Conscious sedation Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(4):426-432
DOI 10.5935/0103-507X.20220278-en
To characterize the knowledge and perceived attitudes toward pharmacologic interventions for light sedation in mechanically ventilated patients and to understand the current gaps comparing current practice with the recommendations of the Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the Intensive Care Unit.
This was a cross-sectional cohort study based on the application of an electronic questionnaire focused on sedation practices.
A total of 303 critical care physicians provided responses to the survey. Most respondents reported routine use of a structured sedation scale (281; 92.6%). Almost half of the respondents reported performing daily interruptions of sedation (147; 48.4%), and the same percentage of participants (48.0%) agreed that patients are often over sedated. During the COVID-19 pandemic, participants reported that patients had a higher chance of receiving midazolam compared to before the pandemic (178; 58.8% versus 106; 34.0%; p = 0.05), and heavy sedation was more common during the COVID-19 pandemic (241; 79.4% versus 148; 49.0%; p = 0.01).
This survey provides valuable data on the perceived attitudes of Brazilian intensive care physicians regarding sedation. Although daily interruption of sedation was a well-known concept and sedation scales were often used by the respondents, insufficient effort was put into frequent monitoring, use of protocols and systematic implementation of sedation strategies. Despite the perception of the benefits linked with light sedation, there is a need to identify improvement targets to propose educational strategies to improve current practices.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):426-432
DOI 10.5935/0103-507X.20220278-en
To characterize the knowledge and perceived attitudes toward pharmacologic interventions for light sedation in mechanically ventilated patients and to understand the current gaps comparing current practice with the recommendations of the Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the Intensive Care Unit.
This was a cross-sectional cohort study based on the application of an electronic questionnaire focused on sedation practices.
A total of 303 critical care physicians provided responses to the survey. Most respondents reported routine use of a structured sedation scale (281; 92.6%). Almost half of the respondents reported performing daily interruptions of sedation (147; 48.4%), and the same percentage of participants (48.0%) agreed that patients are often over sedated. During the COVID-19 pandemic, participants reported that patients had a higher chance of receiving midazolam compared to before the pandemic (178; 58.8% versus 106; 34.0%; p = 0.05), and heavy sedation was more common during the COVID-19 pandemic (241; 79.4% versus 148; 49.0%; p = 0.01).
This survey provides valuable data on the perceived attitudes of Brazilian intensive care physicians regarding sedation. Although daily interruption of sedation was a well-known concept and sedation scales were often used by the respondents, insufficient effort was put into frequent monitoring, use of protocols and systematic implementation of sedation strategies. Despite the perception of the benefits linked with light sedation, there is a need to identify improvement targets to propose educational strategies to improve current practices.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):102-110
DOI 10.5935/0103-507X.20210011
To perform a cross-cultural adaptation of the Richmond Agitation-Sedation Scale (RASS) to Brazilian Portuguese for the evaluation of sedation in pediatric intensive care.
Cross-cultural adaptation process including the conceptual, item, semantic and operational equivalence stages according to current recommendations.
Pretests, divided into two stages, included 30 professionals from the pediatric intensive care unit of a university hospital, who administered the translated RASS to patients aged 29 days to 18 years. The pretests showed a content validity index above 0.90 for all items: 0.97 in the first stage of pretests and 0.99 in the second.
The cross-cultural adaptation of RASS to Brazilian Portuguese resulted in a version with excellent comprehensibility and acceptability in a pediatric intensive care setting. Reliability and validity studies should be performed to evaluate the psychometric properties of the Brazilian Portuguese version of the RASS.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):102-110
DOI 10.5935/0103-507X.20210011
To perform a cross-cultural adaptation of the Richmond Agitation-Sedation Scale (RASS) to Brazilian Portuguese for the evaluation of sedation in pediatric intensive care.
Cross-cultural adaptation process including the conceptual, item, semantic and operational equivalence stages according to current recommendations.
Pretests, divided into two stages, included 30 professionals from the pediatric intensive care unit of a university hospital, who administered the translated RASS to patients aged 29 days to 18 years. The pretests showed a content validity index above 0.90 for all items: 0.97 in the first stage of pretests and 0.99 in the second.
The cross-cultural adaptation of RASS to Brazilian Portuguese resulted in a version with excellent comprehensibility and acceptability in a pediatric intensive care setting. Reliability and validity studies should be performed to evaluate the psychometric properties of the Brazilian Portuguese version of the RASS.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):318-325
DOI 10.5935/0103-507X.20190057
To validate the "Checklist for Managing Critical Patients' Daily Awakening" instrument.
This was a descriptive study that used a quantitative approach for content validation using the Delphi method to obtain the consensus of experts who evaluated the instrument using a Likert scale. The validity index of each item of the instrument was calculated, with a minimum consensus parameter above 0.78.
