Você pesquisou por y?yr=2006 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2006;18(1):52-58
DOI 10.1590/S0103-507X2006000100010
BACKGROUND AND OBJECTIVES: Establish the clinical, epidemiological and laboratorial characteristics of septic patients in an intensive care unit (ICU) of a tertiary care private hospital from Pernambuco, in the northeast of Brazil. METHODS: Cohort study without intervention that included adult patients admitted in the ICU with sepsis or that developed it during ICU stay, during a 6-month period. The patients were followed during all ICU stay period. Laboratory and clinical data were collected after sepsis diagnosis. ICU admission APACHE II score and the SOFA score during the three first days after inclusion in the study were collected. RESULTS: The study included 199 patients, of whom 67.8% were older than 65 years of age. More than a half (56.3%) survived the septic episode, mean APACHE II was 18.2 ± 6.3 and mean SOFA score was 6.3 ± 3.7. The disease related to the admission in ICU was medical in 85.4%, and the majority of patients had a chronic associated disease. In 79.3% the lungs were the source of sepsis and in 40% of patients the etiologic agent of sepsis was isolated. Amongst laboratory tests, thrombocytopenia (platelets < 100.000/mm³) was observed on 20.6%, fibrinogen was elevated (> 300 mg/dL) on 81.7%, and the activity of antithrombin was low (< 70%) on 32.5% of patients. CONCLUSIONS: The epidemiology of sepsis in this study, in a private hospital of Recife, was no different from what was recently described in Southeast and South of Brazil, United States and Europe.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):52-58
DOI 10.1590/S0103-507X2006000100010
BACKGROUND AND OBJECTIVES: Establish the clinical, epidemiological and laboratorial characteristics of septic patients in an intensive care unit (ICU) of a tertiary care private hospital from Pernambuco, in the northeast of Brazil. METHODS: Cohort study without intervention that included adult patients admitted in the ICU with sepsis or that developed it during ICU stay, during a 6-month period. The patients were followed during all ICU stay period. Laboratory and clinical data were collected after sepsis diagnosis. ICU admission APACHE II score and the SOFA score during the three first days after inclusion in the study were collected. RESULTS: The study included 199 patients, of whom 67.8% were older than 65 years of age. More than a half (56.3%) survived the septic episode, mean APACHE II was 18.2 ± 6.3 and mean SOFA score was 6.3 ± 3.7. The disease related to the admission in ICU was medical in 85.4%, and the majority of patients had a chronic associated disease. In 79.3% the lungs were the source of sepsis and in 40% of patients the etiologic agent of sepsis was isolated. Amongst laboratory tests, thrombocytopenia (platelets < 100.000/mm³) was observed on 20.6%, fibrinogen was elevated (> 300 mg/dL) on 81.7%, and the activity of antithrombin was low (< 70%) on 32.5% of patients. CONCLUSIONS: The epidemiology of sepsis in this study, in a private hospital of Recife, was no different from what was recently described in Southeast and South of Brazil, United States and Europe.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):59-62
DOI 10.1590/S0103-507X2006000100011
BACKGROUND AND OBJECTIVES: The assessment of illness severity and prognosis of obstetric patients by scoring systems is still a controversial issue. Preeclampsia is a leading cause of severe maternal morbidity and mortality, and a major cause of obstetric admission to intensive care unit. There is paucity of data regarding the predictability of critically ill preeclamptic women and the application of scoring systems to this population. This study aimed to evaluate and compare the application of APACHE II, SAPS II and MPM II scoring systems between a preeclamptic population and a non obstetric female population. METHODS: A case-control study was conducted on 28 preeclamptic women and 56 non obstetric female patients, admitted to a general intensive care unit over a period of 10 years. The predictive accuracy of the prognostic evaluation systems was estimated by the area under the receiver operator characteristic curve. RESULTS: The mortality rate was 21.4% (6:28) for the study group and 35.7% (20:56) for the control group, with an OR = 0.49 (95%CI = 0.17-1.41). The main causes of ICU admission of preeclamptic women were HELLP syndrome, coma and pulmonary edema. In the preeclamptic population, only the MPM II score showed an area under the ROC curve statistically different from 0.500, while in the control group, all scoring systems had their areas under the ROC curves statistically different from 0.500. CONCLUSIONS: The application of APACHE II and SAPS II to evaluate critically ill preeclamptic women may be not appropriate.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):59-62
