ARDS Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(4):544-548
DOI 10.5935/0103-507X.20210082
To evaluate whether there was any impact on the number of pediatric extracorporeal membrane oxygenation runs and survival rates in the years subsequent to the 2009 pandemic.
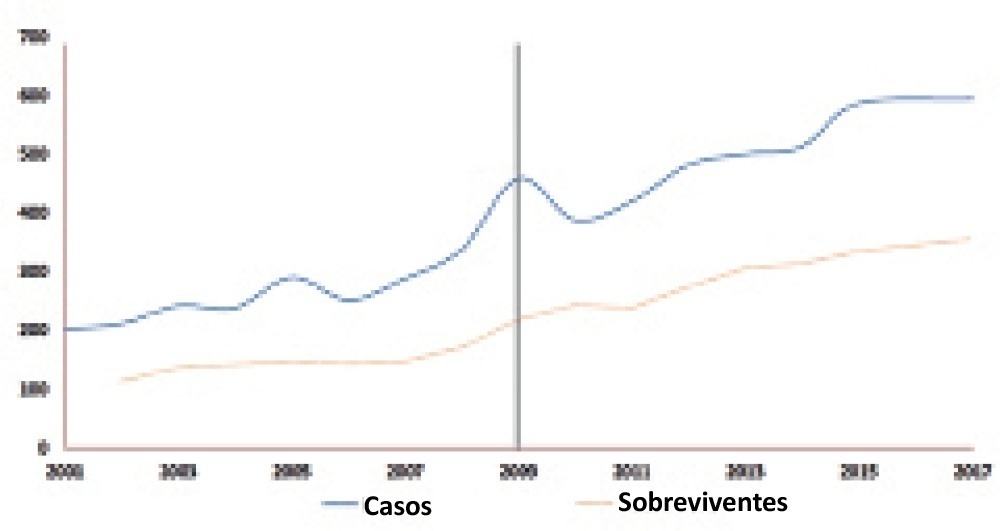
We studied two different periods of extracorporeal membrane oxygenation support for respiratory failure in children by analyzing datasets from the Extracorporeal Life Support Organization. Autoregressive integrated moving average models were constructed to estimate the effect of the pandemic. The year 2009 was the year of intervention (the H1N1 epidemic) in an interrupted time series model. Data collected from 2001 - 2010 were considered preintervention, and data collected from 2010 - 2017 were considered postintervention.
There was an increase in survival rates in the period 2010 - 2017 compared to 2001 - 2010 (p < 0.0001), with a significant improvement in survival when extracorporeal membrane oxygenation was performed for acute respiratory failure due to viral pneumonia. The autoregressive integrated moving average model shows an increase of 23 extracorporeal membrane oxygenation runs per year, prior to the point of the level effect (2009). In terms of survival, the preslope shows that there was no significant increase in survival rates before 2009 (p = 0.41), but the level effect was nearly significant after two years (p = 0.05), with a 6% increase in survival. In four years, there was an 8% (p = 0.03) increase in survival, and six years after 2009, there was up to a 10% (p = 0.026) increase in survival.
In the years following 2009, there was a significant, global incremental increase in the extracorporeal membrane oxygenation survival rates for all runs, mainly due to improvements in the technology and treatment protocols for acute respiratory failure related to viral pneumonia and other respiratory conditions.
Abstract
Rev Bras Ter Intensiva. 2021;33(4):544-548
DOI 10.5935/0103-507X.20210082
To evaluate whether there was any impact on the number of pediatric extracorporeal membrane oxygenation runs and survival rates in the years subsequent to the 2009 pandemic.
We studied two different periods of extracorporeal membrane oxygenation support for respiratory failure in children by analyzing datasets from the Extracorporeal Life Support Organization. Autoregressive integrated moving average models were constructed to estimate the effect of the pandemic. The year 2009 was the year of intervention (the H1N1 epidemic) in an interrupted time series model. Data collected from 2001 - 2010 were considered preintervention, and data collected from 2010 - 2017 were considered postintervention.
There was an increase in survival rates in the period 2010 - 2017 compared to 2001 - 2010 (p < 0.0001), with a significant improvement in survival when extracorporeal membrane oxygenation was performed for acute respiratory failure due to viral pneumonia. The autoregressive integrated moving average model shows an increase of 23 extracorporeal membrane oxygenation runs per year, prior to the point of the level effect (2009). In terms of survival, the preslope shows that there was no significant increase in survival rates before 2009 (p = 0.41), but the level effect was nearly significant after two years (p = 0.05), with a 6% increase in survival. In four years, there was an 8% (p = 0.03) increase in survival, and six years after 2009, there was up to a 10% (p = 0.026) increase in survival.
