Você pesquisou por y - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2024;36:e20240023en
DOI 10.62675/2965-2774.20240023-en
Abstract
Crit Care Sci. 2024;36:e20240023en
DOI 10.62675/2965-2774.20240023-en
Abstract
Crit Care Sci. 2024;36:e20240088en
DOI 10.62675/2965-2774.20240088-en
Abstract
Crit Care Sci. 2024;36:e20240088en
DOI 10.62675/2965-2774.20240088-en
Abstract
Crit Care Sci. 2024;36:e20240229en
DOI 10.62675/2965-2774.20240229-en
To compare two methods for defining and classifying the severity of pediatric acute respiratory distress syndrome: the Berlin classification, which uses the relationship between the partial pressure of oxygen and the fraction of inspired oxygen, and the classification of the Pediatric Acute Lung Injury Consensus Conference, which uses the oxygenation index.
This was a prospective study of patients aged 0 - 18 years with a diagnosis of acute respiratory distress syndrome who were invasively mechanically ventilated and provided one to three arterial blood gas samples, totaling 140 valid measurements. These measures were evaluated for correlation using the Spearman test and agreement using the kappa coefficient between the two classifications, initially using the general population of the study and then subdividing it into patients with and without bronchospasm and those with and without the use of neuromuscular blockers. The effect of these two factors (bronchospasm and neuromuscular blocking agent) separately and together on both classifications was also assessed using two-way analysis of variance.
In the general population, who were 54 patients aged 0 - 18 years a strong negative correlation was found by Spearman’s test (ρ -0.91; p < 0.001), and strong agreement was found by the kappa coefficient (0.62; p < 0.001) in the comparison between Berlin and Pediatric Acute Lung Injury Consensus Conference. In the populations with and without bronchospasm and who did and did not use neuromuscular blockers, the correlation coefficients were similar to those of the general population, though among patients not using neuromuscular blockers, there was greater agreement between the classifications than for patients using neuromuscular blockers (kappa 0.67 versus 0.56, p < 0.001 for both). Neuromuscular blockers had a significant effect on the relationship between the partial pressure of oxygen and the fraction of inspired oxygen (analysis of variance; F: 12.9; p < 0.001) and the oxygenation index (analysis of variance; F: 8.3; p = 0.004).
There was a strong correlation and agreement between the two classifications in the general population and in the subgroups studied. Use of neuromuscular blockers had a significant effect on the severity of acute respiratory distress syndrome.
Abstract
Crit Care Sci. 2024;36:e20240229en
DOI 10.62675/2965-2774.20240229-en
To compare two methods for defining and classifying the severity of pediatric acute respiratory distress syndrome: the Berlin classification, which uses the relationship between the partial pressure of oxygen and the fraction of inspired oxygen, and the classification of the Pediatric Acute Lung Injury Consensus Conference, which uses the oxygenation index.
This was a prospective study of patients aged 0 - 18 years with a diagnosis of acute respiratory distress syndrome who were invasively mechanically ventilated and provided one to three arterial blood gas samples, totaling 140 valid measurements. These measures were evaluated for correlation using the Spearman test and agreement using the kappa coefficient between the two classifications, initially using the general population of the study and then subdividing it into patients with and without bronchospasm and those with and without the use of neuromuscular blockers. The effect of these two factors (bronchospasm and neuromuscular blocking agent) separately and together on both classifications was also assessed using two-way analysis of variance.
In the general population, who were 54 patients aged 0 - 18 years a strong negative correlation was found by Spearman’s test (ρ -0.91; p < 0.001), and strong agreement was found by the kappa coefficient (0.62; p < 0.001) in the comparison between Berlin and Pediatric Acute Lung Injury Consensus Conference. In the populations with and without bronchospasm and who did and did not use neuromuscular blockers, the correlation coefficients were similar to those of the general population, though among patients not using neuromuscular blockers, there was greater agreement between the classifications than for patients using neuromuscular blockers (kappa 0.67 versus 0.56, p < 0.001 for both). Neuromuscular blockers had a significant effect on the relationship between the partial pressure of oxygen and the fraction of inspired oxygen (analysis of variance; F: 12.9; p < 0.001) and the oxygenation index (analysis of variance; F: 8.3; p = 0.004).
There was a strong correlation and agreement between the two classifications in the general population and in the subgroups studied. Use of neuromuscular blockers had a significant effect on the severity of acute respiratory distress syndrome.
Abstract
Crit Care Sci. 2024;36:e20240114en
DOI 10.62675/2965-2774.20240114-en
Abstract
Crit Care Sci. 2024;36:e20240114en
DOI 10.62675/2965-2774.20240114-en
Abstract
Crit Care Sci. 2024;36:e20240258en
DOI 10.62675/2965-2774.20240258-en
Evidence about long-term sequelae after hospitalization for acute respiratory distress syndrome due to COVID-19 is still scarce.
