
You searched for:"Reinaldo Salomão"
We found (6) results for your search.-
Original Article
Availability of resources to treat sepsis in Brazil: a random sample of Brazilian institutions
Rev Bras Ter Intensiva. 2019;31(2):193-201
Abstract
Original ArticleAvailability of resources to treat sepsis in Brazil: a random sample of Brazilian institutions
Rev Bras Ter Intensiva. 2019;31(2):193-201
DOI 10.5935/0103-507X.20190033
Views1ABSTRACT
Objective:
To characterize resource availability from a nationally representative random sample of intensive care units in Brazil.
Methods:
A structured online survey of participating units in the Sepsis PREvalence Assessment Database (SPREAD) study, a nationwide 1-day point prevalence survey to assess the burden of sepsis in Brazil, was sent to the medical director of each unit.
Results:
A representative sample of 277 of the 317 invited units responded to the resources survey. Most of the hospitals had fewer than 500 beds (94.6%) with a median of 14 beds in the intensive care unit. Providing care for public-insured patients was the main source of income in two-thirds of the surveyed units. Own microbiology laboratory was not available for 26.8% of the surveyed intensive care units, and 10.5% did not always have access to blood cultures. Broad spectrum antibiotics were not always available in 10.5% of surveyed units, and 21.3% could not always measure lactate within three hours. Those institutions with a high resource availability (158 units, 57%) were usually larger and preferentially served patients from the private health system compared to institutions without high resource availability. Otherwise, those without high resource availability did not always have broad-spectrum antibiotics (24.4%), vasopressors (4.2%) or crystalloids (7.6%).
Conclusion:
Our study indicates that a relevant number of units cannot perform basic monitoring and therapeutic interventions in septic patients. Our results highlight major opportunities for improvement to adhere to simple but effective interventions in Brazil.
Keywords:Brazil/epidemiologyCritical careDeveloping countriesEpidemiological monitoringHealth resourcesIntensive care unitsSepsis/epidemiologyTherapeuticsSee moreViews1

Abstract
Original ArticleAvailability of resources to treat sepsis in Brazil: a random sample of Brazilian institutions
Rev Bras Ter Intensiva. 2019;31(2):193-201
DOI 10.5935/0103-507X.20190033
Views1ABSTRACT
Objective:
To characterize resource availability from a nationally representative random sample of intensive care units in Brazil.
Methods:
A structured online survey of participating units in the Sepsis PREvalence Assessment Database (SPREAD) study, a nationwide 1-day point prevalence survey to assess the burden of sepsis in Brazil, was sent to the medical director of each unit.
Results:
A representative sample of 277 of the 317 invited units responded to the resources survey. Most of the hospitals had fewer than 500 beds (94.6%) with a median of 14 beds in the intensive care unit. Providing care for public-insured patients was the main source of income in two-thirds of the surveyed units. Own microbiology laboratory was not available for 26.8% of the surveyed intensive care units, and 10.5% did not always have access to blood cultures. Broad spectrum antibiotics were not always available in 10.5% of surveyed units, and 21.3% could not always measure lactate within three hours. Those institutions with a high resource availability (158 units, 57%) were usually larger and preferentially served patients from the private health system compared to institutions without high resource availability. Otherwise, those without high resource availability did not always have broad-spectrum antibiotics (24.4%), vasopressors (4.2%) or crystalloids (7.6%).
Conclusion:
Our study indicates that a relevant number of units cannot perform basic monitoring and therapeutic interventions in septic patients. Our results highlight major opportunities for improvement to adhere to simple but effective interventions in Brazil.
Keywords:Brazil/epidemiologyCritical careDeveloping countriesEpidemiological monitoringHealth resourcesIntensive care unitsSepsis/epidemiologyTherapeuticsSee more -
Original Articles – Basic Research
Association between organ dysfunction and cytokine concentrations during the early phases of septic shock
Rev Bras Ter Intensiva. 2011;23(4):426-433
Abstract
Original Articles – Basic ResearchAssociation between organ dysfunction and cytokine concentrations during the early phases of septic shock
Rev Bras Ter Intensiva. 2011;23(4):426-433
DOI 10.1590/S0103-507X2011000400006
Views1OBJECTIVE: To investigate the correlation of organ dysfunction and its progression with inflammatory response during the early phases of septic shock by assessing baseline cytokine concentrations. METHODS: This study included patients over 18 years old with septic shock within the first 48 hours after the onset of organ dysfunction. Interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10) and C-reactive protein levels were assessed at inclusion and after 24 hours, and the differences between these values were calculated. The progression of organ dysfunction was assessed using the Sequential Organ Failure Assessment (SOFA) score upon admission and 24 hours later for a delta-SOFA determination and were categorized as either worsened or improved. The results were expressed as means + standard deviation or median (25-75% percentiles). Values with descriptive p values of 0.05 or less were considered significant. RESULTS: Overall, we included 41 patients with median SOFA scores of 8.0 (6.5-10.0) upon admission (T0) and 8.0 (6.0-10.0) 24 hours later (T1). Worsened, improved or unchanged SOFA scores were observed in 11 (Group 1), 17 (Group 2) and 13 (Group 3) patients, respectively. For Group 1, the baseline IL-6, IL-8 and IL-10 values were higher, and a significant increase of IL-8 levels was found after 24 hours. The change in the SOFA score after 24 hours was significantly, although weakly, correlated with baseline IL-6 and IL-8 concentrations. CONCLUSIONS: Higher baseline IL-6, IL-8 and IL-10 levels are associated with unfavorable organ dysfunction outcomes. Increased IL-8 levels within the first 24 hours are correlated with a worsening dysfunction.
