
You searched for:"Alejandro Bruhn"
We found (5) results for your search.-
Editorial
Challenges and limitations of using ventilator-free days as an outcome in critical care trials
Crit Care Sci. 2024;36:e20240088en
Abstract
EditorialChallenges and limitations of using ventilator-free days as an outcome in critical care trials
Crit Care Sci. 2024;36:e20240088en
DOI 10.62675/2965-2774.20240088-en
Views25The use of ventilator-free days (VFDs) as an outcome measure is increasingly popular in critical care research.(-) This composite outcome simultaneously reflects patient survival and the time not spent on mechanical ventilation (MV) within a specified timeframe, which usually extends from randomization up to Day 28. For patients who do not survive this period, VFDs […]See moreViews25

Abstract
EditorialChallenges and limitations of using ventilator-free days as an outcome in critical care trials
Crit Care Sci. 2024;36:e20240088en
DOI 10.62675/2965-2774.20240088-en
Views25The use of ventilator-free days (VFDs) as an outcome measure is increasingly popular in critical care research.(-) This composite outcome simultaneously reflects patient survival and the time not spent on mechanical ventilation (MV) within a specified timeframe, which usually extends from randomization up to Day 28. For patients who do not survive this period, VFDs […]See more -
Review Article
A deep look into the rib cage compression technique in mechanically ventilated patients: a narrative review
Rev Bras Ter Intensiva. 2022;34(1):176-184
Abstract
Review ArticleA deep look into the rib cage compression technique in mechanically ventilated patients: a narrative review
