Clinical Report Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2024;36:e20240258en
DOI 10.62675/2965-2774.20240258-en
Evidence about long-term sequelae after hospitalization for acute respiratory distress syndrome due to COVID-19 is still scarce.
To evaluate changes in pulmonary, cardiac, and renal function and in quality of life after hospitalization for acute respiratory distress syndrome secondary to COVID-19.
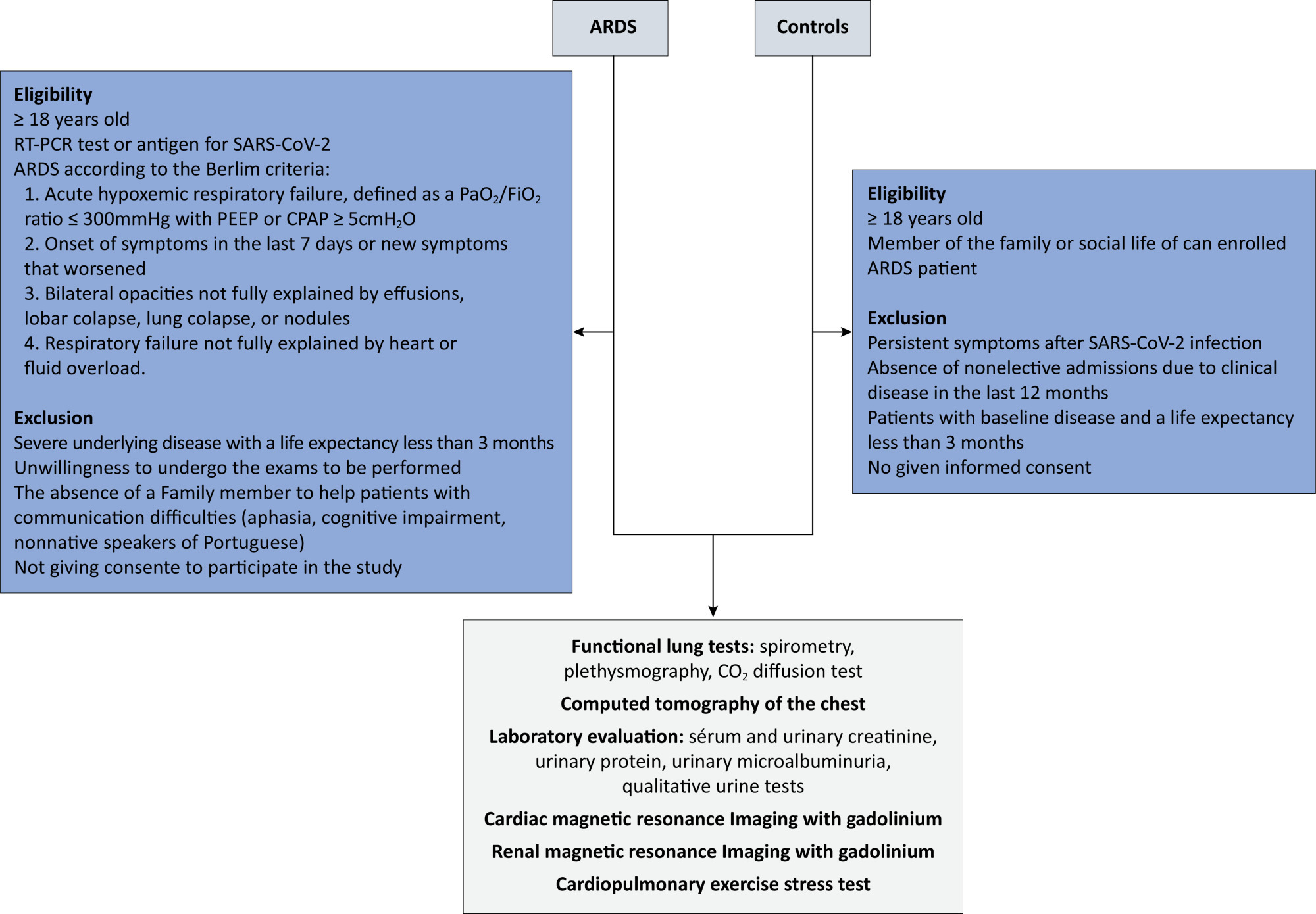
This will be a multicenter case–control study of 220 participants. Eligible are patients who are hospitalized for acute respiratory distress syndrome due to COVID-19. In the control group, individuals with no history of hospitalization in the last 12 months or long-term symptoms of COVID-19 will be selected. All individuals will be subjected to pulmonary spirometry with a carbon monoxide diffusion test, chest tomography, cardiac and renal magnetic resonance imaging with gadolinium, ergospirometry, serum and urinary creatinine, total protein, and urinary microalbuminuria, in addition to quality-of-life questionnaires. Patients will be evaluated 12 months after hospital discharge, and controls will be evaluated within 90 days of inclusion in the study. For all the statistical analyses, p < 0.05 is the threshold for significance.
