Case reports Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2015;27(4):402-405
DOI 10.5935/0103-507X.20150067
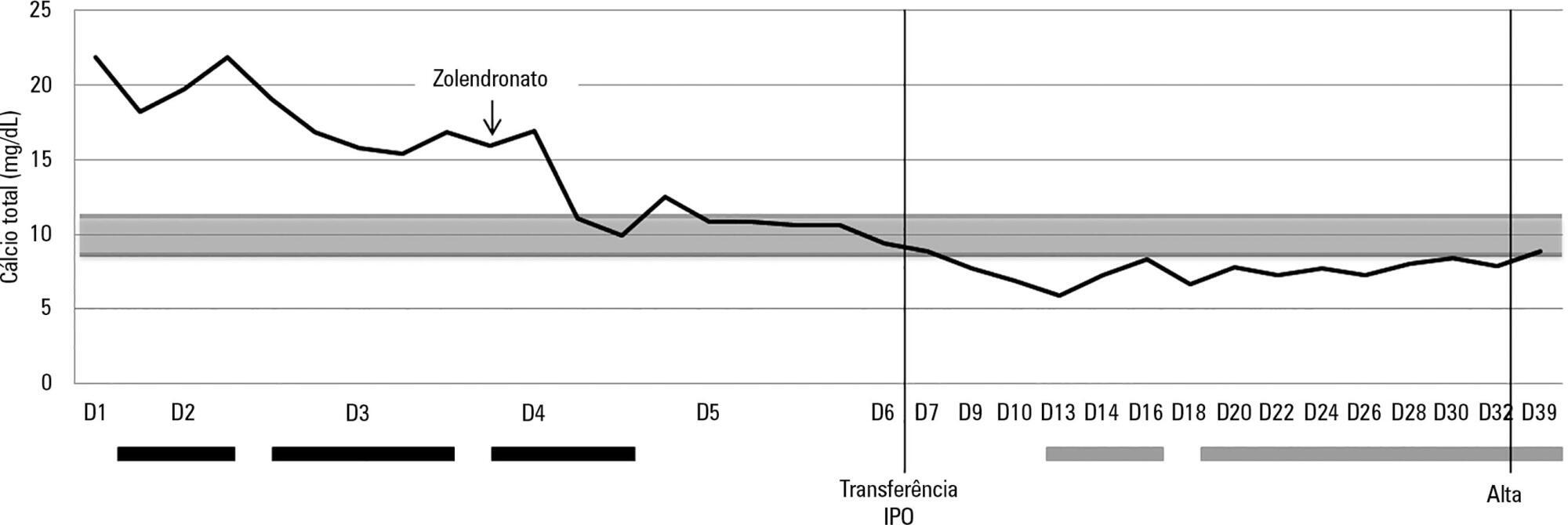
Hypercalcemia is a rare metabolic disorder in children and is potentially fatal. It has a wide differential diagnosis, including cancer. Here, we report the case of a previously healthy 3-year-old who was admitted to the emergency room with fatigue, hyporeactivity, fever and limping gait that had evolved over 5 days and that was progressively worsening. On examination the patient was unconscious (Glasgow coma score: 8). Laboratory tests indicated severe hypercalcemia (total calcium 21.39mg/dL, ionized calcium 2.93mmol/L) and microcytic anemia. Hyperhydration was initiated, and the child was transferred to the pediatric intensive care unit. Continuous venovenous hemodiafiltration with calcium-free solution was instituted, which brought progressive normalization of serum calcium and an improved state of consciousness. Zoledronate was administered, and metabolic and infectious causes and poisoning were excluded. The bone marrow smear revealed a diagnosis of acute lymphoblastic leukemia. Hypercalcemia associated with malignancy in children is rare and occurs as a form of cancer presentation or recurrence. Continuous venovenous hemodiafiltration should be considered in situations where there is imminent risk to life.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):402-405
DOI 10.5935/0103-507X.20150067
Hypercalcemia is a rare metabolic disorder in children and is potentially fatal. It has a wide differential diagnosis, including cancer. Here, we report the case of a previously healthy 3-year-old who was admitted to the emergency room with fatigue, hyporeactivity, fever and limping gait that had evolved over 5 days and that was progressively worsening. On examination the patient was unconscious (Glasgow coma score: 8). Laboratory tests indicated severe hypercalcemia (total calcium 21.39mg/dL, ionized calcium 2.93mmol/L) and microcytic anemia. Hyperhydration was initiated, and the child was transferred to the pediatric intensive care unit. Continuous venovenous hemodiafiltration