Rev Bras Ter Intensiva. 2022;34(1):176-184
DOI 10.5935/0103-507X.20220012-en
Views3ABSTRACT
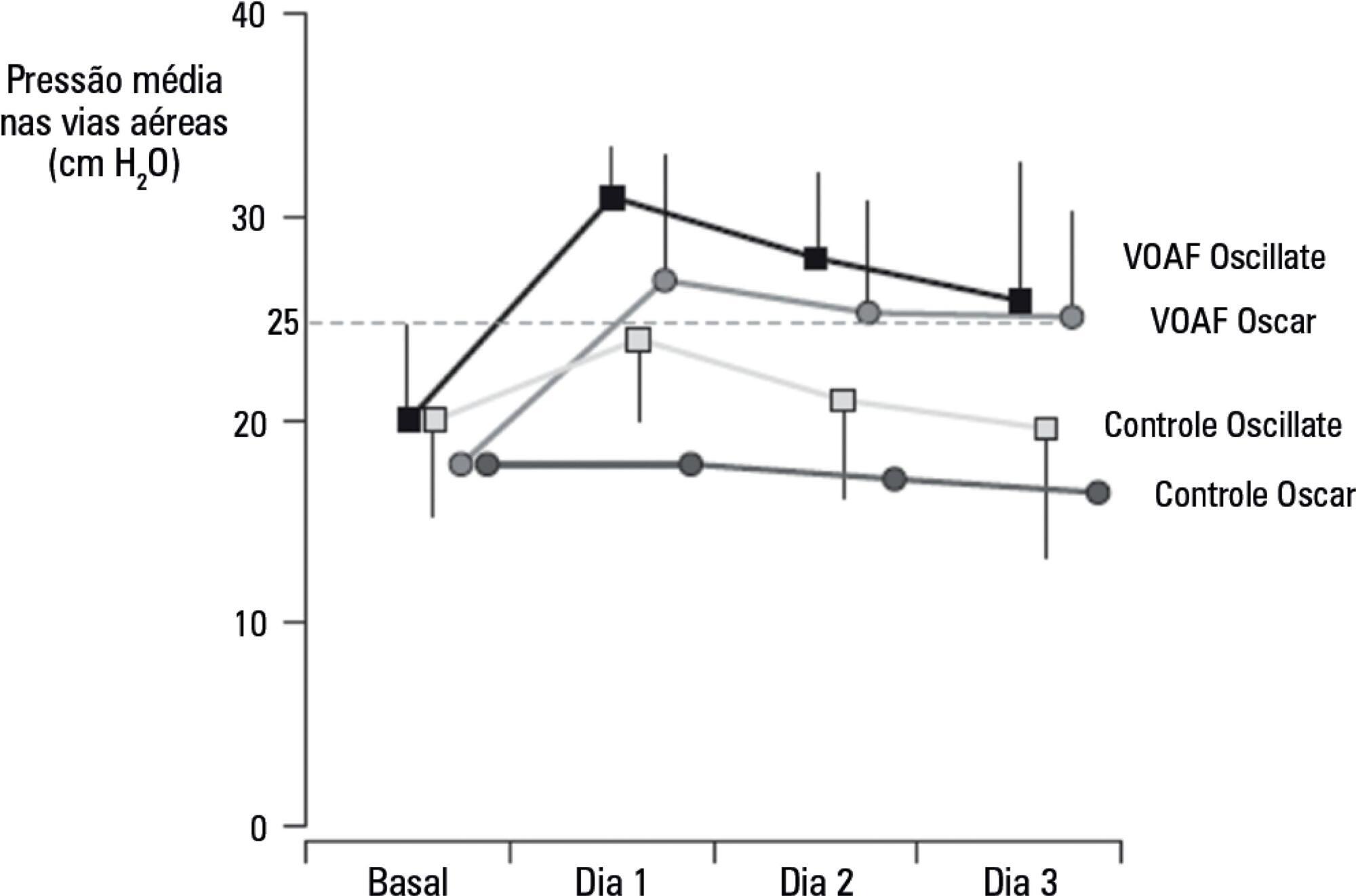
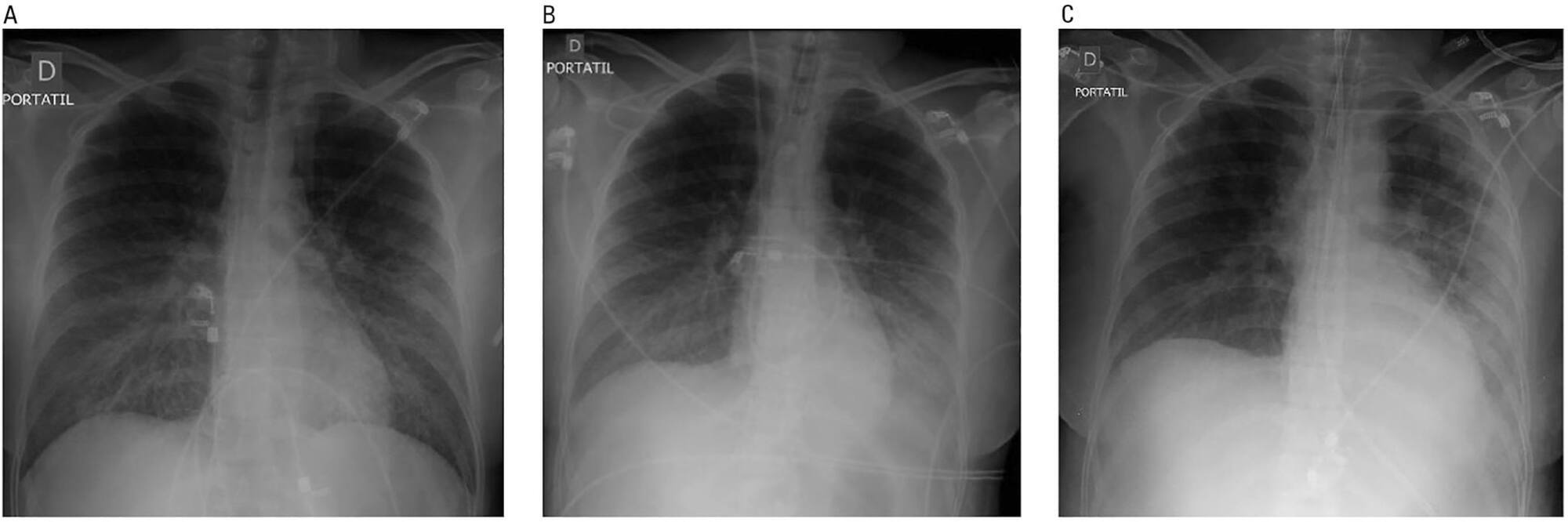
Defective management of secretions is one of the most frequent complications in invasive mechanically ventilated patients. Clearance of secretions through chest physiotherapy is a critical aspect of the treatment of these patients. Manual rib cage compression is one of the most practiced chest physiotherapy techniques in ventilated patients; however, its impact on clinical outcomes remains controversial due to methodological issues and poor understanding of its action. In this review, we present a detailed analysis of the physical principles involved in rib cage compression technique performance, as well as the physiological effects observed in experimental and clinical studies, which show that the use of brief and vigorous rib cage compression, based on increased expiratory flows (expiratory-inspiratory airflow difference of > 33L/minute), can improve mucus movement toward the glottis. On the other hand, the use of soft and gradual rib cage compression throughout the whole expiratory phase does not impact the expiratory flows, resulting in ineffective or undesired effects in some cases. More physiological studies are needed to understand the principles of the rib cage compression technique in ventilated humans. However, according to the evidence, rib cage compression has more potential benefits than risks, so its implementation should be promoted.