Three Delphi rounds were required, starting with 29 experts and ending with 15 experts who were invited in person and via e-mail to participate in the study. Of the 15 items in the instrument, 13 had a content validity index > 0.78. The instrument maintained its attributes, and six items were reformulated without the need to exclude any of them. The validated items enabled the assessment of and decisions regarding the dimensions related to the level of sedation and agitation, vital signs, ventilatory parameters and pain. The instrument presented psychometric indicators with acceptable content validity.
The instrument proposed in the study exhibited content validity for most of its items and emerges as a practical strategy for the management of the daily interruption of sedation of critical patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):318-325
DOI 10.5935/0103-507X.20190057
To validate the "Checklist for Managing Critical Patients' Daily Awakening" instrument.
This was a descriptive study that used a quantitative approach for content validation using the Delphi method to obtain the consensus of experts who evaluated the instrument using a Likert scale. The validity index of each item of the instrument was calculated, with a minimum consensus parameter above 0.78.
Three Delphi rounds were required, starting with 29 experts and ending with 15 experts who were invited in person and via e-mail to participate in the study. Of the 15 items in the instrument, 13 had a content validity index > 0.78. The instrument maintained its attributes, and six items were reformulated without the need to exclude any of them. The validated items enabled the assessment of and decisions regarding the dimensions related to the level of sedation and agitation, vital signs, ventilatory parameters and pain. The instrument presented psychometric indicators with acceptable content validity.
The instrument proposed in the study exhibited content validity for most of its items and emerges as a practical strategy for the management of the daily interruption of sedation of critical patients.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):444-451
DOI 10.5935/0103-507X.20160078
The aim of this study was to systematically review studies that compared a mild target sedation protocol with daily sedation interruption and to perform a meta-analysis with the data presented in these studies.
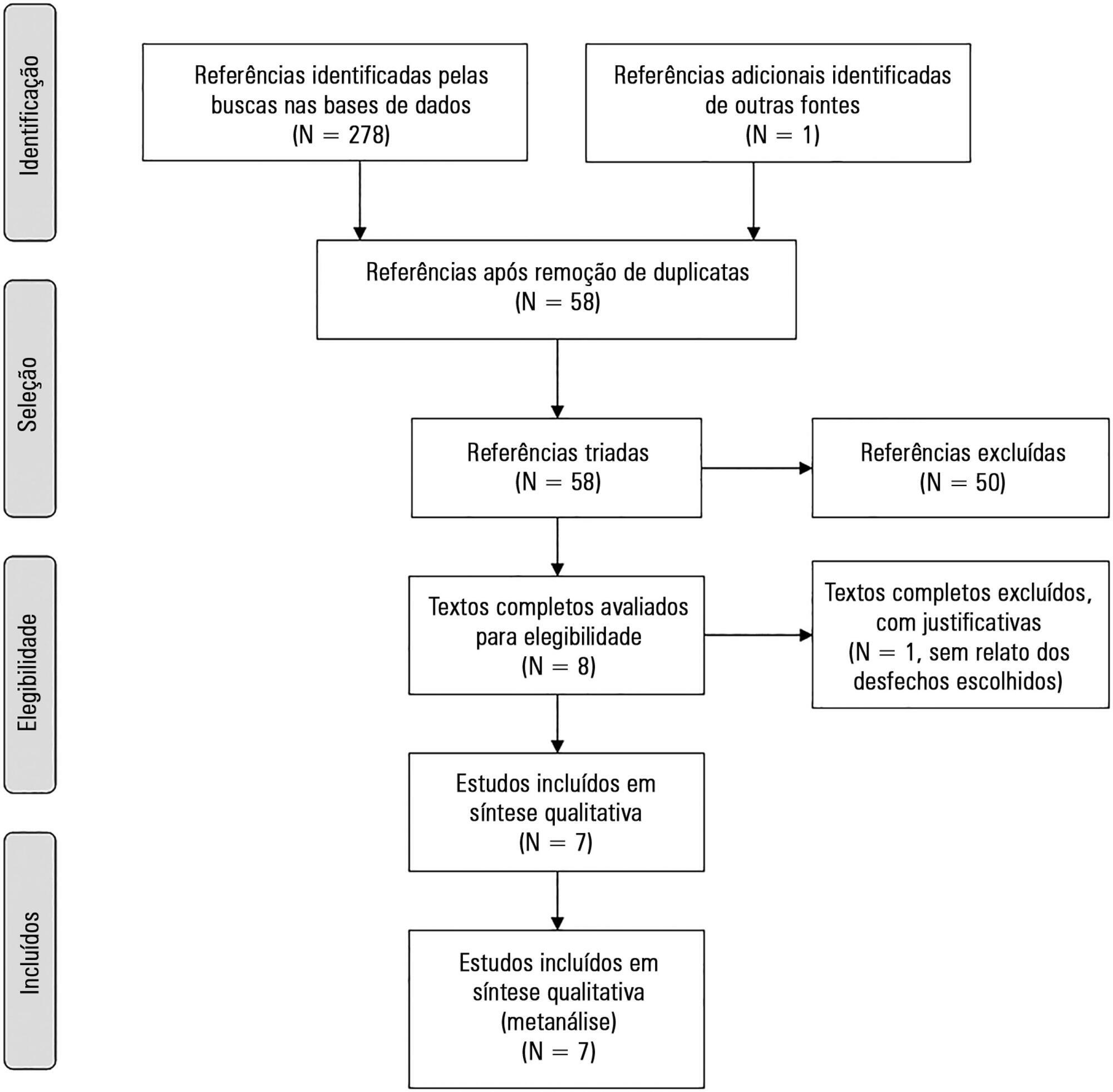
We searched Medline, Scopus and Web of Science databases to identify randomized clinical trials comparing sedation protocols with daily sedation interruption in critically ill patients requiring mechanical ventilation. The primary outcome was mortality in the intensive care unit.
Seven studies were included, with a total of 892 patients. Mortality in the intensive care unit did not differ between the sedation protocol and daily sedation interruption groups (odds ratio [OR] = 0.81; 95% confidence interval [CI] 0.60 - 1.10; I2 = 0%). Hospital mortality, duration of mechanical ventilation, intensive care unit and hospital length of stay did not differ between the groups either. Sedation protocols were associated with an increase in the number of days free of mechanical ventilation (mean difference = 6.70 days; 95%CI 1.09 - 12.31 days; I2 = 87.2%) and a shorter duration of hospital length of stay (mean difference = -5.05 days, 95%CI -9.98 - -0.11 days; I2 = 69%). There were no differences in regard to accidental extubation, extubation failure and the occurrence of delirium.
Sedation protocols and daily sedation interruption do not appear to differ in regard to the majority of analyzed outcomes. The only differences found were small and had a high degree of heterogeneity.
Abstract
Rev Bras Ter Intensiva. 2016;28(4):444-451
DOI 10.5935/0103-507X.20160078
The aim of this study was to systematically review studies that compared a mild target sedation protocol with daily sedation interruption and to perform a meta-analysis with the data presented in these studies.
We searched Medline, Scopus and Web of Science databases to identify randomized clinical trials comparing sedation protocols with daily sedation interruption in critically ill patients requiring mechanical ventilation. The primary outcome was mortality in the intensive care unit.
Seven studies were included, with a total of 892 patients. Mortality in the intensive care unit did not differ between the sedation protocol and daily sedation interruption groups (odds ratio [OR] = 0.81; 95% confidence interval [CI] 0.60 - 1.10; I2 = 0%). Hospital mortality, duration of mechanical ventilation, intensive care unit and hospital length of stay did not differ between the groups either. Sedation protocols were associated with an increase in the number of days free of mechanical ventilation (mean difference = 6.70 days; 95%CI 1.09 - 12.31 days; I2 = 87.2%) and a shorter duration of hospital length of stay (mean difference = -5.05 days, 95%CI -9.98 - -0.11 days; I2 = 69%). There were no differences in regard to accidental extubation, extubation failure and the occurrence of delirium.
Sedation protocols and daily sedation interruption do not appear to differ in regard to the majority of analyzed outcomes. The only differences found were small and had a high degree of heterogeneity.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):306-311
DOI 10.5935/0103-507X.20130052
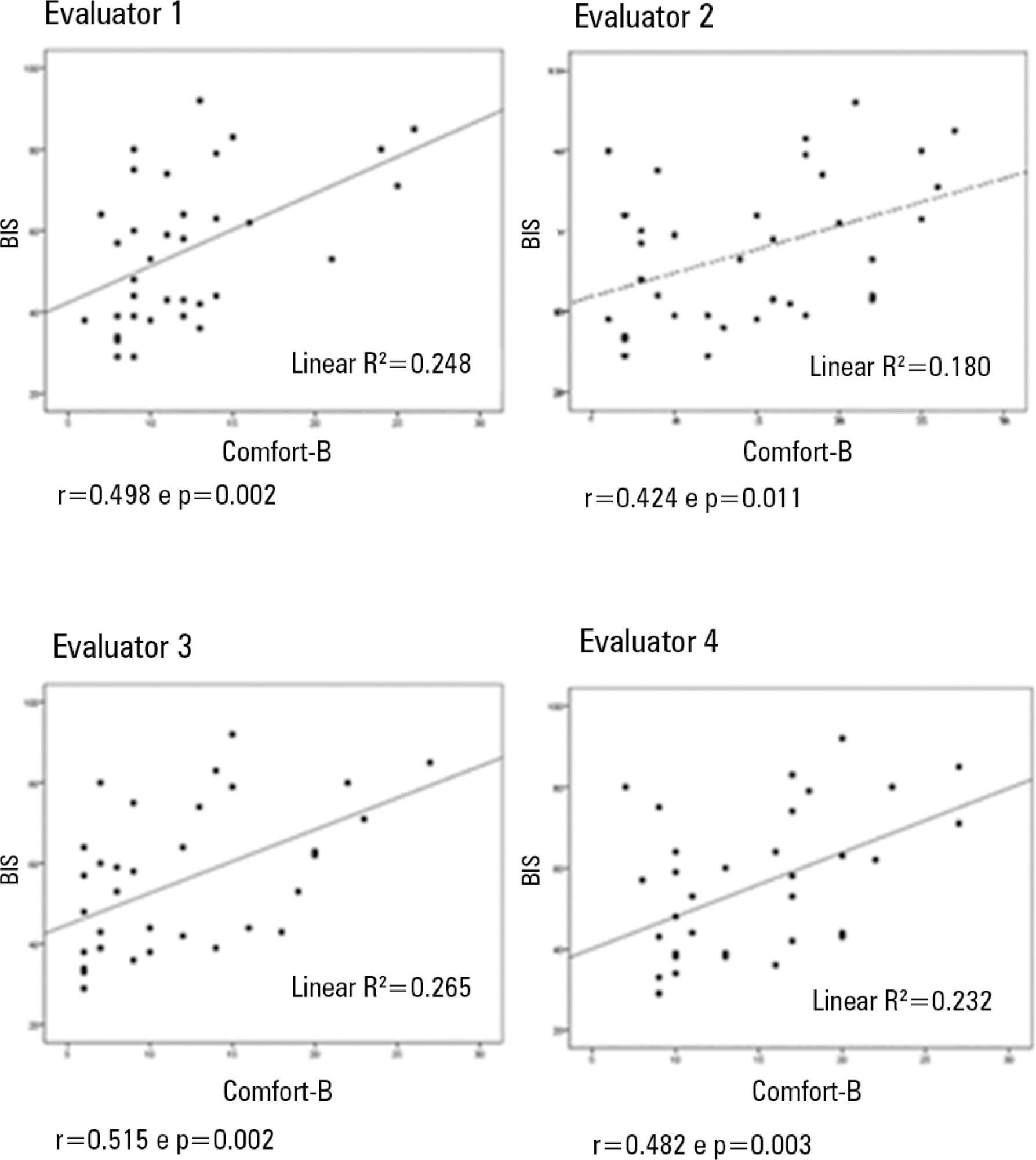
Compare the scores resulting from the Comfort-B scale with the bispectral index in children in an intensive care unit.
Eleven children between the ages of 1 month and 16 years requiring mechanical ventilation and sedation were simultaneously classified based on the bispectral index and the Comfort-B scale. Their behavior was recorded using digital photography, and the record was later evaluated by three independent evaluators. Agreement tests (Bland-Altman and Kappa) were then performed. The correlation between the two methods (Pearson correlation) was tested.
In total, 35 observations were performed on 11 patients. Based on the Kappa coefficient, the agreement among evaluators ranged from 0.56 to 0.75 (p<0.001). There was a positive and consistent association between the bispectral index and the Comfort-B scale [r=0.424 (p=0.011) to r=0.498 (p=0.002)].
Due to the strong correlation between the independent evaluators and the consistent correlation between the two methods, the results suggest that the Comfort-B scale is reproducible and useful in classifying the level of sedation in children requiring mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):306-311
DOI 10.5935/0103-507X.20130052
Compare the scores resulting from the Comfort-B scale with the bispectral index in children in an intensive care unit.
Eleven children between the ages of 1 month and 16 years requiring mechanical ventilation and sedation were simultaneously classified based on the bispectral index and the Comfort-B scale. Their behavior was recorded using digital photography, and the record was later evaluated by three independent evaluators. Agreement tests (Bland-Altman and Kappa) were then performed. The correlation between the two methods (Pearson correlation) was tested.
In total, 35 observations were performed on 11 patients. Based on the Kappa coefficient, the agreement among evaluators ranged from 0.56 to 0.75 (p<0.001). There was a positive and consistent association between the bispectral index and the Comfort-B scale [r=0.424 (p=0.011) to r=0.498 (p=0.002)].
Due to the strong correlation between the independent evaluators and the consistent correlation between the two methods, the results suggest that the Comfort-B scale is reproducible and useful in classifying the level of sedation in children requiring mechanical ventilation.