The primary outcome of the study will be the pulmonary diffusing capacity for carbon monoxide measured after 12 months. The other parameters of pulmonary, cardiac, and renal function and quality of life are secondary outcomes.
This study aims to determine the long-term sequelae of pulmonary, cardiac, and renal function and the quality of life of patients hospitalized for acute respiratory distress syndrome due to COVID-19 in the Brazilian population.
Abstract
Crit Care Sci. 2024;36:e20240258en
DOI 10.62675/2965-2774.20240258-en
Evidence about long-term sequelae after hospitalization for acute respiratory distress syndrome due to COVID-19 is still scarce.
To evaluate changes in pulmonary, cardiac, and renal function and in quality of life after hospitalization for acute respiratory distress syndrome secondary to COVID-19.
This will be a multicenter case–control study of 220 participants. Eligible are patients who are hospitalized for acute respiratory distress syndrome due to COVID-19. In the control group, individuals with no history of hospitalization in the last 12 months or long-term symptoms of COVID-19 will be selected. All individuals will be subjected to pulmonary spirometry with a carbon monoxide diffusion test, chest tomography, cardiac and renal magnetic resonance imaging with gadolinium, ergospirometry, serum and urinary creatinine, total protein, and urinary microalbuminuria, in addition to quality-of-life questionnaires. Patients will be evaluated 12 months after hospital discharge, and controls will be evaluated within 90 days of inclusion in the study. For all the statistical analyses, p < 0.05 is the threshold for significance.
The primary outcome of the study will be the pulmonary diffusing capacity for carbon monoxide measured after 12 months. The other parameters of pulmonary, cardiac, and renal function and quality of life are secondary outcomes.
This study aims to determine the long-term sequelae of pulmonary, cardiac, and renal function and the quality of life of patients hospitalized for acute respiratory distress syndrome due to COVID-19 in the Brazilian population.
Abstract
Crit Care Sci. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
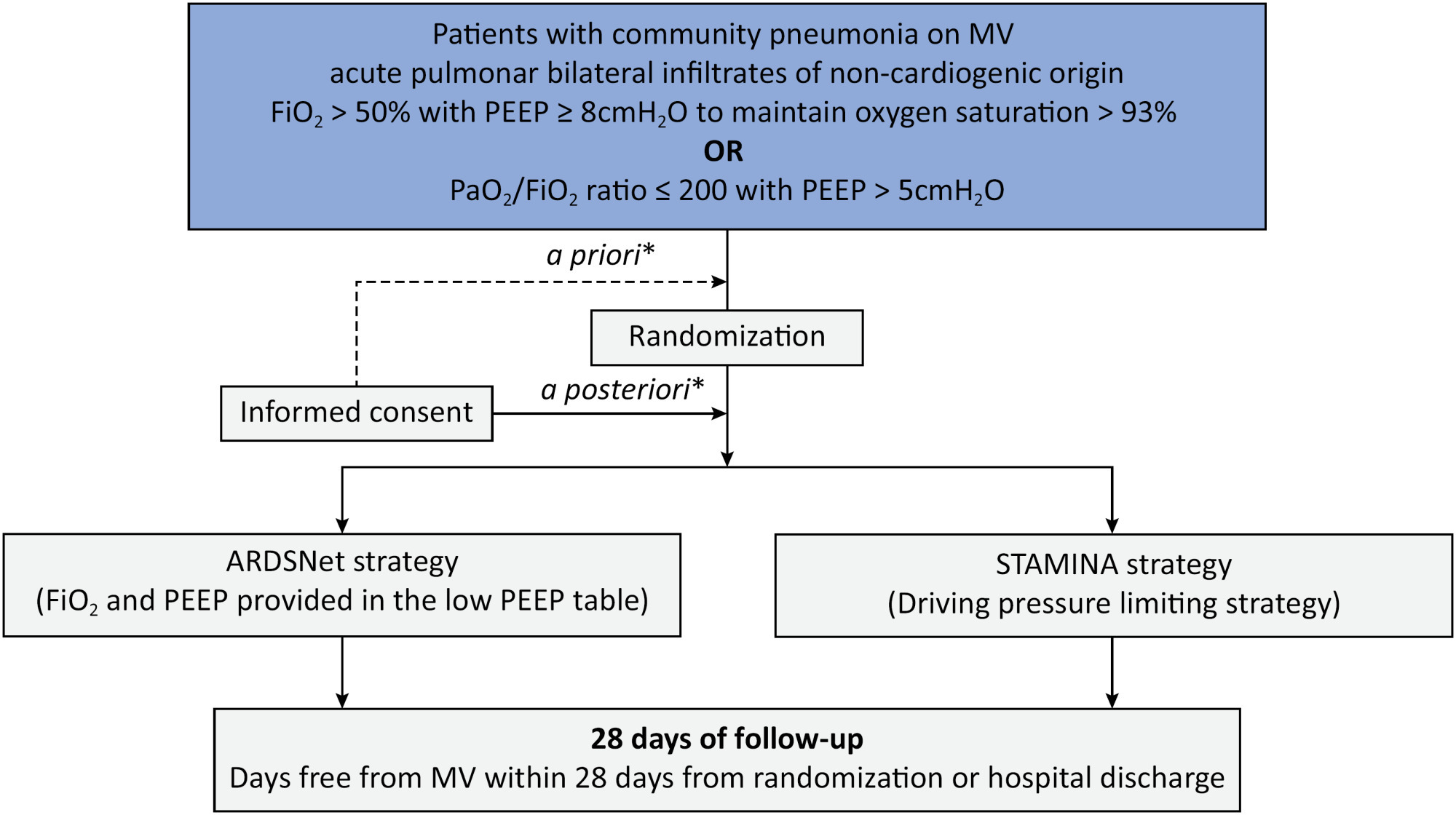
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Abstract
Crit Care Sci. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Abstract
Crit Care Sci. 2024;36:e20240235en
DOI 10.62675/2965-2774.20240235-pt
Newborn infants admitted to the neonatal intensive care unit require arterial cannulation for hemodynamic monitoring and blood sampling. Arterial access is achieved through catheterization of umbilical or peripheral arteries. Peripheral artery cannulation is performed in critically ill newborns, but artery localization and cannulation is often challenging and unsuccessful. Therefore, increasing the internal diameter and preventing vasospasm are important for successful peripheral artery cannulation in neonates. Topical glyceryl trinitrate has the potential to increase cannulation success by relaxing arterial smooth muscles and thus increasing the internal diameter. We aim to conduct a pilot randomized controlled trial to evaluate the efficacy and safety of topycal glyceryl trinitrate in increasing the diameter of the radial artery in neonates.