Keywords:CytokinesetiologyMultiple organ failureShock, septicsystemic inflammatory response syndromeSee moreViews1Abstract
Original Articles – Basic ResearchAssociation between organ dysfunction and cytokine concentrations during the early phases of septic shock
Rev Bras Ter Intensiva. 2011;23(4):426-433
DOI 10.1590/S0103-507X2011000400006
Views1OBJECTIVE: To investigate the correlation of organ dysfunction and its progression with inflammatory response during the early phases of septic shock by assessing baseline cytokine concentrations. METHODS: This study included patients over 18 years old with septic shock within the first 48 hours after the onset of organ dysfunction. Interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10) and C-reactive protein levels were assessed at inclusion and after 24 hours, and the differences between these values were calculated. The progression of organ dysfunction was assessed using the Sequential Organ Failure Assessment (SOFA) score upon admission and 24 hours later for a delta-SOFA determination and were categorized as either worsened or improved. The results were expressed as means + standard deviation or median (25-75% percentiles). Values with descriptive p values of 0.05 or less were considered significant. RESULTS: Overall, we included 41 patients with median SOFA scores of 8.0 (6.5-10.0) upon admission (T0) and 8.0 (6.0-10.0) 24 hours later (T1). Worsened, improved or unchanged SOFA scores were observed in 11 (Group 1), 17 (Group 2) and 13 (Group 3) patients, respectively. For Group 1, the baseline IL-6, IL-8 and IL-10 values were higher, and a significant increase of IL-8 levels was found after 24 hours. The change in the SOFA score after 24 hours was significantly, although weakly, correlated with baseline IL-6 and IL-8 concentrations. CONCLUSIONS: Higher baseline IL-6, IL-8 and IL-10 levels are associated with unfavorable organ dysfunction outcomes. Increased IL-8 levels within the first 24 hours are correlated with a worsening dysfunction.
Keywords:CytokinesetiologyMultiple organ failureShock, septicsystemic inflammatory response syndromeSee more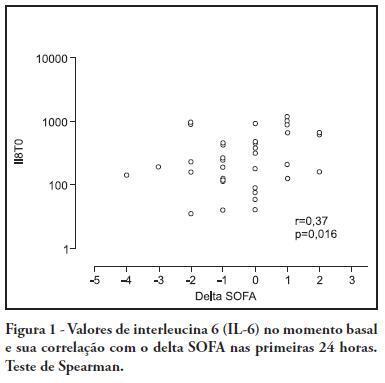
-
Guidelines for the treatment of severe sepsis and septic shock: management of the infectious agent – diagnosis
Rev Bras Ter Intensiva. 2011;23(2):134-144
Abstract
Guidelines for the treatment of severe sepsis and septic shock: management of the infectious agent – diagnosis
Rev Bras Ter Intensiva. 2011;23(2):134-144
DOI 10.1590/S0103-507X2011000200005
Views1See moreSepsis is a common and lethal condition that carries a substantial financial burden and is the primary cause of death in intensive care units. Early diagnosis and treatment of patients has been clearly shown to improve prognosis. Therefore, early diagnosis of infections and control of the primary infection site are fundamental to improving patients’ prognosis. This guideline reviews the available evidence concerning the primary strategies for the diagnosis of infection
Views1Abstract
Guidelines for the treatment of severe sepsis and septic shock: management of the infectious agent – diagnosis
Rev Bras Ter Intensiva. 2011;23(2):134-144
DOI 10.1590/S0103-507X2011000200005
Views1See moreSepsis is a common and lethal condition that carries a substantial financial burden and is the primary cause of death in intensive care units. Early diagnosis and treatment of patients has been clearly shown to improve prognosis. Therefore, early diagnosis of infections and control of the primary infection site are fundamental to improving patients’ prognosis. This guideline reviews the available evidence concerning the primary strategies for the diagnosis of infection
-
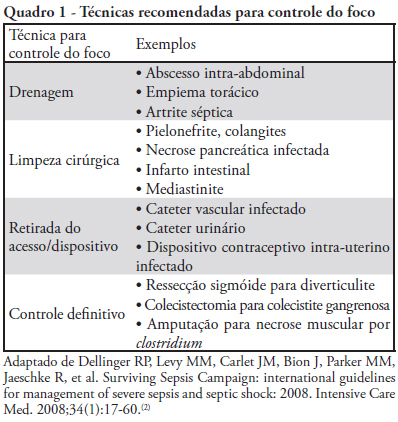
Guidelines for the treatment of severe sepsis and septic shock – management of the infectious agent – source control and antimicrobial treatment
Rev Bras Ter Intensiva. 2011;23(2):145-157
Abstract
Guidelines for the treatment of severe sepsis and septic shock – management of the infectious agent – source control and antimicrobial treatment
Rev Bras Ter Intensiva. 2011;23(2):145-157
DOI 10.1590/S0103-507X2011000200006