In the years following 2009, there was a significant, global incremental increase in the extracorporeal membrane oxygenation survival rates for all runs, mainly due to improvements in the technology and treatment protocols for acute respiratory failure related to viral pneumonia and other respiratory conditions.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):37-42
DOI 10.1590/S0103-507X2008000100006
BACKGROUND AND OBJECTIVES: In acute respiratory discomfort syndrome (ARDS) patients, prone position improves oxygenation in more than 70% of the cases. It is well known that prone position promotes a lot of pulmonary changes, including pulmonary mechanics, so we hypothesized that there is the necessity to optimize the ventilatory parameters after the patient is placed in prone position, especially the positive end expiratory pressure (PEEP) values. The objective of this study valued the influence of the prone position at the calculation of the ideal PEEP, given a title by the best pulmonary complaisance and he compared the pulmonary alterations of mechanics, of oxygenation and of ventilation in the positions supine and prone. METHODS: Prospective study, taken place in the Irmandade Santa Casa de Misericórdia de São Paulo Intensive Care Service. Three fases have been compared. Fase 1: in supine position, after the best PEEP calculation. Fase 2: two hours after the patient was placed in prone position and the best PEEP was calculated. The patient was kept for 6 hours in this position. Fase 3: after this time, patient was placed in supine again and after two hours, a new best PEEP calculation and arterial gas analysis was done. And then fase1 versus fase 2, fase 2 versus fase 3, fase 3 versus fase1 were compared. RESULTS: There were no differences in the PEEP values found in all study fases: fase 1 = 14 ± 4.43; fase 2 = 14.73 ± 4.77 and fase 3 = 13.65 ± 4.92. CONCLUSIONS: There were no differences in best PEEP values between prone and supine position. Therefore, there is no need to recalculate the PEEP value after each position change.
Abstract
Rev Bras Ter Intensiva. 2008;20(1):37-42
DOI 10.1590/S0103-507X2008000100006
BACKGROUND AND OBJECTIVES: In acute respiratory discomfort syndrome (ARDS) patients, prone position improves oxygenation in more than 70% of the cases. It is well known that prone position promotes a lot of pulmonary changes, including pulmonary mechanics, so we hypothesized that there is the necessity to optimize the ventilatory parameters after the patient is placed in prone position, especially the positive end expiratory pressure (PEEP) values. The objective of this study valued the influence of the prone position at the calculation of the ideal PEEP, given a title by the best pulmonary complaisance and he compared the pulmonary alterations of mechanics, of oxygenation and of ventilation in the positions supine and prone. METHODS: Prospective study, taken place in the Irmandade Santa Casa de Misericórdia de São Paulo Intensive Care Service. Three fases have been compared. Fase 1: in supine position, after the best PEEP calculation. Fase 2: two hours after the patient was placed in prone position and the best PEEP was calculated. The patient was kept for 6 hours in this position. Fase 3: after this time, patient was placed in supine again and after two hours, a new best PEEP calculation and arterial gas analysis was done. And then fase1 versus fase 2, fase 2 versus fase 3, fase 3 versus fase1 were compared. RESULTS: There were no differences in the PEEP values found in all study fases: fase 1 = 14 ± 4.43; fase 2 = 14.73 ± 4.77 and fase 3 = 13.65 ± 4.92. CONCLUSIONS: There were no differences in best PEEP values between prone and supine position. Therefore, there is no need to recalculate the PEEP value after each position change.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):469-474
DOI 10.1590/S0103-507X2007000400011
BACKGROUND AND OBJECTIVES: Mechanical ventilation is considered a basic element of life support in the intensive care unit and is essential for patients with acute lung injury (ALI) and acute respiratory distress syndrome (ARDS). Experimental studies have demonstrated that mechanical ventilation with high volumes and/or high pressures can exacerbate (VALI) or induce lung injury (VILI) with histological aspect similar to ALI/ARDS. CONTENTS: This systematic review included the literature on MedLine and SciElo database published in the last 20 years. In this review, we will highlight the most recent data on the mechanisms of VILI. The main mechanisms of VILI are: volutrauma caused by overinflation and uneven expansion of the lungs due to high ventilation pressures or volumes; aletectrauma induced by shear forces generated during cyclic closure and reopening of terminal airways; and biotrauma where the injury resulted from the release inflammatory mediators due to physical stresses associated with mechanical ventilation. CONCLUSIONS: It is fundamental to understand the mechanisms related to volutrauma, atelectrauma, and biotrauma to avoid ventilator-associated lung injury.
Abstract
Rev Bras Ter Intensiva. 2007;19(4):469-474
DOI 10.1590/S0103-507X2007000400011
BACKGROUND AND OBJECTIVES: Mechanical ventilation is considered a basic element of life support in the intensive care unit and is essential for patients with acute lung injury (ALI) and acute respiratory distress syndrome (ARDS). Experimental studies have demonstrated that mechanical ventilation with high volumes and/or high pressures can exacerbate (VALI) or induce lung injury (VILI) with histological aspect similar to ALI/ARDS. CONTENTS: This systematic review included the literature on MedLine and SciElo database published in the last 20 years. In this review, we will highlight the most recent data on the mechanisms of VILI. The main mechanisms of VILI are: volutrauma caused by overinflation and uneven expansion of the lungs due to high ventilation pressures or volumes; aletectrauma induced by shear forces generated during cyclic closure and reopening of terminal airways; and biotrauma where the injury resulted from the release inflammatory mediators due to physical stresses associated with mechanical ventilation. CONCLUSIONS: It is fundamental to understand the mechanisms related to volutrauma, atelectrauma, and biotrauma to avoid ventilator-associated lung injury.
Abstract
Rev Bras Ter Intensiva. 2007;19(1):113-117
DOI 10.1590/S0103-507X2007000100015
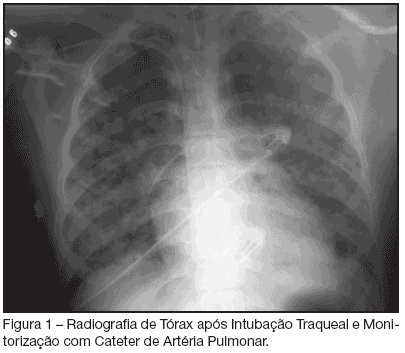
BACKGROUNG AND OBJECTIVES: Varicella is an exantematic disease caused by varicella-zoster virus. Varicella pneumonia complicated with acute respiratory distress syndrome (ARDS) is very rare in adults and is associated with high morbimortality. We report two cases of ARDS secondary to varicella-zoster virus pneumonia. CASES REPORT: We report two cases of ARDS and multiple organ dysfunction syndrome (MODS) secondary to varicella-zoster virus pneumonia. A 15-year-old man with human immunodeficiency virus (HIV) infection and a 29-year-old immunocompetent female were admitted in the ICU with primary varicella infection and pneumonia. Both cases progressed towards ARDS, severe thrombocytopenia and acidosis. In addition cardiovascular and renal failure occurred in the first and second patients, respectively. Treatment consisted of immediate administration of intravenous acyclovir and a lung-protective ventilation strategy. CONCLUSIONS: Both cases of varicella-zoster pneumonia, complicated with ARDS and MODS, had a favourable outcome.
Abstract
Rev Bras Ter Intensiva. 2007;19(1):113-117
DOI 10.1590/S0103-507X2007000100015
BACKGROUNG AND OBJECTIVES: Varicella is an exantematic disease caused by varicella-zoster virus. Varicella pneumonia complicated with acute respiratory distress syndrome (ARDS) is very rare in adults and is associated with high morbimortality. We report two cases of ARDS secondary to varicella-zoster virus pneumonia. CASES REPORT: We report two cases of ARDS and multiple organ dysfunction syndrome (MODS) secondary to varicella-zoster virus pneumonia. A 15-year-old man with human immunodeficiency virus (HIV) infection and a 29-year-old immunocompetent female were admitted in the ICU with primary varicella infection and pneumonia. Both cases progressed towards ARDS, severe thrombocytopenia and acidosis. In addition cardiovascular and renal failure occurred in the first and second patients, respectively. Treatment consisted of immediate administration of intravenous acyclovir and a lung-protective ventilation strategy. CONCLUSIONS: Both cases of varicella-zoster pneumonia, complicated with ARDS and MODS, had a favourable outcome.