with calcium-free solution was instituted, which brought progressive normalization of serum calcium and an improved state of consciousness. Zoledronate was administered, and metabolic and infectious causes and poisoning were excluded. The bone marrow smear revealed a diagnosis of acute lymphoblastic leukemia. Hypercalcemia associated with malignancy in children is rare and occurs as a form of cancer presentation or recurrence. Continuous venovenous hemodiafiltration should be considered in situations where there is imminent risk to life.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):397-401
DOI 10.5935/0103-507X.20150066
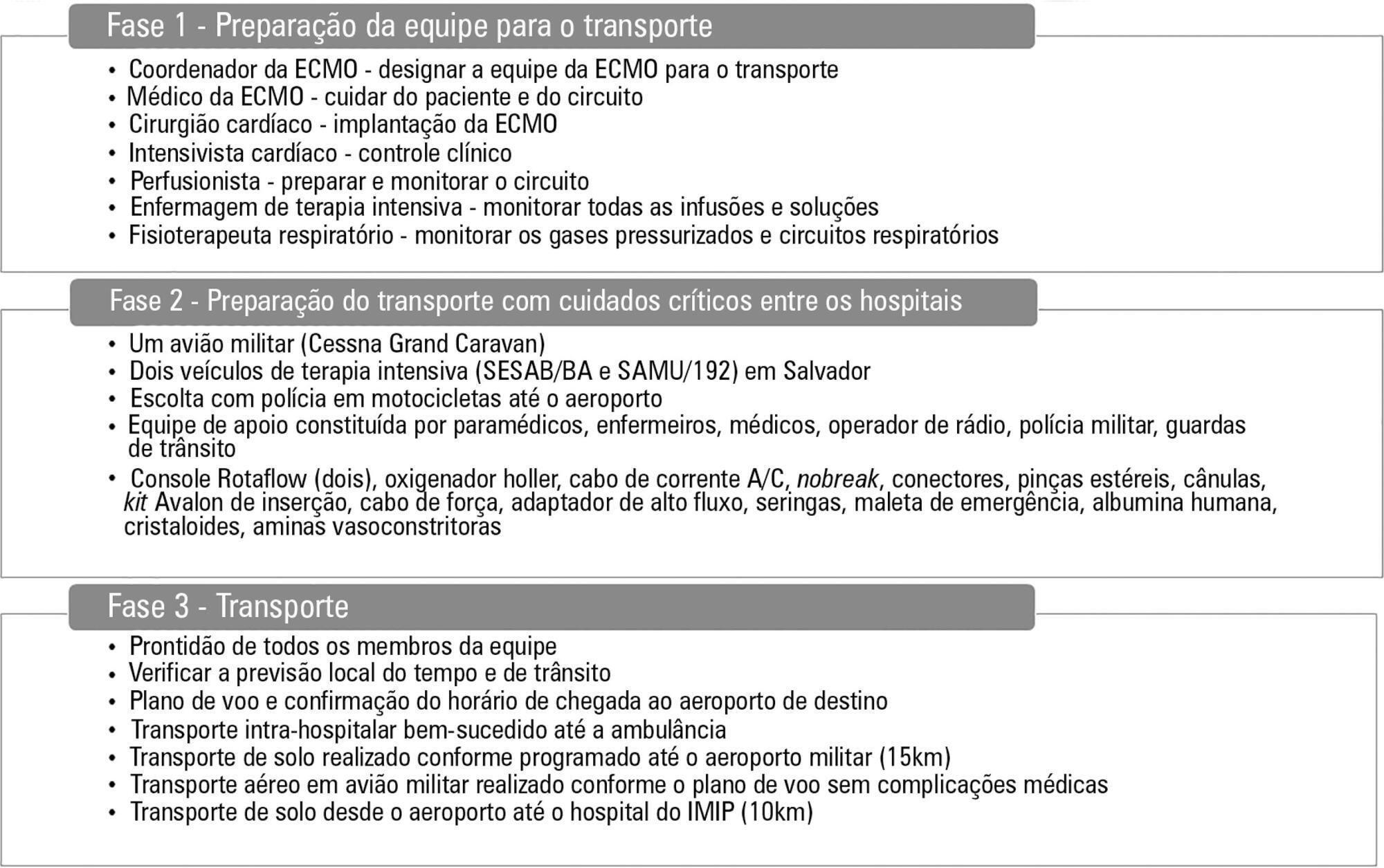
A 17-year-old Brazilian male presented with progressive dyspnea for 15 days, worsening in the last 24 hours, and was admitted in respiratory failure and cardiogenic shock, with multiple organ dysfunctions. Echocardiography showed a left ventricle ejection fraction of 11%, severe diffuse hypokinesia, and a systolic pulmonary artery pressure of 50mmHg, resulting in the need for hemodynamic support with dobutamine (20mcg/kg/min) and noradrenaline (1.7mcg/kg/min). After 48 hours with no clinical or hemodynamic improvement, an extracorporeal membrane oxygenation was implanted. The patient presented with hemodynamic, systemic perfusion and renal and liver function improvements; however, his cardiac function did not recover after 72 hours, and he was transfer to another hospital. Air transport was conducted from Salvador to Recife in Brazil. A heart transplant was performed with rapid recovery of both liver and kidney functions, as well as good graft function. Histopathology of the explanted heart showed chronic active myocarditis and amastigotes of Trypanosoma cruzi. The estimated global prevalence of T. cruzi infections declined from 18 million in 1991, when the first regional control initiative began, to 5.7 million in 2010. Myocarditis is an inflammatory disease due to infectious or non-infectious conditions. Clinical manifestation is variable, ranging from subclinical presentation to refractory heart failure and cardiogenic shock. Several reports suggest that the use of extracorporeal membrane oxygenation in patients presenting with severe refractory myocarditis is a potential bridging therapy to heart transplant when there is no spontaneous recovery of ventricular function. In a 6-month follow-up outpatient consult, the patient presented well and was asymptomatic.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):397-401
DOI 10.5935/0103-507X.20150066
A 17-year-old Brazilian male presented with progressive dyspnea for 15 days, worsening in the last 24 hours, and was admitted in respiratory failure and cardiogenic shock, with multiple organ dysfunctions. Echocardiography showed a left ventricle ejection fraction of 11%, severe diffuse hypokinesia, and a systolic pulmonary artery pressure of 50mmHg, resulting in the need for hemodynamic support with dobutamine (20mcg/kg/min) and noradrenaline (1.7mcg/kg/min). After 48 hours with no clinical or hemodynamic improvement, an extracorporeal membrane oxygenation was implanted. The patient presented with hemodynamic, systemic perfusion and renal and liver function improvements; however, his cardiac function did not recover after 72 hours, and he was transfer to another hospital. Air transport was conducted from Salvador to Recife in Brazil. A heart transplant was performed with rapid recovery of both liver and kidney functions, as well as good graft function. Histopathology of the explanted heart showed chronic active myocarditis and amastigotes of Trypanosoma cruzi. The estimated global prevalence of T. cruzi infections declined from 18 million in 1991, when the first regional control initiative began, to 5.7 million in 2010. Myocarditis is an inflammatory disease due to infectious or non-infectious conditions. Clinical manifestation is variable, ranging from subclinical presentation to refractory heart failure and cardiogenic shock. Several reports suggest that the use of extracorporeal membrane oxygenation in patients presenting with severe refractory myocarditis is a potential bridging therapy to heart transplant when there is no spontaneous recovery of ventricular function. In a 6-month follow-up outpatient consult, the patient presented well and was asymptomatic.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):185-189
DOI 10.5935/0103-507X.20150031
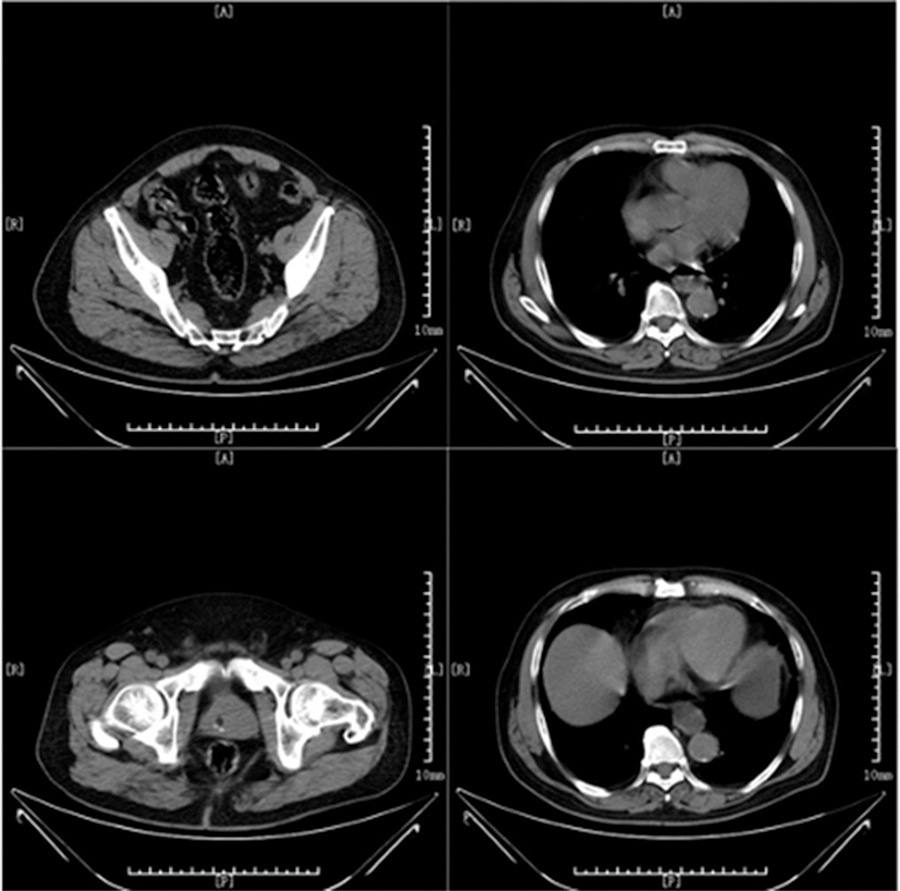
This is a case report of a 43-year-old Caucasian male with end-stage renal disease being treated with hemodialysis and infective endocarditis in the aortic and tricuspid valves. The clinical presentation was dominated by neurologic impairment with cerebral embolism and hemorrhagic components. A thoracoabdominal computerized tomography scan revealed septic pulmonary embolus. The patient underwent empirical antibiotherapy with ceftriaxone, gentamicin and vancomycin, and the therapy was changed to flucloxacilin and gentamicin after the isolation of S. aureus in blood cultures. The multidisciplinary team determined that the patient should undergo valve replacement after the stabilization of the intracranial hemorrhage; however, on the 8th day of hospitalization, the patient entered cardiac arrest due to a massive septic pulmonary embolism and died. Despite the risk of aggravation of the hemorrhagic cerebral lesion, early surgical intervention should be considered in high-risk patients.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):185-189
DOI 10.5935/0103-507X.20150031
This is a case report of a 43-year-old Caucasian male with end-stage renal disease being treated with hemodialysis and infective endocarditis in the aortic and tricuspid valves. The clinical presentation was dominated by neurologic impairment with cerebral embolism and hemorrhagic components. A thoracoabdominal computerized tomography scan revealed septic pulmonary embolus. The patient underwent empirical antibiotherapy with ceftriaxone, gentamicin and vancomycin, and the therapy was changed to flucloxacilin and gentamicin after the isolation of S. aureus in blood cultures. The multidisciplinary team determined that the patient should undergo valve replacement after the stabilization of the intracranial hemorrhage; however, on the 8th day of hospitalization, the patient entered cardiac arrest due to a massive septic pulmonary embolism and died. Despite the risk of aggravation of the hemorrhagic cerebral lesion, early surgical intervention should be considered in high-risk patients.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):412-415
DOI 10.5935/0103-507X.20150069
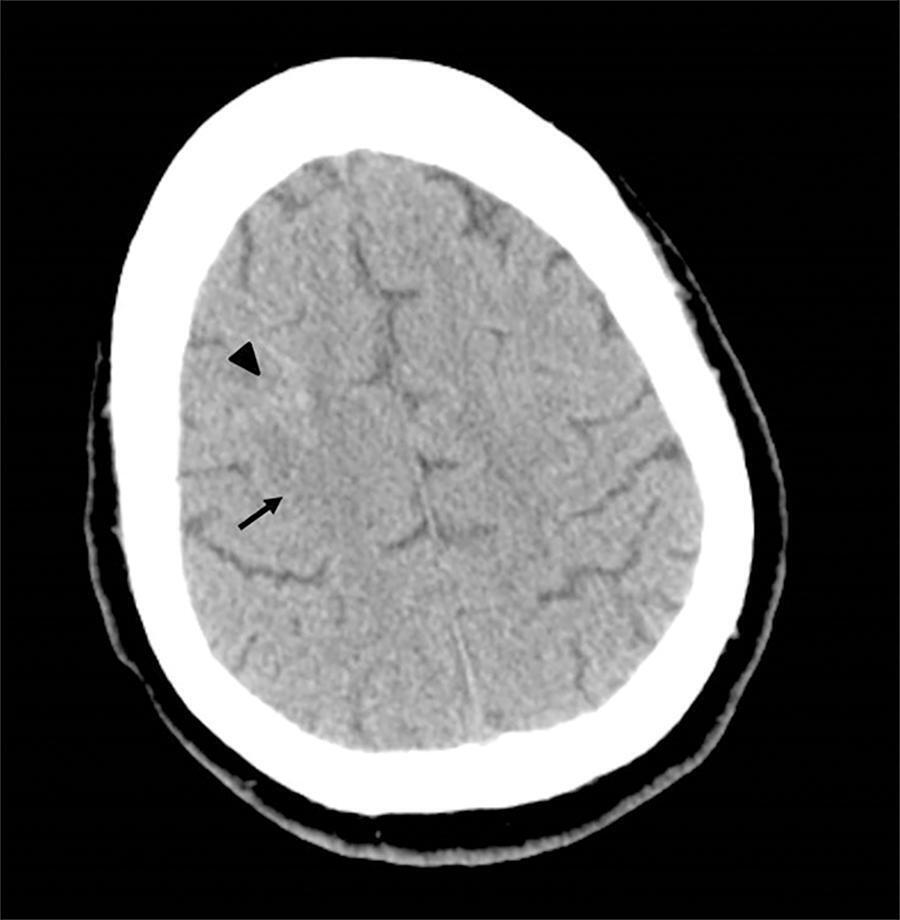
We report the case of a 2-year-old child who survived an acute episode of severe spontaneous intracranial hemorrhage with clinical and radiological signs of intracranial hypertension and transtentorial herniation. The patient underwent emergency surgery to drain the hematoma, and a catheter was inserted to monitor intracranial pressure. In the initial computed tomography analysis performed prior to hematoma drainage, a brain cyst was evident contralateral to the hematoma, which, based on the analysis by the care team, possibly helped to avoid a worse outcome because the cyst accommodated the brain after the massive hemorrhage. After the investigation, the patient was determined to have previously undiagnosed hemophilia A. The patient underwent treatment in intensive care, which included the control of intracranial pressure, factor VIII replacement and discharge without signs of neurological impairment.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):412-415
DOI 10.5935/0103-507X.20150069
We report the case of a 2-year-old child who survived an acute episode of severe spontaneous intracranial hemorrhage with clinical and radiological signs of intracranial hypertension and transtentorial herniation. The patient underwent emergency surgery to drain the hematoma, and a catheter was inserted to monitor intracranial pressure. In the initial computed tomography analysis performed prior to hematoma drainage, a brain cyst was evident contralateral to the hematoma, which, based on the analysis by the care team, possibly helped to avoid a worse outcome because the cyst accommodated the brain after the massive hemorrhage. After the investigation, the patient was determined to have previously undiagnosed hemophilia A. The patient underwent treatment in intensive care, which included the control of intracranial pressure, factor VIII replacement and discharge without signs of neurological impairment.

Abstract
Rev Bras Ter Intensiva. 2015;27(4):406-411
DOI 10.5935/0103-507X.20150068
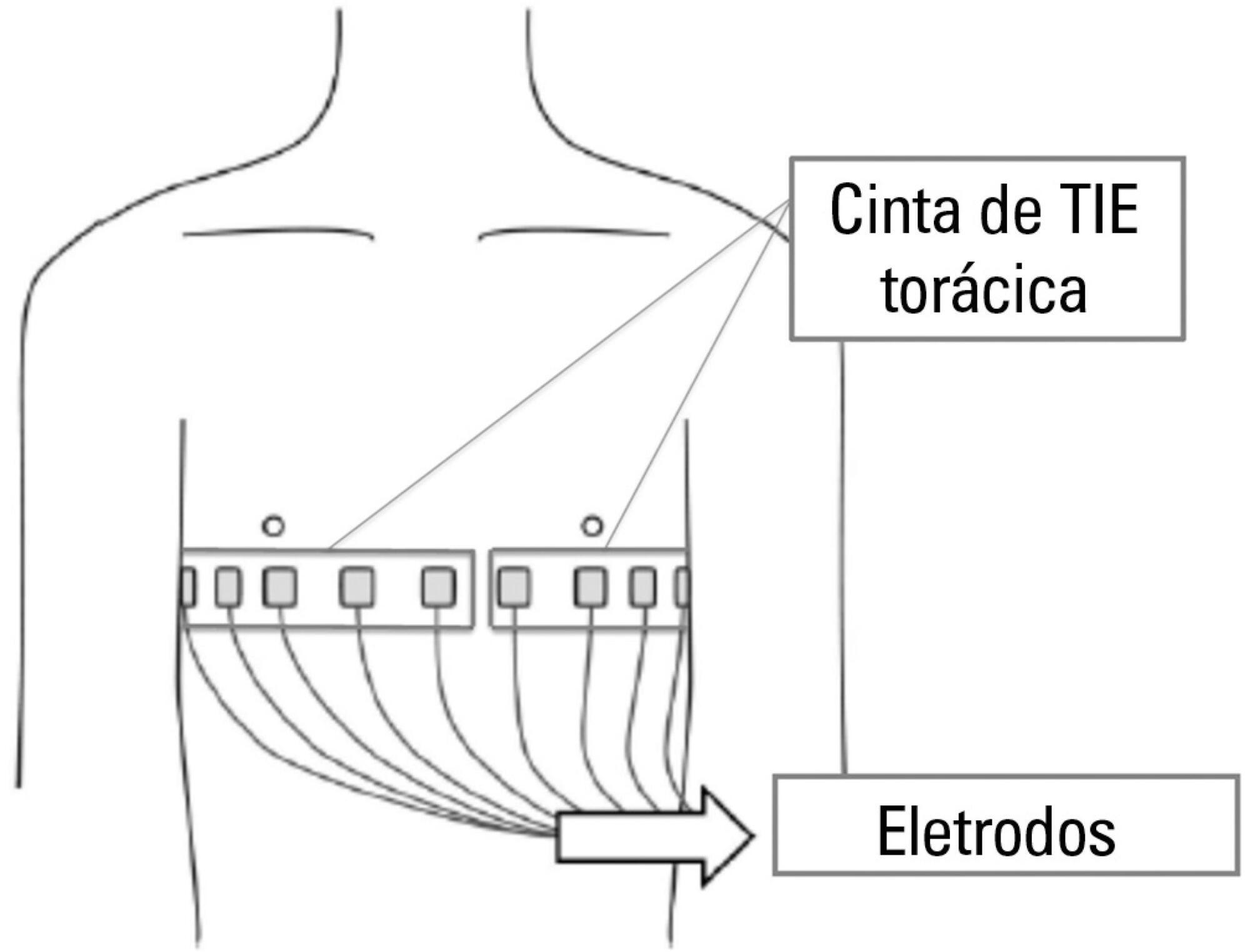
Thoracic electrical impedance tomography is a real-time, noninvasive monitoring tool of the regional pulmonary ventilation distribution. Its bedside use in patients with acute respiratory distress syndrome has the potential to aid in alveolar recruitment maneuvers, which are often necessary in cases of refractory hypoxemia. In this case report, we describe the monitoring results and interpretation of thoracic electrical impedance tomography used during alveolar recruitment maneuvers in a patient with acute respiratory distress syndrome, with transient application of high alveolar pressures and optimal positive end-expiratory pressure titration. Furthermore, we provide a brief literature review regarding the use of alveolar recruitment maneuvers and monitoring using thoracic electrical impedance tomography in patients with acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):406-411
DOI 10.5935/0103-507X.20150068
Thoracic electrical impedance tomography is a real-time, noninvasive monitoring tool of the regional pulmonary ventilation distribution. Its bedside use in patients with acute respiratory distress syndrome has the potential to aid in alveolar recruitment maneuvers, which are often necessary in cases of refractory hypoxemia. In this case report, we describe the monitoring results and interpretation of thoracic electrical impedance tomography used during alveolar recruitment maneuvers in a patient with acute respiratory distress syndrome, with transient application of high alveolar pressures and optimal positive end-expiratory pressure titration. Furthermore, we provide a brief literature review regarding the use of alveolar recruitment maneuvers and monitoring using thoracic electrical impedance tomography in patients with acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):407-409
DOI 10.5935/0103-507X.20140062
Haff disease is a syndrome consisting of unexplained rhabdomyolysis. Patients suffering from Haff disease report having eaten fish within 24 hours before the onset of illness. Most patients survive and recover quickly. The present study is the first report of Haff disease complicated by multiple organ failure after crayfish consumption. A 66-year-old Chinese man ate cooked crayfish on the night of June 23, 2013. He arrived at our hospital 2 days later and was admitted to the intensive care unit. After admission, the patient was diagnosed with Haff disease complicated by multiple organ failure. Despite supportive and symptomatic treatments, the condition of the patient deteriorated, and he died due to his illness.
Haff disease is a rare clinical syndrome that is sometimes misdiagnosed. Early diagnosis and proper treatment are essential to prevent progression to multiple organ failure.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):407-409
DOI 10.5935/0103-507X.20140062
Haff disease is a syndrome consisting of unexplained rhabdomyolysis. Patients suffering from Haff disease report having eaten fish within 24 hours before the onset of illness. Most patients survive and recover quickly. The present study is the first report of Haff disease complicated by multiple organ failure after crayfish consumption. A 66-year-old Chinese man ate cooked crayfish on the night of June 23, 2013. He arrived at our hospital 2 days later and was admitted to the intensive care unit. After admission, the patient was diagnosed with Haff disease complicated by multiple organ failure. Despite supportive and symptomatic treatments, the condition of the patient deteriorated, and he died due to his illness.
Haff disease is a rare clinical syndrome that is sometimes misdiagnosed. Early diagnosis and proper treatment are essential to prevent progression to multiple organ failure.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):317-320
DOI 10.5935/0103-507X.20140045
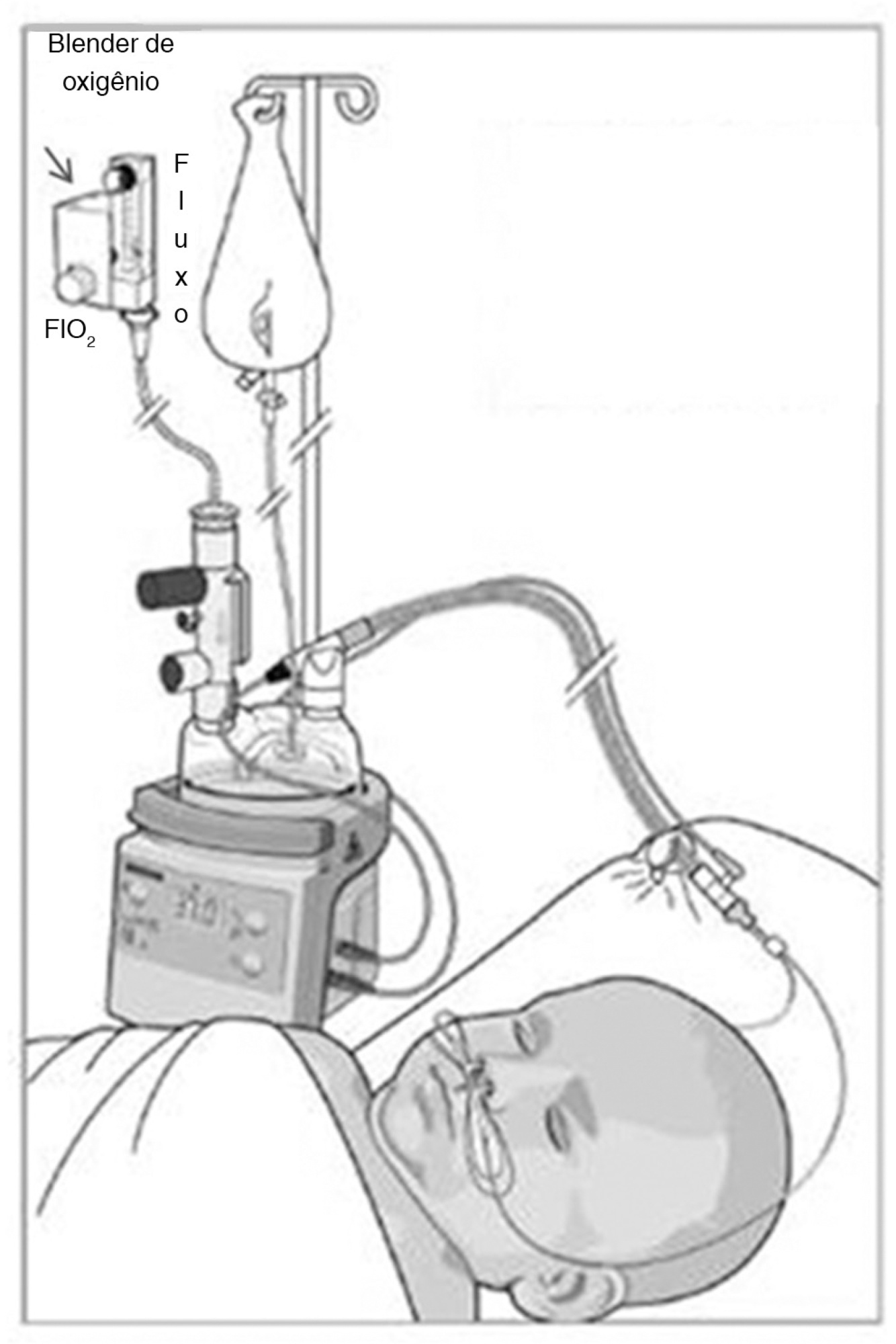
Atelectasis is a pulmonary disorder that lengthens the hospitalization time of newborns in intensive care units, resulting in increased morbidity among these infants. High-flow nasal cannulae have been used in newborns to prevent atelectasis and/or expand pulmonary regions affected by atelectasis; however, to date, no evidence-based data regarding this approach have been reported. In this paper, we report on the cases of two male newborn patients. The first and second patients described in this report were hospitalized for a neurosurgical procedure and the treatment of abdominal disease, respectively, and were subjected to invasive mechanical ventilation for 4 and 36 days, respectively. After extubation, these patients continued receiving oxygen therapy but experienced clinical and radiological worsening typical of atelectasis. In both cases, by 24 hours after the implantation of an high-flow nasal cannulae to provide noninvasive support, radiological examinations revealed the complete resolution of atelectasis. In these cases, the use of an high-flow nasal cannulae was effective in reversing atelectasis. Thus, this approach may be utilized as a supplemental noninvasive ventilatory therapy to avoid unnecessary intubation.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):317-320
DOI 10.5935/0103-507X.20140045
Atelectasis is a pulmonary disorder that lengthens the hospitalization time of newborns in intensive care units, resulting in increased morbidity among these infants. High-flow nasal cannulae have been used in newborns to prevent atelectasis and/or expand pulmonary regions affected by atelectasis; however, to date, no evidence-based data regarding this approach have been reported. In this paper, we report on the cases of two male newborn patients. The first and second patients described in this report were hospitalized for a neurosurgical procedure and the treatment of abdominal disease, respectively, and were subjected to invasive mechanical ventilation for 4 and 36 days, respectively. After extubation, these patients continued receiving oxygen therapy but experienced clinical and radiological worsening typical of atelectasis. In both cases, by 24 hours after the implantation of an high-flow nasal cannulae to provide noninvasive support, radiological examinations revealed the complete resolution of atelectasis. In these cases, the use of an high-flow nasal cannulae was effective in reversing atelectasis. Thus, this approach may be utilized as a supplemental noninvasive ventilatory therapy to avoid unnecessary intubation.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):313-316
DOI 10.5935/0103-507X.20140044
We describe herein a case of a patient who, when in orthostatic positions, had severe hypoxemia and ventilatory dysfunction. Although the severity of symptoms required hospitalization in an intensive care setting, the initial tests only identified the presence of enlarged aortic root, which did not explain the condition. The association of these events with an unusual etiology, namely intracardiac shunt, characterized the diagnosis of platypnea-orthodeoxia syndrome. The literature review shows that, with advancing research methods, there was a progressive increase in the identification of this condition, and this association should be part of the differential diagnosis of dyspnea in patients with enlarged aortic root.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):313-316
DOI 10.5935/0103-507X.20140044
We describe herein a case of a patient who, when in orthostatic positions, had severe hypoxemia and ventilatory dysfunction. Although the severity of symptoms required hospitalization in an intensive care setting, the initial tests only identified the presence of enlarged aortic root, which did not explain the condition. The association of these events with an unusual etiology, namely intracardiac shunt, characterized the diagnosis of platypnea-orthodeoxia syndrome. The literature review shows that, with advancing research methods, there was a progressive increase in the identification of this condition, and this association should be part of the differential diagnosis of dyspnea in patients with enlarged aortic root.
