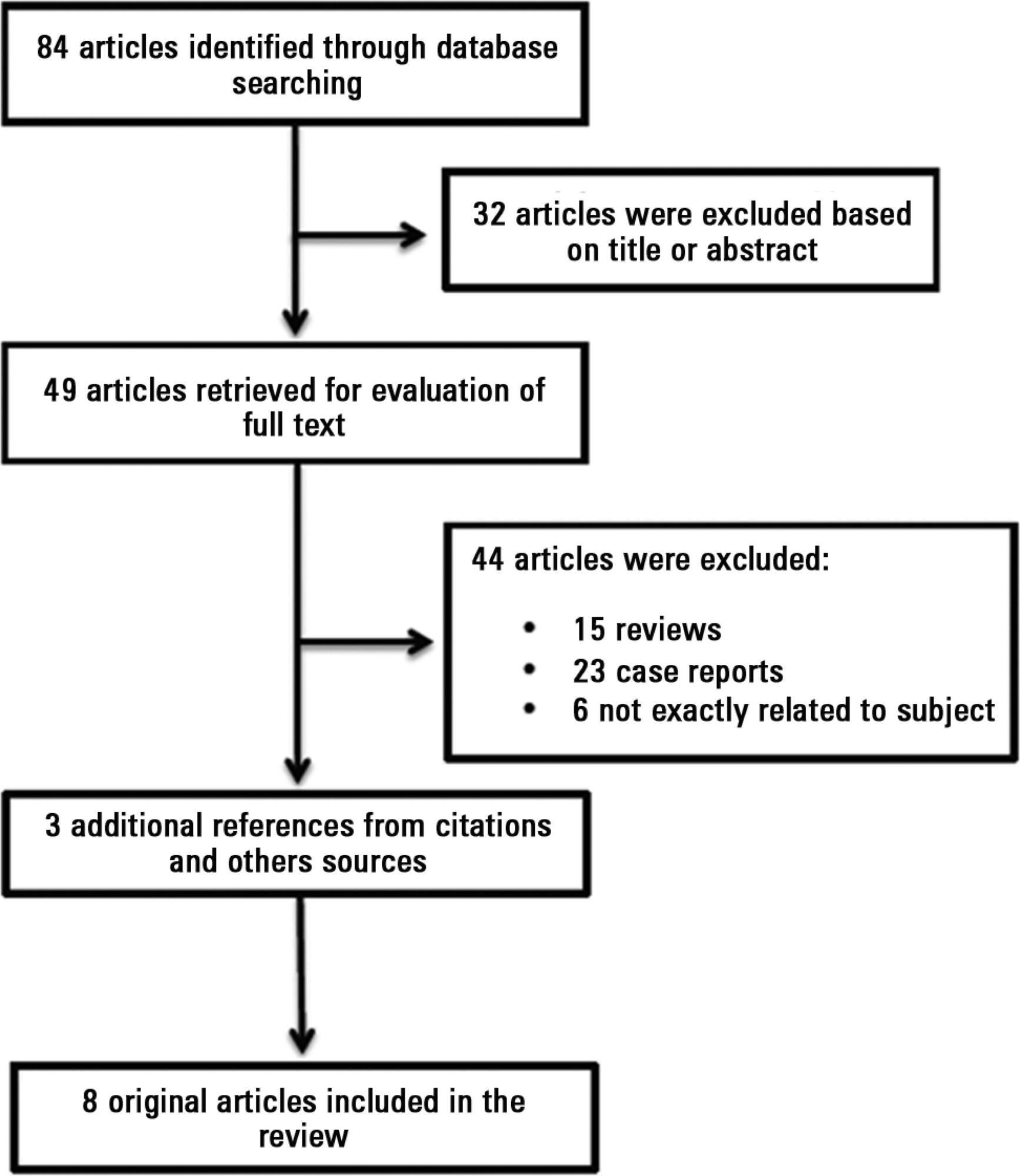
Antiphospholipid antibodies are responsible for a wide spectrum of clinical manifestations. Venous, arterial and microvascular thrombosis and severe catastrophic cases account for a large morbidly/mortality. Through the connection between the immune, inflammatory and hemostatic systems, it is possible that these antibodies may contribute to the development of organ dysfunction and are associated with poor short and long-term prognoses in critically ill patients. We performed a search of the PubMed/MedLine database for articles written during the period from January 2000 to February 2013 to evaluate the frequency of antiphospholipid antibodies in critically ill patients and their impact on the outcomes of these patients. Only eight original studies involving critically ill patients were found. However, the development of antiphospholipid antibodies in critically ill patients seems to be frequent, but more studies are necessary to clarify their pathogenic role and implications for clinical practice.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):176-182
DOI 10.5935/0103-507X.20140026
Antiphospholipid antibodies are responsible for a wide spectrum of clinical manifestations. Venous, arterial and microvascular thrombosis and severe catastrophic cases account for a large morbidly/mortality. Through the connection between the immune, inflammatory and hemostatic systems, it is possible that these antibodies may contribute to the development of organ dysfunction and are associated with poor short and long-term prognoses in critically ill patients. We performed a search of the PubMed/MedLine database for articles written during the period from January 2000 to February 2013 to evaluate the frequency of antiphospholipid antibodies in critically ill patients and their impact on the outcomes of these patients. Only eight original studies involving critically ill patients were found. However, the development of antiphospholipid antibodies in critically ill patients seems to be frequent, but more studies are necessary to clarify their pathogenic role and implications for clinical practice.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):186-191
DOI 10.1590/S0103-507X2007000200008
BACKGROUND AND OBJECTIVES: The adverse effects of intra-abdominal hypertension are known for many years. Only recently proper attention has been given to routine intra-abdominal pressure (IAP) monitoring. There is evidence that a quarter of intensive care units (ICU) do not measure IAP, due to a lack of knowledge of its importance or difficulty in results interpretation. The aim of this study is investigate the knowledge of ICU physicians about abdominal compartimental syndrome and its management. METHODS: A questionnaire with 12 questions about this