Views0See moreSepsis is a common and lethal condition that carries a substantial financial burden. In addition, it is the main cause of death in intensive care units. Early diagnosis and treatment of patients has been clearly shown to improve prognosis. Therefore, early diagnosis of the infecting agent, control of the primary infection site and the use of appropriate antibiotic therapy are fundamental to improving outcomes. This guideline reviews the available evidence in the literature concerning infection control and therapy strategies
Views0Abstract
Guidelines for the treatment of severe sepsis and septic shock – management of the infectious agent – source control and antimicrobial treatment
Rev Bras Ter Intensiva. 2011;23(2):145-157
DOI 10.1590/S0103-507X2011000200006
Views0See moreSepsis is a common and lethal condition that carries a substantial financial burden. In addition, it is the main cause of death in intensive care units. Early diagnosis and treatment of patients has been clearly shown to improve prognosis. Therefore, early diagnosis of the infecting agent, control of the primary infection site and the use of appropriate antibiotic therapy are fundamental to improving outcomes. This guideline reviews the available evidence in the literature concerning infection control and therapy strategies
-
Guidelines for treatment of severe sepsis/septic shock: tissue perfusion assessment
Rev Bras Ter Intensiva. 2011;23(1):6-12
Abstract
Guidelines for treatment of severe sepsis/septic shock: tissue perfusion assessment
Rev Bras Ter Intensiva. 2011;23(1):6-12
DOI 10.1590/S0103-507X2011000100003
Views0See moreSepsis is a very frequent condition and causes high mortality rates and healthcare costs; it is the main cause of death in intensive care units. Clear, improved prognosis was shown for early diagnosed and treated patients. Treatment guidelines are fundamental for appropriate therapy. It is clear that hypoperfusion patients should be hemodynamically optimized; therefore, recognition of hypoperfusion signs is one of the main therapeutic steps. This guideline discusses the current literature and available data regarding the evaluation of hemodynamic parameters.
Views0Abstract
Guidelines for treatment of severe sepsis/septic shock: tissue perfusion assessment
Rev Bras Ter Intensiva. 2011;23(1):6-12
DOI 10.1590/S0103-507X2011000100003
Views0See moreSepsis is a very frequent condition and causes high mortality rates and healthcare costs; it is the main cause of death in intensive care units. Clear, improved prognosis was shown for early diagnosed and treated patients. Treatment guidelines are fundamental for appropriate therapy. It is clear that hypoperfusion patients should be hemodynamically optimized; therefore, recognition of hypoperfusion signs is one of the main therapeutic steps. This guideline discusses the current literature and available data regarding the evaluation of hemodynamic parameters.
-
Guidelines for the treatment of severe sepsis and septic shock: hemodynamic resuscitation
Rev Bras Ter Intensiva. 2011;23(1):13-23
Abstract
Guidelines for the treatment of severe sepsis and septic shock: hemodynamic resuscitation
Rev Bras Ter Intensiva. 2011;23(1):13-23
DOI 10.1590/S0103-507X2011000100004
Views0See moreSepsis has a high incidence, mortality and cost and is the main cause of death in intensive care units. Early recognition and treatment have been clearly associated with a better prognosis. Establishing new guidelines is a fundamental step for improving treatment. Patients with clear signs of hypoperfusion should undergo hemodynamic optimization. This guideline addresses the main strategies in the literature that are clinically available.
Views0Abstract
Guidelines for the treatment of severe sepsis and septic shock: hemodynamic resuscitation
Rev Bras Ter Intensiva. 2011;23(1):13-23
DOI 10.1590/S0103-507X2011000100004
Views0See moreSepsis has a high incidence, mortality and cost and is the main cause of death in intensive care units. Early recognition and treatment have been clearly associated with a better prognosis. Establishing new guidelines is a fundamental step for improving treatment. Patients with clear signs of hypoperfusion should undergo hemodynamic optimization. This guideline addresses the main strategies in the literature that are clinically available.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis