Septic shock Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2008;20(2):173-177
DOI 10.1590/S0103-507X2008000200010
BACKGROUND AND OBJECTIVES: The debate on efficacy and patient safety related to the use of drotrecogin alfa (DrotAA) is timely, principally due to the negative results observed in clinical studies performed after the PROWESS study, and the economic cost-related impact of the drug on the healthcare system. The aim of this study was to review the main studies on the use of DrotAA in patients with severe sepsis. The focus was on drug efficacy-and patient safety-related issues. CONTENTS: Articles were selected by a MedLine search for studies on the use of DrotAA in patients with sepsis using the following key words: activated protein C; drotrecogin alfa; sepsis; septic shock; Xigris®. Additional references were retrieved from the studies initially selected. CONCLUSIONS: Mortality and bleeding complications associated with the use of DrotAA were more frequent in large observational studies than those reported in randomized trials. In the light of the current knowledge, routine use of DrotAA should be reevaluated until well-designed confirmatory clinical trials can clarify the true efficacy and safety of the drug and help identify the subgroup of patients that can benefit from use of DrotAA. Physicians should be cautious with the rapid transfer of evidences not well-documented, to the guidelines and recommendations practiced in the care and treatment of patients with severe sepsis.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):173-177
DOI 10.1590/S0103-507X2008000200010
BACKGROUND AND OBJECTIVES: The debate on efficacy and patient safety related to the use of drotrecogin alfa (DrotAA) is timely, principally due to the negative results observed in clinical studies performed after the PROWESS study, and the economic cost-related impact of the drug on the healthcare system. The aim of this study was to review the main studies on the use of DrotAA in patients with severe sepsis. The focus was on drug efficacy-and patient safety-related issues. CONTENTS: Articles were selected by a MedLine search for studies on the use of DrotAA in patients with sepsis using the following key words: activated protein C; drotrecogin alfa; sepsis; septic shock; Xigris®. Additional references were retrieved from the studies initially selected. CONCLUSIONS: Mortality and bleeding complications associated with the use of DrotAA were more frequent in large observational studies than those reported in randomized trials. In the light of the current knowledge, routine use of DrotAA should be reevaluated until well-designed confirmatory clinical trials can clarify the true efficacy and safety of the drug and help identify the subgroup of patients that can benefit from use of DrotAA. Physicians should be cautious with the rapid transfer of evidences not well-documented, to the guidelines and recommendations practiced in the care and treatment of patients with severe sepsis.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):128-134
DOI 10.1590/S0103-507X2008000200003
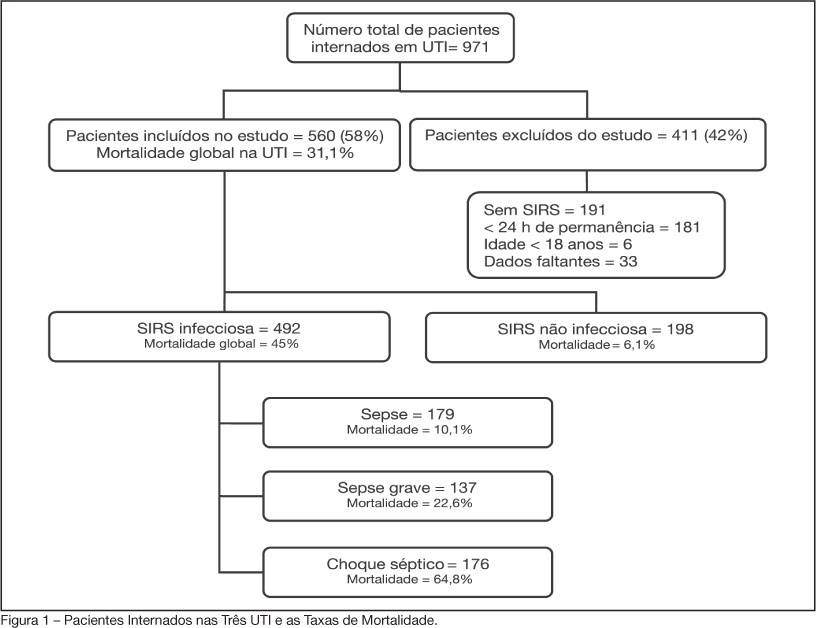
BACKGROUND AND OBJECTIVES: Sepsis is the main cause of death in patients treated in intensive care units (ICU). The aim of this study was to evaluate etiology, prognostic factors and mortality of septic patients treated in ICU of Passo Fundo, Brazil. METHODS: Out of 971 consecutive patients prospectively evaluated from August 2005 to February 2006, 560 were selected due to presence of systemic inflammatory response syndrome (SIRS) and followed for 28 days or until discharge or death. Patients were categorized according with the etiology of SIRS and further classified as having SIRS, sepsis, severe sepsis and septic shock. Prognosis was assessed by means of Apache II and SOFA. Mortality was compared in different etiologies of sepsis, APACHE II and SOFA scores, parameters. RESULTS: Of the 971 patients admitted to the ICU, 560 developed SIRS (58%). The most frequent cause of internation was neurological disease (28.9%), the most frequent site of infection was the respiratory tract (71.6%), and the most prevalent pathogens were gram-negative bacilli (53.2%). Mean APACHE II score was 18 ± 9, and mean SOFA score was 5 ± 4. Median ICU stay was 6 (3-11) days and overall mortality rate was 31.1%: 6.1% for non-infectious SIRS, 10.1% for sepsis, 22.6% for severe sepsis, and 64.8% for septic shock. CONCLUSIONS: Sepsis is an important health problem that leads to an extremely high mortality rate in the ICU of Passo Fundo, Brazil.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):128-134
DOI 10.1590/S0103-507X2008000200003
BACKGROUND AND OBJECTIVES: Sepsis is the main cause of death in patients treated in intensive care units (ICU). The aim of this study was to evaluate etiology, prognostic factors and mortality of septic patients treated in ICU of Passo Fundo, Brazil. METHODS: Out of 971 consecutive patients prospectively evaluated from August 2005 to February 2006, 560 were selected due to presence of systemic inflammatory response syndrome (SIRS) and followed for 28 days or until discharge or death. Patients were categorized according with the etiology of SIRS and further classified as having SIRS, sepsis, severe sepsis and septic shock. Prognosis was assessed by means of Apache II and SOFA. Mortality was compared in different etiologies of sepsis, APACHE II and SOFA scores, parameters. RESULTS: Of the 971 patients admitted to the ICU, 560 developed SIRS (58%). The most frequent cause of internation was neurological disease (28.9%), the most frequent site of infection was the respiratory tract (71.6%), and the most prevalent pathogens were gram-negative bacilli (53.2%). Mean APACHE II score was 18 ± 9, and mean SOFA score was 5 ± 4. Median ICU stay was 6 (3-11) days and overall mortality rate was 31.1%: 6.1% for non-infectious SIRS, 10.1% for sepsis, 22.6% for severe sepsis, and 64.8% for septic shock. CONCLUSIONS: Sepsis is an important health problem that leads to an extremely high mortality rate in the ICU of Passo Fundo, Brazil.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):135-143
DOI 10.1590/S0103-507X2008000200004
BACKGROUND AND OBJECTIVES: To face the high mortality of sepsis, interventions grouped as "Surviving Sepsis Campaign" have been suggested. The aim of the study was to describe the application of glycemic control, corticoid use in septic shock, inotropics and drotrecogin-alpha in sepsis. METHODS: We studied 110 patients with sepsis from Recife/Brazil, who received drotrecogin-alpha between 2003/2006. Data on management of sepsis considering Surviving Sepsis Campaign, drotrecogin-alpha, mortality at 28 days and severe bleeding were recorded. RESULTS: Mean APACHE II was 25.6 and mean SOFA was 9.2. Around 95% of the patients presented two or more organ dysfunctions and 98% presented septic shock. The majority (56%) were under 65 years. Abdominal (48%) and respiratory (28%) focus of infection were the most prevalent. Hydrocortisone was used in 61% of the patients, and 29 (48.3%) died. Of the 38 patients with prolonged shock that did not receive it, 28 (73.7%) died. Of the 97 patients who presented uncontrolled glycemia only 65% achieved strict glycemic control and the mortality was 51.6%. Fluid gain ranged from 600 ml to 9,400 ml in the first 24h. In only 30 patients was myocardial dysfunction detected. The infusion of drotrecogin alpha started within 24h in 45%, between 24 and 48h in 35% and after 48h in 20%. Death occurred in 57% and severe bleeding in 9%. CONCLUSIONS: Discrepancy between the recommendations of Surviving Sepsis Campaign and clinical practice was observed. Death rate was 57%, similar to that found in the literature for septic shock irrespective of the use of drotrecogin-alpha.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):135-143
DOI 10.1590/S0103-507X2008000200004
BACKGROUND AND OBJECTIVES: To face the high mortality of sepsis, interventions grouped as "Surviving Sepsis Campaign" have been suggested. The aim of the study was to describe the application of glycemic control, corticoid use in septic shock, inotropics and drotrecogin-alpha in sepsis. METHODS: We studied 110 patients with sepsis from Recife/Brazil, who received drotrecogin-alpha between 2003/2006. Data on management of sepsis considering Surviving Sepsis Campaign, drotrecogin-alpha, mortality at 28 days and severe bleeding were recorded. RESULTS: Mean APACHE II was 25.6 and mean SOFA was 9.2. Around 95% of the patients presented two or more organ dysfunctions and 98% presented septic shock. The majority (56%) were under 65 years. Abdominal (48%) and respiratory (28%) focus of infection were the most prevalent. Hydrocortisone was used in 61% of the patients, and 29 (48.3%) died. Of the 38 patients with prolonged shock that did not receive it, 28 (73.7%) died. Of the 97 patients who presented uncontrolled glycemia only 65% achieved strict glycemic control and the mortality was 51.6%. Fluid gain ranged from 600 ml to 9,400 ml in the first 24h. In only 30 patients was myocardial dysfunction detected. The infusion of drotrecogin alpha started within 24h in 45%, between 24 and 48h in 35% and after 48h in 20%. Death occurred in 57% and severe bleeding in 9%. CONCLUSIONS: Discrepancy between the recommendations of Surviving Sepsis Campaign and clinical practice was observed. Death rate was 57%, similar to that found in the literature for septic shock irrespective of the use of drotrecogin-alpha.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):9-17
DOI 10.1590/S0103-507X2006000100003
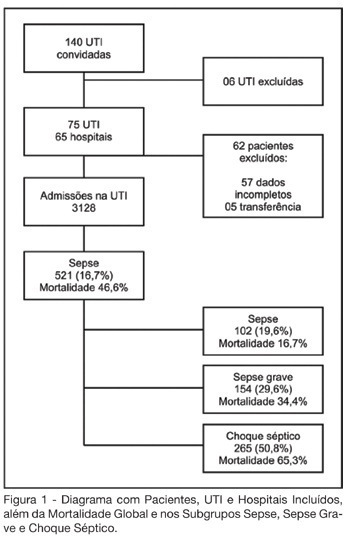
BACKGROUND AND OBJECTIVES: Sepsis represents the major cause of death in the ICUs all over the world. Many studies have shown an increasing incidence over time and only a slight reduce in mortality. Many new treatment strategies are arising and we should define the incidence and features of sepsis in Brazil. METHODS: Prospective cohort study in sixty-five hospitals all over Brazil. The patients who were admitted or who developed sepsis during the month of September, 2003 were enrolled. They were followed until the 28th day and/or until their discharge. The diagnoses were made in accordance to the criteria proposed by ACCP/SCCM. It were evaluated demographic features, APACHE II score, SOFA (Sepsis-related Organ Failure Assessment) score, mortality, sources of infections, microbiology, morbidities and length of stay (LOS). RESULTS: Seventy-five ICUs from all regions of Brazil took part in the study.3128 patients were identified and 521 (16.7%) filled the criteria of sepsis, severe sepsis or septic shock. Mean age was 61.7 (IQR 39-79), 293 (55.7%) were males, and the overall 28-day mortality rate was 46.6%. Average APACHE II score was 20 and SOFA score on the first day was 7 (IQR 4-10). SOFA score in the mortality group was higher on day 1 (8, IQR 5-11), and had increased on day 3 (9, IQR 6-12). The mortality rate for sepsis, severe sepsis and septic shock was 16.7%, 34.4% and 65.3%, respectively. The average LOS was 15 days (IQR 5-22). The two main sources of infection were the respiratory tract (69%) and the abdomen one (23.1%). Gram-negative bacilli were more prevalent (40.1%). Gram-positive cocci were identified in 32.8% and fungi infections in 5%. Mechanical ventilation was observed in 82.1% of the patients, Swan-Ganz catheter in 18.8%, vasopressors in 66.2% and hemotransfusion in 44.7%. CONCLUSIONS: It was observed a high mortality of sepsis in the ICUs in Brazil. The high frequency of septic shock demonstrated a group at high risk of death. In order to have a better use of the resources and reduce in mortality during the next 5 years, it is very important to identify our specific features related to this syndrome.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):9-17
DOI 10.1590/S0103-507X2006000100003