DOI 10.1590/S0103-507X2006000100011
BACKGROUND AND OBJECTIVES: The assessment of illness severity and prognosis of obstetric patients by scoring systems is still a controversial issue. Preeclampsia is a leading cause of severe maternal morbidity and mortality, and a major cause of obstetric admission to intensive care unit. There is paucity of data regarding the predictability of critically ill preeclamptic women and the application of scoring systems to this population. This study aimed to evaluate and compare the application of APACHE II, SAPS II and MPM II scoring systems between a preeclamptic population and a non obstetric female population. METHODS: A case-control study was conducted on 28 preeclamptic women and 56 non obstetric female patients, admitted to a general intensive care unit over a period of 10 years. The predictive accuracy of the prognostic evaluation systems was estimated by the area under the receiver operator characteristic curve. RESULTS: The mortality rate was 21.4% (6:28) for the study group and 35.7% (20:56) for the control group, with an OR = 0.49 (95%CI = 0.17-1.41). The main causes of ICU admission of preeclamptic women were HELLP syndrome, coma and pulmonary edema. In the preeclamptic population, only the MPM II score showed an area under the ROC curve statistically different from 0.500, while in the control group, all scoring systems had their areas under the ROC curves statistically different from 0.500. CONCLUSIONS: The application of APACHE II and SAPS II to evaluate critically ill preeclamptic women may be not appropriate.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
BACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
BACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):7-8
Abstract
Rev Bras Ter Intensiva. 2006;18(1):7-8
Abstract
Rev Bras Ter Intensiva. 2006;18(1):78-85
DOI 10.1590/S0103-507X2006000100013
BACKGROUND AND OBJECTIVES: Cardiac output and preload as absolute data do not offer helpful information about the hemodynamic of critically ill patients. However, monitoring the response of these variables to volume challenge or inotropic drugs is a very useful tool in the critical care setting, particularly for patients with signs of tissue hypoperfusion. Although PAC remains the " gold standard" to measure cardiac output and preload, new and alternative technologies were developed to evaluate these hemodynamic variables. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty three physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations regarding the use of arterial pulse pressure variation during mechanical ventilation, continuous arterial pulse contour and lithium dilution cardiac output measurements, esophageal Doppler waveform, thoracic electrical bioimpedance, echocardiography and partial CO2 rebreathing for monitoring cardiac output and preload were created. CONCLUSIONS: The new and less invasive techniques for the measurement of cardiac output, preload or fluid responsiveness are accurate and may be an alternative to PAC in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):78-85
DOI 10.1590/S0103-507X2006000100013
BACKGROUND AND OBJECTIVES: Cardiac output and preload as absolute data do not offer helpful information about the hemodynamic of critically ill patients. However, monitoring the response of these variables to volume challenge or inotropic drugs is a very useful tool in the critical care setting, particularly for patients with signs of tissue hypoperfusion. Although PAC remains the " gold standard" to measure cardiac output and preload, new and alternative technologies were developed to evaluate these hemodynamic variables. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty three physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations regarding the use of arterial pulse pressure variation during mechanical ventilation, continuous arterial pulse contour and lithium dilution cardiac output measurements, esophageal Doppler waveform, thoracic electrical bioimpedance, echocardiography and partial CO2 rebreathing for monitoring cardiac output and preload were created. CONCLUSIONS: The new and less invasive techniques for the measurement of cardiac output, preload or fluid responsiveness are accurate and may be an alternative to PAC in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):86-94
DOI 10.1590/S0103-507X2006000100014
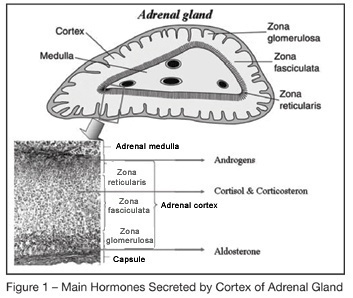