To evaluate changes in pulmonary, cardiac, and renal function and in quality of life after hospitalization for acute respiratory distress syndrome secondary to COVID-19.
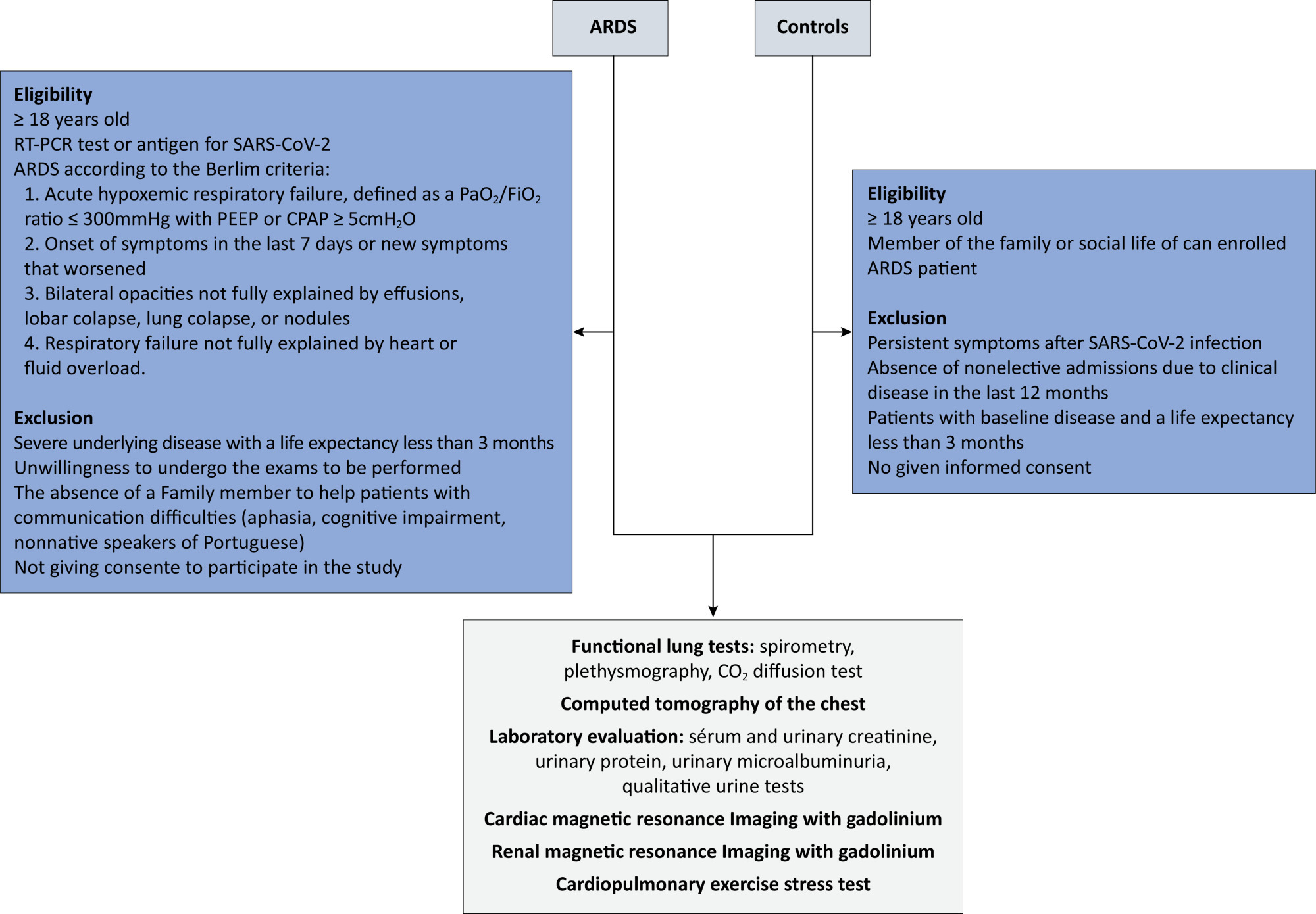
This will be a multicenter case–control study of 220 participants. Eligible are patients who are hospitalized for acute respiratory distress syndrome due to COVID-19. In the control group, individuals with no history of hospitalization in the last 12 months or long-term symptoms of COVID-19 will be selected. All individuals will be subjected to pulmonary spirometry with a carbon monoxide diffusion test, chest tomography, cardiac and renal magnetic resonance imaging with gadolinium, ergospirometry, serum and urinary creatinine, total protein, and urinary microalbuminuria, in addition to quality-of-life questionnaires. Patients will be evaluated 12 months after hospital discharge, and controls will be evaluated within 90 days of inclusion in the study. For all the statistical analyses, p < 0.05 is the threshold for significance.
The primary outcome of the study will be the pulmonary diffusing capacity for carbon monoxide measured after 12 months. The other parameters of pulmonary, cardiac, and renal function and quality of life are secondary outcomes.
This study aims to determine the long-term sequelae of pulmonary, cardiac, and renal function and the quality of life of patients hospitalized for acute respiratory distress syndrome due to COVID-19 in the Brazilian population.
Abstract
Crit Care Sci. 2024;36:e20240258en
DOI 10.62675/2965-2774.20240258-en
Evidence about long-term sequelae after hospitalization for acute respiratory distress syndrome due to COVID-19 is still scarce.
To evaluate changes in pulmonary, cardiac, and renal function and in quality of life after hospitalization for acute respiratory distress syndrome secondary to COVID-19.
This will be a multicenter case–control study of 220 participants. Eligible are patients who are hospitalized for acute respiratory distress syndrome due to COVID-19. In the control group, individuals with no history of hospitalization in the last 12 months or long-term symptoms of COVID-19 will be selected. All individuals will be subjected to pulmonary spirometry with a carbon monoxide diffusion test, chest tomography, cardiac and renal magnetic resonance imaging with gadolinium, ergospirometry, serum and urinary creatinine, total protein, and urinary microalbuminuria, in addition to quality-of-life questionnaires. Patients will be evaluated 12 months after hospital discharge, and controls will be evaluated within 90 days of inclusion in the study. For all the statistical analyses, p < 0.05 is the threshold for significance.
The primary outcome of the study will be the pulmonary diffusing capacity for carbon monoxide measured after 12 months. The other parameters of pulmonary, cardiac, and renal function and quality of life are secondary outcomes.
This study aims to determine the long-term sequelae of pulmonary, cardiac, and renal function and the quality of life of patients hospitalized for acute respiratory distress syndrome due to COVID-19 in the Brazilian population.
Abstract
Crit Care Sci. 2024;36:e20240049en
DOI 10.62675/2965-2774.20240049-en
Boswellia serrata is an herbal extract from the Boswellia serrata tree that has anti-inflammatory and analgesic properties and alleviates pain caused by rheumatoid arthritis, gout, osteoarthritis, and sciatica. Syndrome of inappropriate antidiuretic hormone secretion accompanied by hyponatremia, seizures, and rhabdomyolysis as a manifestation of Boswellia serrata intoxication has not been reported previously. A 38-year-old female suffered clinically isolated syndrome and has since been regularly taking B. serrata capsules (200mg/d) to strengthen her immune system. She experienced hypersensitivity to light, ocular pain, nausea, dizziness, and lower limb weakness four days after receiving her first BNT162b2 vaccine dose, and she increased the dosage of B. serrata to five capsules (1000mg/d) one week after vaccination. After taking B. serrata at a dosage of 1000mg/d for 3 weeks, she was admitted to the intensive care unit because of a first, unprovoked generalized tonic–clonic seizure. The patient's workup revealed syndrome of inappropriate antidiuretic hormone secretion, which resolved completely upon treatment and discontinuation of B. serrata. In summary, B. serrata potentially causes syndrome of inappropriate antidiuretic hormone secretion when it is taken at high doses. Patients should not self-medicate.
Abstract
Crit Care Sci. 2024;36:e20240049en
DOI 10.62675/2965-2774.20240049-en
Boswellia serrata is an herbal extract from the Boswellia serrata tree that has anti-inflammatory and analgesic properties and alleviates pain caused by rheumatoid arthritis, gout, osteoarthritis, and sciatica. Syndrome of inappropriate antidiuretic hormone secretion accompanied by hyponatremia, seizures, and rhabdomyolysis as a manifestation of Boswellia serrata intoxication has not been reported previously. A 38-year-old female suffered clinically isolated syndrome and has since been regularly taking B. serrata capsules (200mg/d) to strengthen her immune system. She experienced hypersensitivity to light, ocular pain, nausea, dizziness, and lower limb weakness four days after receiving her first BNT162b2 vaccine dose, and she increased the dosage of B. serrata to five capsules (1000mg/d) one week after vaccination. After taking B. serrata at a dosage of 1000mg/d for 3 weeks, she was admitted to the intensive care unit because of a first, unprovoked generalized tonic–clonic seizure. The patient's workup revealed syndrome of inappropriate antidiuretic hormone secretion, which resolved completely upon treatment and discontinuation of B. serrata. In summary, B. serrata potentially causes syndrome of inappropriate antidiuretic hormone secretion when it is taken at high doses. Patients should not self-medicate.
Abstract
Crit Care Sci. 2024;36:e20240291en
DOI 10.62675/2965-2774.20240291-en
Abstract
Crit Care Sci. 2024;36:e20240291en
DOI 10.62675/2965-2774.20240291-en
Abstract
Crit Care Sci. 2024;36:e20240192en
DOI 10.62675/2965-2774.20240192-en
Abstract
Crit Care Sci. 2024;36:e20240192en
DOI 10.62675/2965-2774.20240192-en