Keywords:artificialCritical careMucociliary clearancePhysical therapy modalitiesPressureRespirationRespiratory therapyRib cageSee moreViews3Abstract
Review ArticleA deep look into the rib cage compression technique in mechanically ventilated patients: a narrative review
Rev Bras Ter Intensiva. 2022;34(1):176-184
DOI 10.5935/0103-507X.20220012-en
Views3ABSTRACT
Defective management of secretions is one of the most frequent complications in invasive mechanically ventilated patients. Clearance of secretions through chest physiotherapy is a critical aspect of the treatment of these patients. Manual rib cage compression is one of the most practiced chest physiotherapy techniques in ventilated patients; however, its impact on clinical outcomes remains controversial due to methodological issues and poor understanding of its action. In this review, we present a detailed analysis of the physical principles involved in rib cage compression technique performance, as well as the physiological effects observed in experimental and clinical studies, which show that the use of brief and vigorous rib cage compression, based on increased expiratory flows (expiratory-inspiratory airflow difference of > 33L/minute), can improve mucus movement toward the glottis. On the other hand, the use of soft and gradual rib cage compression throughout the whole expiratory phase does not impact the expiratory flows, resulting in ineffective or undesired effects in some cases. More physiological studies are needed to understand the principles of the rib cage compression technique in ventilated humans. However, according to the evidence, rib cage compression has more potential benefits than risks, so its implementation should be promoted.
Keywords:artificialCritical careMucociliary clearancePhysical therapy modalitiesPressureRespirationRespiratory therapyRib cageSee more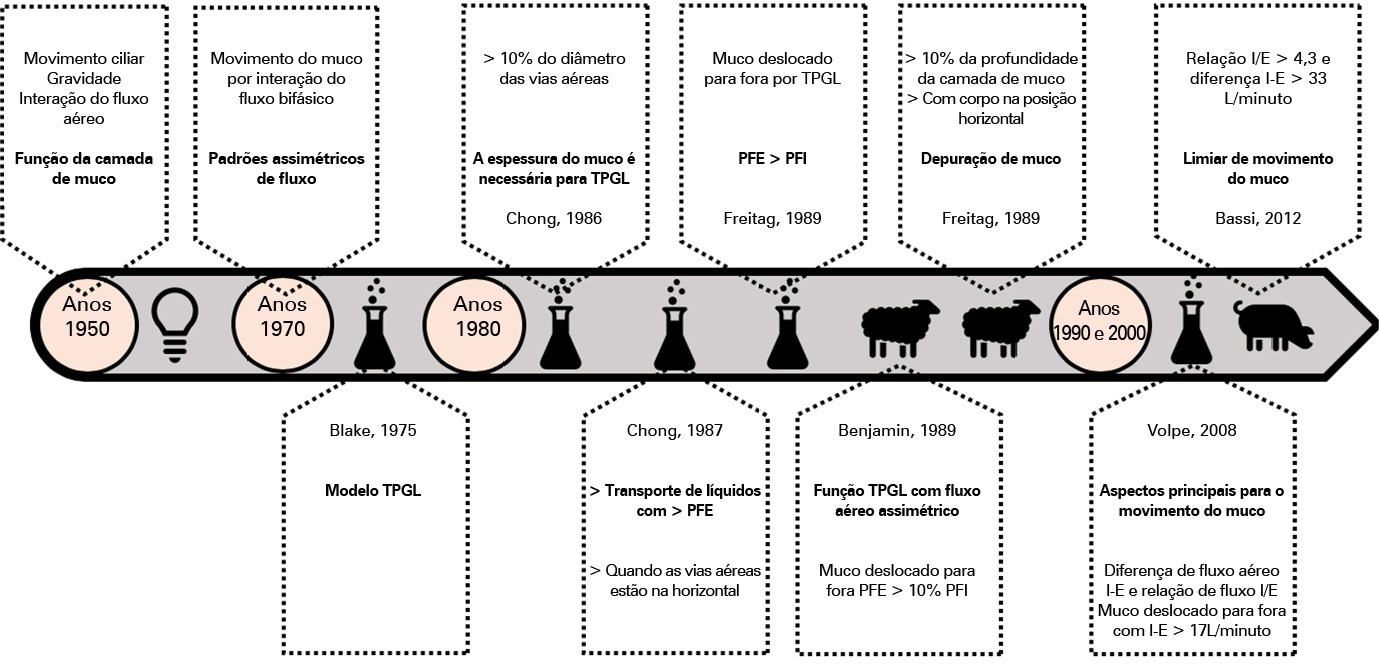
-
Review Articles
Does the use of high PEEP levels prevent ventilator-induced lung injury?