This study will be a single-center, observer-blind, randomized, placebo-controlled trial conducted in the neonatal intensive care unit of Perth Children's Hospital, Western Australia. A total of 60 infants born at >34 weeks of gestation who are admitted for elective surgery or medical reasons and for whom a peripheral arterial line is needed for sampling or blood pressure monitoring will be recruited after informed parental consent is obtained. The primary outcome will be the change in radial arterial diameter from baseline to postintervention. Secondary outcomes will be the absolute and percentage change from baseline in the radial arterial diameter in both limbs and safety (hypotension and methemoglobinemia).
This will be the first randomized controlled trial evaluating the use of topical glyceryl trinitrate to facilitate peripheral artery cannulation in neonates. If our pilot randomized controlled trial confirms the benefits of glyceryl trinitrate patches, it will pave the way for large multicenter randomized controlled trials in this field.
Abstract
Crit Care Sci. 2024;36:e20240235en
DOI 10.62675/2965-2774.20240235-pt
Newborn infants admitted to the neonatal intensive care unit require arterial cannulation for hemodynamic monitoring and blood sampling. Arterial access is achieved through catheterization of umbilical or peripheral arteries. Peripheral artery cannulation is performed in critically ill newborns, but artery localization and cannulation is often challenging and unsuccessful. Therefore, increasing the internal diameter and preventing vasospasm are important for successful peripheral artery cannulation in neonates. Topical glyceryl trinitrate has the potential to increase cannulation success by relaxing arterial smooth muscles and thus increasing the internal diameter. We aim to conduct a pilot randomized controlled trial to evaluate the efficacy and safety of topycal glyceryl trinitrate in increasing the diameter of the radial artery in neonates.
This study will be a single-center, observer-blind, randomized, placebo-controlled trial conducted in the neonatal intensive care unit of Perth Children's Hospital, Western Australia. A total of 60 infants born at >34 weeks of gestation who are admitted for elective surgery or medical reasons and for whom a peripheral arterial line is needed for sampling or blood pressure monitoring will be recruited after informed parental consent is obtained. The primary outcome will be the change in radial arterial diameter from baseline to postintervention. Secondary outcomes will be the absolute and percentage change from baseline in the radial arterial diameter in both limbs and safety (hypotension and methemoglobinemia).
This will be the first randomized controlled trial evaluating the use of topical glyceryl trinitrate to facilitate peripheral artery cannulation in neonates. If our pilot randomized controlled trial confirms the benefits of glyceryl trinitrate patches, it will pave the way for large multicenter randomized controlled trials in this field.