BACKGROUND AND OBJECTIVES: Corticosteroids were introduced in the treatment of severe infection as early as in the nineteen forties. Several " negative" randomized controlled trials of high-dose of glucocorticoids given for a short period of time in the early course of severe sepsis or acute respiratory distress syndrome raised serious doubts on the benefit of this treatment. Recently, a link between septic shock and adrenal insufficiency, or systemic inflammation induced glucocorticoids receptor resistance had been established. This finding prompted renewed interest of a replacement therapy with low doses of corticosteroids during longer periods. The goal of this article is to review the key role of corticosteroids in the host response to stress and will update the reader with the new validated indications of corticosteroids treatment in the ICU. CONTENTS: Extensive review of the adrenal physiology and its pathophysiological derangements and clinical implications in critically ill patients. CONCLUSIONS: During sepsis, hemodynamic instability and perpetuation of inflammatory state may result from adrenal insufficiency (AI). Thus, an ACTH test should be performed as soon as possible to identify non overt AI. It should be immediately followed by a replacement therapy with iv bolus of 50 mg of hydrocortisone every 6 hours combined to 50 µg of fludrocortisone once daily. When the results of the ACTH test are available, treatment should be continued for 7 days in the non responders to ACTH and withdraw in the responders. Whether responders to ACTH with high baseline cortisol levels (> 34 µg/dL) have tissue resistance to cortisol and also should receive exogenous hormones remains to be evaluated in clinical trials.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):86-94
DOI 10.1590/S0103-507X2006000100014
BACKGROUND AND OBJECTIVES: Corticosteroids were introduced in the treatment of severe infection as early as in the nineteen forties. Several " negative" randomized controlled trials of high-dose of glucocorticoids given for a short period of time in the early course of severe sepsis or acute respiratory distress syndrome raised serious doubts on the benefit of this treatment. Recently, a link between septic shock and adrenal insufficiency, or systemic inflammation induced glucocorticoids receptor resistance had been established. This finding prompted renewed interest of a replacement therapy with low doses of corticosteroids during longer periods. The goal of this article is to review the key role of corticosteroids in the host response to stress and will update the reader with the new validated indications of corticosteroids treatment in the ICU. CONTENTS: Extensive review of the adrenal physiology and its pathophysiological derangements and clinical implications in critically ill patients. CONCLUSIONS: During sepsis, hemodynamic instability and perpetuation of inflammatory state may result from adrenal insufficiency (AI). Thus, an ACTH test should be performed as soon as possible to identify non overt AI. It should be immediately followed by a replacement therapy with iv bolus of 50 mg of hydrocortisone every 6 hours combined to 50 µg of fludrocortisone once daily. When the results of the ACTH test are available, treatment should be continued for 7 days in the non responders to ACTH and withdraw in the responders. Whether responders to ACTH with high baseline cortisol levels (> 34 µg/dL) have tissue resistance to cortisol and also should receive exogenous hormones remains to be evaluated in clinical trials.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):9-17
DOI 10.1590/S0103-507X2006000100003
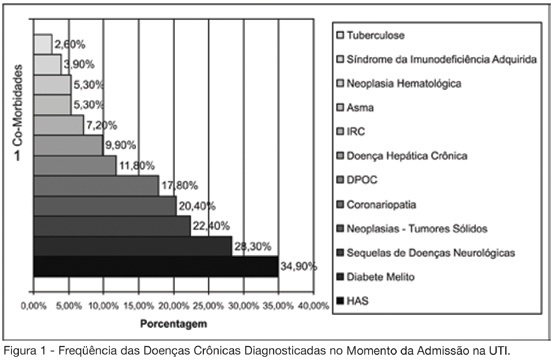
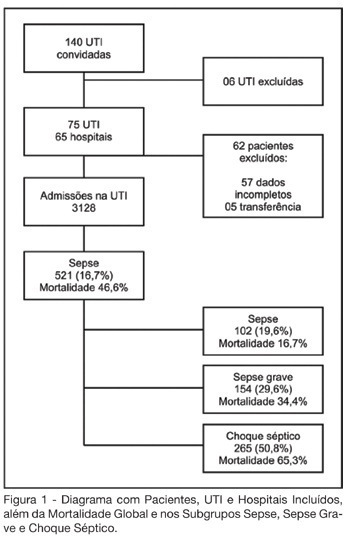
BACKGROUND AND OBJECTIVES: Sepsis represents the major cause of death in the ICUs all over the world. Many studies have shown an increasing incidence over time and only a slight reduce in mortality. Many new treatment strategies are arising and we should define the incidence and features of sepsis in Brazil. METHODS: Prospective cohort study in sixty-five hospitals all over Brazil. The patients who were admitted or who developed sepsis during the month of September, 2003 were enrolled. They were followed until the 28th day and/or until their discharge. The diagnoses were made in accordance to the criteria proposed by ACCP/SCCM. It were evaluated demographic features, APACHE II score, SOFA (Sepsis-related Organ Failure Assessment) score, mortality, sources of infections, microbiology, morbidities and length of stay (LOS). RESULTS: Seventy-five ICUs from all regions of Brazil took part in the study.3128 patients were identified and 521 (16.7%) filled the criteria of sepsis, severe sepsis or septic shock. Mean age was 61.7 (IQR 39-79), 293 (55.7%) were males, and the overall 28-day mortality rate was 46.6%. Average APACHE II score was 20 and SOFA score on the first day was 7 (IQR 4-10). SOFA score in the mortality group was higher on day 1 (8, IQR 5-11), and had increased on day 3 (9, IQR 6-12). The mortality rate for sepsis, severe sepsis and septic shock was 16.7%, 34.4% and 65.3%, respectively. The average LOS was 15 days (IQR 5-22). The two main sources of infection were the respiratory tract (69%) and the abdomen one (23.1%). Gram-negative bacilli were more prevalent (40.1%). Gram-positive cocci were identified in 32.8% and fungi infections in 5%. Mechanical ventilation was observed in 82.1% of the patients, Swan-Ganz catheter in 18.8%, vasopressors in 66.2% and hemotransfusion in 44.7%. CONCLUSIONS: It was observed a high mortality of sepsis in the ICUs in Brazil. The high frequency of septic shock demonstrated a group at high risk of death. In order to have a better use of the resources and reduce in mortality during the next 5 years, it is very important to identify our specific features related to this syndrome.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):9-17