issue was mailed to ICU physicians. RESULTS: The current knowledge of the international definitions of ACS does not seem to be linked to the number of years of medical practice, but was associated with the time spent working on intensive care. Although most physicians are aware of the existence of ACS, less than half know the present international definitions. The IAP monitoring is performed in patients at risk for ACS, by means of the intravesical filling with 25 to 100 mL of liquids, in intervals varying from of 4 to 8 hours. There was no consensus on the value of IAP values (with or without organ dysfunctions) for the clinical or surgical treatments of ACS in this survey. CONCLUSIONS: The knowledge of ACS is satisfactory when we consider only physicians that devote most of their time to ICU work. However, it is necessary to improve education and knowledge of most intensive care physicians regarding the presence and severity of intra-abdominal hypertension in Rio de Janeiro.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):186-191
DOI 10.1590/S0103-507X2007000200008
BACKGROUND AND OBJECTIVES: The adverse effects of intra-abdominal hypertension are known for many years. Only recently proper attention has been given to routine intra-abdominal pressure (IAP) monitoring. There is evidence that a quarter of intensive care units (ICU) do not measure IAP, due to a lack of knowledge of its importance or difficulty in results interpretation. The aim of this study is investigate the knowledge of ICU physicians about abdominal compartimental syndrome and its management. METHODS: A questionnaire with 12 questions about this issue was mailed to ICU physicians. RESULTS: The current knowledge of the international definitions of ACS does not seem to be linked to the number of years of medical practice, but was associated with the time spent working on intensive care. Although most physicians are aware of the existence of ACS, less than half know the present international definitions. The IAP monitoring is performed in patients at risk for ACS, by means of the intravesical filling with 25 to 100 mL of liquids, in intervals varying from of 4 to 8 hours. There was no consensus on the value of IAP values (with or without organ dysfunctions) for the clinical or surgical treatments of ACS in this survey. CONCLUSIONS: The knowledge of ACS is satisfactory when we consider only physicians that devote most of their time to ICU work. However, it is necessary to improve education and knowledge of most intensive care physicians regarding the presence and severity of intra-abdominal hypertension in Rio de Janeiro.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):193-195
DOI 10.5935/0103-507X.20150040
Abstract
Rev Bras Ter Intensiva. 2015;27(3):193-195
DOI 10.5935/0103-507X.20150040