Oral hygiene Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2014;26(4):379-383
DOI 10.5935/0103-507X.20140058
To describe the oral health status of patients hospitalized in an intensive care unit.
Clinical assessment of the oral cavity was performed in 35 patients at two time-points (up to 48 hours after admission and 72 hours after the first assessment) and recorded in data collection forms. The following data were collected: plaque index, condition of the mucosa, presence or absence of dental prosthesis, number of teeth present, and tongue coating index.
The prevalence of nosocomial infection was 22% (eight patients), with 50% respiratory tract infections. All patients exhibited oral biofilm, and 20 (57%) showed biofilm visible to the naked eye; tongue coating was present on more than two thirds of the tongue in 24 patients (69%) and was thick in most cases. A significant increase in plaque index (p=0.007) occurred after 72 hours, although the tongue coating index was p<0.001 regarding the area and p=0.5 regarding the thickness.
The plaque and tongue coating indices increased with the length of hospital stay at the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):379-383
DOI 10.5935/0103-507X.20140058
To describe the oral health status of patients hospitalized in an intensive care unit.
Clinical assessment of the oral cavity was performed in 35 patients at two time-points (up to 48 hours after admission and 72 hours after the first assessment) and recorded in data collection forms. The following data were collected: plaque index, condition of the mucosa, presence or absence of dental prosthesis, number of teeth present, and tongue coating index.
The prevalence of nosocomial infection was 22% (eight patients), with 50% respiratory tract infections. All patients exhibited oral biofilm, and 20 (57%) showed biofilm visible to the naked eye; tongue coating was present on more than two thirds of the tongue in 24 patients (69%) and was thick in most cases. A significant increase in plaque index (p=0.007) occurred after 72 hours, although the tongue coating index was p<0.001 regarding the area and p=0.5 regarding the thickness.
The plaque and tongue coating indices increased with the length of hospital stay at the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2013;25(1):44-48
DOI 10.1590/S0103-507X2013000100009
OBJECTIVE: To evaluate the effectiveness of a tongue cleaner in the removal of tongue biofilm in mechanically ventilated patients. METHODS: Tongue biofilm and tracheal secretion samples were collected from a total of 50 patients: 27 in the study group (SG) who were intubated or tracheostomized under assisted ventilation and treated with the tongue cleaner and 23 in the control group (CG) who did not undergo tongue cleaning. Oral and tracheal secretion cultures of the SG (initially and after 5 days) and the CG (at a single time-point) were performed to evaluate the changes in bacterial flora. RESULTS: The median age of the SG patients was 77 years (45-99 years), and that of the CG patients was 79 years (21-94 years). The length of hospital stay ranged from 17-1,370 days for the SG with a median stay of 425 days and from 4-240 days for the CG with a median stay of 120 days. No significant differences were found when the dental plaque indexes were compared between the SG and the CG. There was no correlation between the index and the length of hospital stay. The same bacterial flora was found in the dental plaque of 9 of the 27 SG patients before and after the tongue scraper was used for 5 days compared with the CG (p=0.683). Overall, 7 of the 27 SG patients had positive bacterial cultures for the same strains in both tongue biofilm and tracheal secretions compared with the CG (p=0.003). Significant similarities in strain resistance and susceptibility of the assessed microorganisms were observed between oral and tracheal microflora in 6/23 cases in the CG (p=0.006). CONCLUSION: The use of a tongue cleaner is effective at reducing tongue biofilm in patients on mechanical ventilation and facilitates oral hygiene interventions performed by caregivers.
Abstract
Rev Bras Ter Intensiva. 2013;25(1):44-48
DOI 10.1590/S0103-507X2013000100009
OBJECTIVE: To evaluate the effectiveness of a tongue cleaner in the removal of tongue biofilm in mechanically ventilated patients. METHODS: Tongue biofilm and tracheal secretion samples were collected from a total of 50 patients: 27 in the study group (SG) who were intubated or tracheostomized under assisted ventilation and treated with the tongue cleaner and 23 in the control group (CG) who did not undergo tongue cleaning. Oral and tracheal secretion cultures of the SG (initially and after 5 days) and the CG (at a single time-point) were performed to evaluate the changes in bacterial flora. RESULTS: The median age of the SG patients was 77 years (45-99 years), and that of the CG patients was 79 years (21-94 years). The length of hospital stay ranged from 17-1,370 days for the SG with a median stay of 425 days and from 4-240 days for the CG with a median stay of 120 days. No significant differences were found when the dental plaque indexes were compared between the SG and the CG. There was no correlation between the index and the length of hospital stay. The same bacterial flora was found in the dental plaque of 9 of the 27 SG patients before and after the tongue scraper was used for 5 days compared with the CG (p=0.683). Overall, 7 of the 27 SG patients had positive bacterial cultures for the same strains in both tongue biofilm and tracheal secretions compared with the CG (p=0.003). Significant similarities in strain resistance and susceptibility of the assessed microorganisms were observed between oral and tracheal microflora in 6/23 cases in the CG (p=0.006). CONCLUSION: The use of a tongue cleaner is effective at reducing tongue biofilm in patients on mechanical ventilation and facilitates oral hygiene interventions performed by caregivers.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):369-374
DOI 10.1590/S0103-507X2012000400013
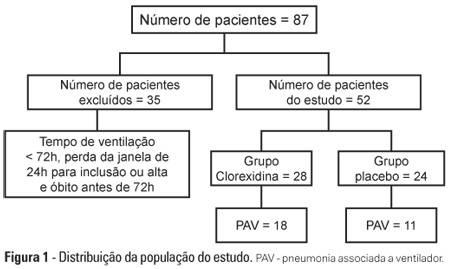
OBJECTIVE: To evaluate the effects of oral chlorhexidine hygiene with toothbrushing on the rate of ventilator-associated pneumonia in a mixed population of critically ill patients under prolonged mechanical ventilation. METHODS: Prospective, randomized, and placebo-controlled pilot study. Patients who were receiving mechanical ventilation, had been admitted less than 24 hours prior, and were anticipated to require mechanical ventilation for more than 72 hours were included in the study. The patients were randomly divided into one of the following groups: chlorhexidine hygiene with toothbrushing or a placebo group (gel with the same color and consistency and toothbrushing). RESULTS: The planned interim analysis was conducted using 52 patients, and the study was terminated prematurely. In total, 28 patients were included in the chlorhexidine / toothbrushing group, and 24 patients were included in the placebo group. Ventilator-associated pneumonia occurred in 45.8% of the placebo group and in 64.3% of the chlorhexidine hygiene with toothbrushing group (RR=1.4; 95% CI=0.83-2.34; p=0.29). CONCLUSION: Because the study was terminated due to futility, it was not possible to evaluate the impact of oral hygiene using 2% chlorhexidine and toothbrushing on the incidence of ventilator-associated pneumonia in this heterogeneous population of critical patients receiving long-term mechanical ventilation, and no beneficial effect was observed for this intervention.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):369-374
DOI 10.1590/S0103-507X2012000400013
OBJECTIVE: To evaluate the effects of oral chlorhexidine hygiene with toothbrushing on the rate of ventilator-associated pneumonia in a mixed population of critically ill patients under prolonged mechanical ventilation. METHODS: Prospective, randomized, and placebo-controlled pilot study. Patients who were receiving mechanical ventilation, had been admitted less than 24 hours prior, and were anticipated to require mechanical ventilation for more than 72 hours were included in the study. The patients were randomly divided into one of the following groups: chlorhexidine hygiene with toothbrushing or a placebo group (gel with the same color and consistency and toothbrushing). RESULTS: The planned interim analysis was conducted using 52 patients, and the study was terminated prematurely. In total, 28 patients were included in the chlorhexidine / toothbrushing group, and 24 patients were included in the placebo group. Ventilator-associated pneumonia occurred in 45.8% of the placebo group and in 64.3% of the chlorhexidine hygiene with toothbrushing group (RR=1.4; 95% CI=0.83-2.34; p=0.29). CONCLUSION: Because the study was terminated due to futility, it was not possible to evaluate the impact of oral hygiene using 2% chlorhexidine and toothbrushing on the incidence of ventilator-associated pneumonia in this heterogeneous population of critical patients receiving long-term mechanical ventilation, and no beneficial effect was observed for this intervention.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):38-44
DOI 10.1590/S0103-507X2009000100006
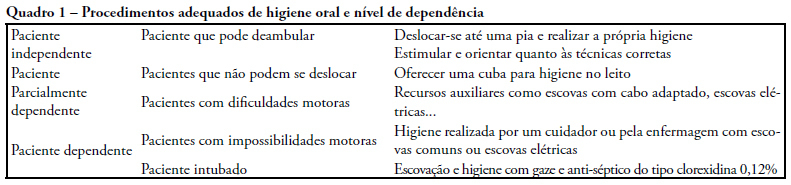
OBJECTIVES: A study was carried out, by means of a questionnaire for guided interviews seeking to establish a profile of perceptions and oral care given by ICU nursing team to patients in intensive care units. METHODS: The target population consisted of nursing practitioners divided in three education categories: nurses, nursing technicians and auxiliary nurses working at public and private hospital institutions providing for intensive care unit patients in Belem-PA. Dentistry experience has developed in this field reporting scientific findings and practical applications on prevention and reestablishment of the oral health in question. RESULTS: This survey disclosed results suggesting that oral hygiene care given to intensive care units patients is insufficient and inadequate requiring changes be made in the care now provided in the nosocomial environment by the nursing team. CONCLUSION: Presence of a dentist, knowledge of preventive dentistry, dissemination and use of oral hygiene specific resources are means suggested in an attempt to resolve difficulties found in oral health maintenance and treatment of oral diseases that affect the general health of hospitalized individuals. Interdisciplinary action for these individuals is advocated to achieve a better quality of life by preventing or minimizing oral pathologies.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):38-44
DOI 10.1590/S0103-507X2009000100006
OBJECTIVES: A study was carried out, by means of a questionnaire for guided interviews seeking to establish a profile of perceptions and oral care given by ICU nursing team to patients in intensive care units. METHODS: The target population consisted of nursing practitioners divided in three education categories: nurses, nursing technicians and auxiliary nurses working at public and private hospital institutions providing for intensive care unit patients in Belem-PA. Dentistry experience has developed in this field reporting scientific findings and practical applications on prevention and reestablishment of the oral health in question. RESULTS: This survey disclosed results suggesting that oral hygiene care given to intensive care units patients is insufficient and inadequate requiring changes be made in the care now provided in the nosocomial environment by the nursing team. CONCLUSION: Presence of a dentist, knowledge of preventive dentistry, dissemination and use of oral hygiene specific resources are means suggested in an attempt to resolve difficulties found in oral health maintenance and treatment of oral diseases that affect the general health of hospitalized individuals. Interdisciplinary action for these individuals is advocated to achieve a better quality of life by preventing or minimizing oral pathologies.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):412-417
DOI 10.1590/S0103-507X2006000400016
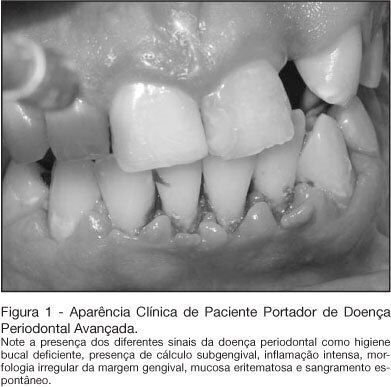
BACKGROUND AND OBJECTIVES: In the intensive care unit, the nosocomial respiratory infection is responsible for high rates of morbidity, mortality and expressive increase in hospitals costs. Its establishment feels more commonly by the aspiration of the content present within the mouth and the pharynx. Thus we intended to review the literature on the participation of the oral condition in the establishment of the nosocomial respiratory infection. CONTENTS: Deficient oral hygiene is common in patients under intensive care, which provides the colonization of oral biofilm for pathogenic microorganisms, especially for respiratory pathogens. The studies clearly show that the amount of oral biofilm in patients under intensive care increases according to period hospitalization meanwhile there also is an increase in respiratory pathogens. That colonizes the oral biofilm. This biofilm is an important resource of pathogens in patients under intensive care. CONCLUSIONS: In spite of well-established hypotheses that narrow down the relationships between lung infections and the oral condition, the studies are not still completely defined. However, due to strong possibilities that these hypotheses are true, it is necessary to have and maintain the oral health, in addition to more integration of dentistry and of Medicine, seeking patients' global treatment, the prevention of diseases, and more humanization at the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):412-417
DOI 10.1590/S0103-507X2006000400016
BACKGROUND AND OBJECTIVES: In the intensive care unit, the nosocomial respiratory infection is responsible for high rates of morbidity, mortality and expressive increase in hospitals costs. Its establishment feels more commonly by the aspiration of the content present within the mouth and the pharynx. Thus we intended to review the literature on the participation of the oral condition in the establishment of the nosocomial respiratory infection. CONTENTS: Deficient oral hygiene is common in patients under intensive care, which provides the colonization of oral biofilm for pathogenic microorganisms, especially for respiratory pathogens. The studies clearly show that the amount of oral biofilm in patients under intensive care increases according to period hospitalization meanwhile there also is an increase in respiratory pathogens. That colonizes the oral biofilm. This biofilm is an important resource of pathogens in patients under intensive care. CONCLUSIONS: In spite of well-established hypotheses that narrow down the relationships between lung infections and the oral condition, the studies are not still completely defined. However, due to strong possibilities that these hypotheses are true, it is necessary to have and maintain the oral health, in addition to more integration of dentistry and of Medicine, seeking patients' global treatment, the prevention of diseases, and more humanization at the intensive care unit.