BACKGROUND AND OBJECTIVES: Sepsis represents the major cause of death in the ICUs all over the world. Many studies have shown an increasing incidence over time and only a slight reduce in mortality. Many new treatment strategies are arising and we should define the incidence and features of sepsis in Brazil. METHODS: Prospective cohort study in sixty-five hospitals all over Brazil. The patients who were admitted or who developed sepsis during the month of September, 2003 were enrolled. They were followed until the 28th day and/or until their discharge. The diagnoses were made in accordance to the criteria proposed by ACCP/SCCM. It were evaluated demographic features, APACHE II score, SOFA (Sepsis-related Organ Failure Assessment) score, mortality, sources of infections, microbiology, morbidities and length of stay (LOS). RESULTS: Seventy-five ICUs from all regions of Brazil took part in the study.3128 patients were identified and 521 (16.7%) filled the criteria of sepsis, severe sepsis or septic shock. Mean age was 61.7 (IQR 39-79), 293 (55.7%) were males, and the overall 28-day mortality rate was 46.6%. Average APACHE II score was 20 and SOFA score on the first day was 7 (IQR 4-10). SOFA score in the mortality group was higher on day 1 (8, IQR 5-11), and had increased on day 3 (9, IQR 6-12). The mortality rate for sepsis, severe sepsis and septic shock was 16.7%, 34.4% and 65.3%, respectively. The average LOS was 15 days (IQR 5-22). The two main sources of infection were the respiratory tract (69%) and the abdomen one (23.1%). Gram-negative bacilli were more prevalent (40.1%). Gram-positive cocci were identified in 32.8% and fungi infections in 5%. Mechanical ventilation was observed in 82.1% of the patients, Swan-Ganz catheter in 18.8%, vasopressors in 66.2% and hemotransfusion in 44.7%. CONCLUSIONS: It was observed a high mortality of sepsis in the ICUs in Brazil. The high frequency of septic shock demonstrated a group at high risk of death. In order to have a better use of the resources and reduce in mortality during the next 5 years, it is very important to identify our specific features related to this syndrome.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):196-199
DOI 10.1590/S0103-507X2006000200014
BACKGROUND AND OBJECTIVES: The hemodynamic support of sepsis is now formulated trying to insert terlipressin as salvage drug in catecholamine resistant shock, justifying a broad critical analysis. CONTENTS: The analysis included hemodynamic therapies with defined specific goals and new recommendations for fluid resuscitation, vasopressor therapy, and inotropic therapy of septic in adult and pediatric patients. CONCLUSIONS: Terlipressin appears as a new but controversial alternative for vasopressor therapy in sepsis.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):196-199
DOI 10.1590/S0103-507X2006000200014
BACKGROUND AND OBJECTIVES: The hemodynamic support of sepsis is now formulated trying to insert terlipressin as salvage drug in catecholamine resistant shock, justifying a broad critical analysis. CONTENTS: The analysis included hemodynamic therapies with defined specific goals and new recommendations for fluid resuscitation, vasopressor therapy, and inotropic therapy of septic in adult and pediatric patients. CONCLUSIONS: Terlipressin appears as a new but controversial alternative for vasopressor therapy in sepsis.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):18-23
DOI 10.1590/S0103-507X2008000100003
BACKGROUND AND OBJECTIVES: The incidence of relative adrenal insufficiency (RAI) in patients with septic shock is high and has a significant impact on survival. The purpose of this study was to determine whether a random cortisol concentration < 25 mg/dL was as good as a low dose (1 mg) corticotrophin stimulation test in the diagnosis of RAI in patients with septic shock as assessed by the hemodynamic response to hydrocortisone. METHODS: Patients were randomized to a single cortisol determination or to a low dose corticotrophin stimulation test. After blood collection to cortisol determinations, hydrocortisone (100 mg every 8 hrs) was administered for all patients in the first 36 hours. RAI was defined by a random cortisol concentration < 25 mg/dL or a D cortisol concentration < 9 mg/dL in the corticotrophin test. RESULTS: Sixty patients (G1 = 30; G2 = 30) were included in the analysis and were comparable regarding to demographic data, nosologies and disease severity. The time to norepinephrin withdrawal in group 1 patients with RAI diagnostic criteria was not different from the patients with cortisol > 25 mg/dL. In group 2 patients with D cortisol < 9 mg/dL had a shorter time of norepinephrin infusion (3 days) compared to patients with D cortisol > 9 (6 days). CONCLUSIONS: This study suggests that 1 mg corticotrophin test is better than a random cortisol determination < 25 mg/dL to the diagnosis of relative adrenal insufficiency in septic shock patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):18-23
DOI 10.1590/S0103-507X2008000100003
BACKGROUND AND OBJECTIVES: The incidence of relative adrenal insufficiency (RAI) in patients with septic shock is high and has a significant impact on survival. The purpose of this study was to determine whether a random cortisol concentration < 25 mg/dL was as good as a low dose (1 mg) corticotrophin stimulation test in the diagnosis of RAI in patients with septic shock as assessed by the hemodynamic response to hydrocortisone. METHODS: Patients were randomized to a single cortisol determination or to a low dose corticotrophin stimulation test. After blood collection to cortisol determinations, hydrocortisone (100 mg every 8 hrs) was administered for all patients in the first 36 hours. RAI was defined by a random cortisol concentration < 25 mg/dL or a D cortisol concentration < 9 mg/dL in the corticotrophin test. RESULTS: Sixty patients (G1 = 30; G2 = 30) were included in the analysis and were comparable regarding to demographic data, nosologies and disease severity. The time to norepinephrin withdrawal in group 1 patients with RAI diagnostic criteria was not different from the patients with cortisol > 25 mg/dL. In group 2 patients with D cortisol < 9 mg/dL had a shorter time of norepinephrin infusion (3 days) compared to patients with D cortisol > 9 (6 days). CONCLUSIONS: This study suggests that 1 mg corticotrophin test is better than a random cortisol determination < 25 mg/dL to the diagnosis of relative adrenal insufficiency in septic shock patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):402-406
DOI 10.1590/S0103-507X2006000400014
BACKGROUND AND OBJECTIVES: Sepsis is a syndrome with an important inflammatory component in its pathophysiology. Some drugs that act on the activation of inflammatory cascade have been tested in septic patients. Statins, beyond hypolipemic effects, have anti-inflammatory capacities, known as pleiotropic effects. That action may be of value on sepsis treatment. Review of publications who discuss the use of statins. This article has the objective to review the mainly papers about statins and sepses. METHODS: Original published articles were searched using Medline database crossing the keys words "sepsis and statins" between 1990 and 2006 RESULTS: Experimental and retrospective studies has been investigated the use of statins in septic patients, until this moment, most of then show benefits on morbidity and mortality. However, there is not prospective, randomized, placebo controlled trials. Or metanalyses, witch denotes lack strong and robust that could be indicated this action. So, since the benefit is still unable, it is necessary randomized clinical trials witch can prove this theory. CONCLUSIONS: Several experimental and retrospective studies have investigated the use of statins in septic patients, but despite literature demonstrating a promising role for its use in these patients, these studies are experimental or retrospective. Therefore, we must wait larger, prospective, randomized trials before we may be able to understand its role and possibly recommend these drugs in the treatment of septic patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):402-406
DOI 10.1590/S0103-507X2006000400014
BACKGROUND AND OBJECTIVES: Sepsis is a syndrome with an important inflammatory component in its pathophysiology. Some drugs that act on the activation of inflammatory cascade have been tested in septic patients. Statins, beyond hypolipemic effects, have anti-inflammatory capacities, known as pleiotropic effects. That action may be of value on sepsis treatment. Review of publications who discuss the use of statins. This article has the objective to review the mainly papers about statins and sepses. METHODS: Original published articles were searched using Medline database crossing the keys words "sepsis and statins" between 1990 and 2006 RESULTS: Experimental and retrospective studies has been investigated the use of statins in septic patients, until this moment, most of then show benefits on morbidity and mortality. However, there is not prospective, randomized, placebo controlled trials. Or metanalyses, witch denotes lack strong and robust that could be indicated this action. So, since the benefit is still unable, it is necessary randomized clinical trials witch can prove this theory. CONCLUSIONS: Several experimental and retrospective studies have investigated the use of statins in septic patients, but despite literature demonstrating a promising role for its use in these patients, these studies are experimental or retrospective. Therefore, we must wait larger, prospective, randomized trials before we may be able to understand its role and possibly recommend these drugs in the treatment of septic patients.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):437-443
DOI 10.1590/S0103-507X2007000400006
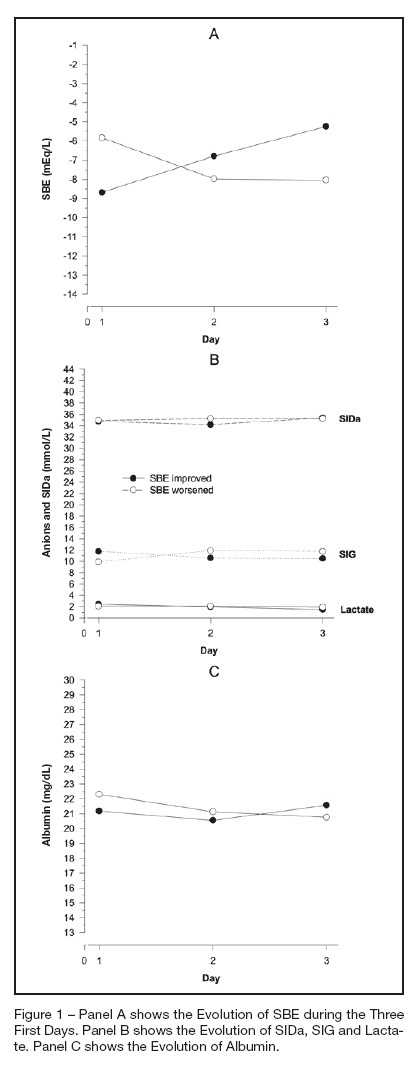
BACKGROUND AND OBJECTIVES: The amount of metabolic acidosis measured through the standard base excess (SBE) has been shown to be an outcome marker and its improvement has been associated with better survival. We studied the mechanism of standard base excess variation in the first three days of intensive care unit (ICU) stay through the evaluation of independent variables of physico-chemical approach. METHODS: Data were retrieved from our prospective collected data base from patients with diagnosis of septic shock, daily up to the third day after the ICU admission. Single correlations between SBE and independent variables were performed as well as a mathematical multilinear model was built to disclose the SBE variation determinants. RESULTS: We have shown that in septic shock patients the standard base excess variation during the first three days of ICU stay is weakly correlated to strong ion gap (SIG), lactate, creatinin and PaCO2 when individually analyzed. Analyzing concomitantly those independent variables, we built a mathematical model with a stepwise multilinear regression composed by apparent strong ion difference (SIDa), SIG, PaCO2, albumin and diuresis that resulted in a R² coefficient of 0.866 to determine SBE variation. CONCLUSIONS: Variations of metabolic acidosis measured through the standard base excess in septic shock patients when analyzed until the third day after intensive care unit admission, is resultant of interaction of several independent determinants as PaCO2, diuresis, SIG, SIDa and albumin.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):437-443
DOI 10.1590/S0103-507X2007000400006
BACKGROUND AND OBJECTIVES: The amount of metabolic acidosis measured through the standard base excess (SBE) has been shown to be an outcome marker and its improvement has been associated with better survival. We studied the mechanism of standard base excess variation in the first three days of intensive care unit (ICU) stay through the evaluation of independent variables of physico-chemical approach. METHODS: Data were retrieved from our prospective collected data base from patients with diagnosis of septic shock, daily up to the third day after the ICU admission. Single correlations between SBE and independent variables were performed as well as a mathematical multilinear model was built to disclose the SBE variation determinants. RESULTS: We have shown that in septic shock patients the standard base excess variation during the first three days of ICU stay is weakly correlated to strong ion gap (SIG), lactate, creatinin and PaCO2 when individually analyzed. Analyzing concomitantly those independent variables, we built a mathematical model with a stepwise multilinear regression composed by apparent strong ion difference (SIDa), SIG, PaCO2, albumin and diuresis that resulted in a R² coefficient of 0.866 to determine SBE variation. CONCLUSIONS: Variations of metabolic acidosis measured through the standard base excess in septic shock patients when analyzed until the third day after intensive care unit admission, is resultant of interaction of several independent determinants as PaCO2, diuresis, SIG, SIDa and albumin.