DOI 10.1590/S0103-507X2006000100003
BACKGROUND AND OBJECTIVES: Sepsis represents the major cause of death in the ICUs all over the world. Many studies have shown an increasing incidence over time and only a slight reduce in mortality. Many new treatment strategies are arising and we should define the incidence and features of sepsis in Brazil. METHODS: Prospective cohort study in sixty-five hospitals all over Brazil. The patients who were admitted or who developed sepsis during the month of September, 2003 were enrolled. They were followed until the 28th day and/or until their discharge. The diagnoses were made in accordance to the criteria proposed by ACCP/SCCM. It were evaluated demographic features, APACHE II score, SOFA (Sepsis-related Organ Failure Assessment) score, mortality, sources of infections, microbiology, morbidities and length of stay (LOS). RESULTS: Seventy-five ICUs from all regions of Brazil took part in the study.3128 patients were identified and 521 (16.7%) filled the criteria of sepsis, severe sepsis or septic shock. Mean age was 61.7 (IQR 39-79), 293 (55.7%) were males, and the overall 28-day mortality rate was 46.6%. Average APACHE II score was 20 and SOFA score on the first day was 7 (IQR 4-10). SOFA score in the mortality group was higher on day 1 (8, IQR 5-11), and had increased on day 3 (9, IQR 6-12). The mortality rate for sepsis, severe sepsis and septic shock was 16.7%, 34.4% and 65.3%, respectively. The average LOS was 15 days (IQR 5-22). The two main sources of infection were the respiratory tract (69%) and the abdomen one (23.1%). Gram-negative bacilli were more prevalent (40.1%). Gram-positive cocci were identified in 32.8% and fungi infections in 5%. Mechanical ventilation was observed in 82.1% of the patients, Swan-Ganz catheter in 18.8%, vasopressors in 66.2% and hemotransfusion in 44.7%. CONCLUSIONS: It was observed a high mortality of sepsis in the ICUs in Brazil. The high frequency of septic shock demonstrated a group at high risk of death. In order to have a better use of the resources and reduce in mortality during the next 5 years, it is very important to identify our specific features related to this syndrome.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):95-98
DOI 10.1590/S0103-507X2006000100015
BACKGROUND AND OBJECTIVES: Iatrogenic conditions was due of the medical, correctly intervention or not, justified or not, which harmful consequences to the patient. The cares in Intensive Care Medicine present substantial challenges with relation to the security of the patient. The objective of this article is to make one brief revision of literature on the iatrogenic in its concepts and basic terms and its taxes prevalence in Intensive Care Medicine. CONTENTS: Intensive Care Medicine supplies subsidies that improve the morbidity and mortality, but that also the significant risks of adverse events and serious errors associate. The Iatrogenic can be minimized with the adequate monitorization or can be friction as waited aggravation, idiopathic and if to perpetuate in the anonymity. CONCLUSIONS: It is basic to recognize the necessity of the constant learning and recycling and conscience of the susceptibilities to the error; in this context, the respect for the human being must guide the professional behavior.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):95-98
DOI 10.1590/S0103-507X2006000100015
BACKGROUND AND OBJECTIVES: Iatrogenic conditions was due of the medical, correctly intervention or not, justified or not, which harmful consequences to the patient. The cares in Intensive Care Medicine present substantial challenges with relation to the security of the patient. The objective of this article is to make one brief revision of literature on the iatrogenic in its concepts and basic terms and its taxes prevalence in Intensive Care Medicine. CONTENTS: Intensive Care Medicine supplies subsidies that improve the morbidity and mortality, but that also the significant risks of adverse events and serious errors associate. The Iatrogenic can be minimized with the adequate monitorization or can be friction as waited aggravation, idiopathic and if to perpetuate in the anonymity. CONCLUSIONS: It is basic to recognize the necessity of the constant learning and recycling and conscience of the susceptibilities to the error; in this context, the respect for the human being must guide the professional behavior.