Rev Bras Ter Intensiva. 2017;29(2):231-237
Abstract
Review ArticlesDoes the use of high PEEP levels prevent ventilator-induced lung injury?
Rev Bras Ter Intensiva. 2017;29(2):231-237
DOI 10.5935/0103-507X.20170032
Views0See moreABSTRACT
Overdistention and intratidal alveolar recruitment have been advocated as the main physical mechanisms responsible for ventilator-induced lung injury. Limiting tidal volume has a demonstrated survival benefit in patients with acute respiratory distress syndrome and is recognized as the cornerstone of protective ventilation. In contrast, the use of high positive end-expiratory pressure levels in clinical trials has yielded conflicting results and remains controversial. In the present review, we will discuss the benefits and limitations of the open lung approach and will discuss some recent experimental and clinical trials on the use of high versus low/moderate positive end-expiratory pressure levels. We will also distinguish dynamic (tidal volume) from static strain (positive end-expiratory pressure and mean airway pressure) and will discuss their roles in inducing ventilator-induced lung injury. High positive end-expiratory pressure strategies clearly decrease refractory hypoxemia in patients with acute respiratory distress syndrome, but they also increase static strain, which in turn may harm patients, especially those with lower levels of lung recruitability. In patients with severe respiratory failure, titrating positive end-expiratory pressure against the severity of hypoxemia, or providing it in a decremental fashion after a recruitment maneuver, is recommended. If high plateau, driving or mean airway pressures are observed, prone positioning or ultraprotective ventilation may be indicated to improve oxygenation without additional stress and strain in the lung.
Views0Abstract
Review ArticlesDoes the use of high PEEP levels prevent ventilator-induced lung injury?
Rev Bras Ter Intensiva. 2017;29(2):231-237
DOI 10.5935/0103-507X.20170032
Views0See moreABSTRACT
Overdistention and intratidal alveolar recruitment have been advocated as the main physical mechanisms responsible for ventilator-induced lung injury. Limiting tidal volume has a demonstrated survival benefit in patients with acute respiratory distress syndrome and is recognized as the cornerstone of protective ventilation. In contrast, the use of high positive end-expiratory pressure levels in clinical trials has yielded conflicting results and remains controversial. In the present review, we will discuss the benefits and limitations of the open lung approach and will discuss some recent experimental and clinical trials on the use of high versus low/moderate positive end-expiratory pressure levels. We will also distinguish dynamic (tidal volume) from static strain (positive end-expiratory pressure and mean airway pressure) and will discuss their roles in inducing ventilator-induced lung injury. High positive end-expiratory pressure strategies clearly decrease refractory hypoxemia in patients with acute respiratory distress syndrome, but they also increase static strain, which in turn may harm patients, especially those with lower levels of lung recruitability. In patients with severe respiratory failure, titrating positive end-expiratory pressure against the severity of hypoxemia, or providing it in a decremental fashion after a recruitment maneuver, is recommended. If high plateau, driving or mean airway pressures are observed, prone positioning or ultraprotective ventilation may be indicated to improve oxygenation without additional stress and strain in the lung.
-
Case Report
Hantavirus cardiopulmonary syndrome successfully treated with high-volume hemofiltration
Rev Bras Ter Intensiva. 2016;28(2):190-194
Abstract
Case ReportHantavirus cardiopulmonary syndrome successfully treated with high-volume hemofiltration
Rev Bras Ter Intensiva. 2016;28(2):190-194
DOI 10.5935/0103-507X.20160032
Views0See moreABSTRACT
Hantavirus cardiopulmonary syndrome has a high mortality rate, and early connection to extracorporeal membrane oxygenation has been suggested to improve outcomes. We report the case of a patient with demonstrated Hantavirus cardiopulmonary syndrome and refractory shock who fulfilled the criteria for extracorporeal membrane oxygenation and responded successfully to high volume continuous hemofiltration. The implementation of high volume continuous hemofiltration along with protective ventilation reversed the shock within a few hours and may have prompted recovery. In patients with Hantavirus cardiopulmonary syndrome, a short course of high volume continuous hemofiltration may help differentiate patients who can be treated with conventional intensive care unit management from those who will require more complex therapies, such as extracorporeal membrane oxygenation.
Views0Abstract
Case ReportHantavirus cardiopulmonary syndrome successfully treated with high-volume hemofiltration
Rev Bras Ter Intensiva. 2016;28(2):190-194
DOI 10.5935/0103-507X.20160032
Views0See moreABSTRACT
Hantavirus cardiopulmonary syndrome has a high mortality rate, and early connection to extracorporeal membrane oxygenation has been suggested to improve outcomes. We report the case of a patient with demonstrated Hantavirus cardiopulmonary syndrome and refractory shock who fulfilled the criteria for extracorporeal membrane oxygenation and responded successfully to high volume continuous hemofiltration. The implementation of high volume continuous hemofiltration along with protective ventilation reversed the shock within a few hours and may have prompted recovery. In patients with Hantavirus cardiopulmonary syndrome, a short course of high volume continuous hemofiltration may help differentiate patients who can be treated with conventional intensive care unit management from those who will require more complex therapies, such as extracorporeal membrane oxygenation.
-
Original Articles – Clinical Research
Positive end-expiratory pressure increases strain in patients with ALI/ARDS
Rev Bras Ter Intensiva. 2012;24(1):43-51
Abstract
Original Articles – Clinical ResearchPositive end-expiratory pressure increases strain in patients with ALI/ARDS
Rev Bras Ter Intensiva. 2012;24(1):43-51
DOI 10.1590/S0103-507X2012000100007
Views0OBJECTIVE: The objective of this study was to assess the effects of positive end-expiratory pressure on recruitment, cyclic recruitment and derecruitment and strain in patients with acute lung injury and acute respiratory distress syndrome using lung computed tomography. METHODS: This is an open, controlled, non-randomized interventional study of ten patients with acute lung injury and acute respiratory distress syndrome. Using computed tomography, single, basal slices of the lung were obtained during inspiratory and expiratory pauses at a tidal volume of 6 ml/kg and a positive end-expiratory pressure of 5, 10, 15 and 20 cmH2O. The densities of the lung parenchyma were measured in Hounsfield units. The values for positive end-expiratory pressure-induced recruitment, cyclic recruitment and derecruitment and strain were then calculated. RESULTS: Increasing levels of positive end-expiratory pressure were correlated with increased recruitment and global strain (p < 0.01), which was significantly correlated with plateau pressure (r² = 0.97, p < 0.01). In addition, increasing levels of positive end-expiratory pressure systematically increased strain along the sternovertebral axis. CONCLUSION: While strain is an adverse effect of positive end-expiratory pressure, the decision use positive end-expiratory pressure with any patient should be balanced against the potential benefits of recruitment. Due to the small number of patients in this study, the present data should be treated as hypothesis generating and is not intended to limit the clinical application of a high level of positive end-expiratory pressure in patients with severe hypoxemia.
Keywords:Positive end-expiratory pressureRespiration, artificialRespiratory distress syndrome, adultTomography, X-ray computedSee moreViews0Abstract
Original Articles – Clinical ResearchPositive end-expiratory pressure increases strain in patients with ALI/ARDS
Rev Bras Ter Intensiva. 2012;24(1):43-51
DOI 10.1590/S0103-507X2012000100007
Views0OBJECTIVE: The objective of this study was to assess the effects of positive end-expiratory pressure on recruitment, cyclic recruitment and derecruitment and strain in patients with acute lung injury and acute respiratory distress syndrome using lung computed tomography. METHODS: This is an open, controlled, non-randomized interventional study of ten patients with acute lung injury and acute respiratory distress syndrome. Using computed tomography, single, basal slices of the lung were obtained during inspiratory and expiratory pauses at a tidal volume of 6 ml/kg and a positive end-expiratory pressure of 5, 10, 15 and 20 cmH2O. The densities of the lung parenchyma were measured in Hounsfield units. The values for positive end-expiratory pressure-induced recruitment, cyclic recruitment and derecruitment and strain were then calculated. RESULTS: Increasing levels of positive end-expiratory pressure were correlated with increased recruitment and global strain (p < 0.01), which was significantly correlated with plateau pressure (r² = 0.97, p < 0.01). In addition, increasing levels of positive end-expiratory pressure systematically increased strain along the sternovertebral axis. CONCLUSION: While strain is an adverse effect of positive end-expiratory pressure, the decision use positive end-expiratory pressure with any patient should be balanced against the potential benefits of recruitment. Due to the small number of patients in this study, the present data should be treated as hypothesis generating and is not intended to limit the clinical application of a high level of positive end-expiratory pressure in patients with severe hypoxemia.
Keywords:Positive end-expiratory pressureRespiration, artificialRespiratory distress syndrome, adultTomography, X-ray computedSee more
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis