iatrogenic Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2006;18(1):95-98
DOI 10.1590/S0103-507X2006000100015
BACKGROUND AND OBJECTIVES: Iatrogenic conditions was due of the medical, correctly intervention or not, justified or not, which harmful consequences to the patient. The cares in Intensive Care Medicine present substantial challenges with relation to the security of the patient. The objective of this article is to make one brief revision of literature on the iatrogenic in its concepts and basic terms and its taxes prevalence in Intensive Care Medicine. CONTENTS: Intensive Care Medicine supplies subsidies that improve the morbidity and mortality, but that also the significant risks of adverse events and serious errors associate. The Iatrogenic can be minimized with the adequate monitorization or can be friction as waited aggravation, idiopathic and if to perpetuate in the anonymity. CONCLUSIONS: It is basic to recognize the necessity of the constant learning and recycling and conscience of the susceptibilities to the error; in this context, the respect for the human being must guide the professional behavior.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):95-98
DOI 10.1590/S0103-507X2006000100015
BACKGROUND AND OBJECTIVES: Iatrogenic conditions was due of the medical, correctly intervention or not, justified or not, which harmful consequences to the patient. The cares in Intensive Care Medicine present substantial challenges with relation to the security of the patient. The objective of this article is to make one brief revision of literature on the iatrogenic in its concepts and basic terms and its taxes prevalence in Intensive Care Medicine. CONTENTS: Intensive Care Medicine supplies subsidies that improve the morbidity and mortality, but that also the significant risks of adverse events and serious errors associate. The Iatrogenic can be minimized with the adequate monitorization or can be friction as waited aggravation, idiopathic and if to perpetuate in the anonymity. CONCLUSIONS: It is basic to recognize the necessity of the constant learning and recycling and conscience of the susceptibilities to the error; in this context, the respect for the human being must guide the professional behavior.

Abstract
Rev Bras Ter Intensiva. 2006;18(1):104-108
DOI 10.1590/S0103-507X2006000100017
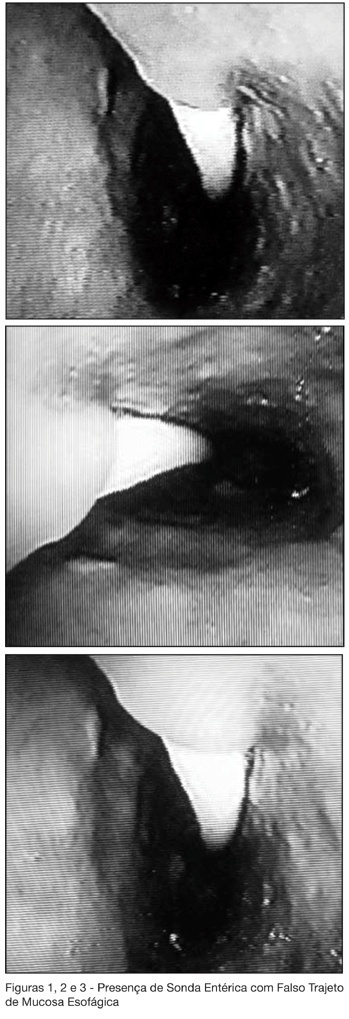
BACKGROUND AND OBJECTIVES: This study is a case report of a patient that was submitted to implant of enteric tube (ET) in the ICU, being evidenced false passage in proximal esophagus during endoscopic procedure, demonstrating tunnel for the submucosa. CASE REPORT: A 77 years old woman, transferred to ICU, where ET was installed (due to difficulty of being carried through both nostrils) being confirmed its position through thoraco-abdominal x-ray. The patient remained around 10 days with the ET, receiving diet, without any alteration. In the 10th day she was evolved with melena and reduction of the values of Hb/Ht, without hemodynamic repercussion. Submitted to the high digestive endoscopic that evidenced ulcer injury to bulbar, of about 2.5 cm, with signals of former bleeding. During the examination, a false passage of the ET in proximal esophagus was visualized: 2 cm below of the crico-faring, tunnel for the submucosa possibly for all above-mentioned segments, following its habitual passage until gastric chamber. CONCLUSIONS: Patients of high risk for esophagus perforation for ET installation can be identified and well-taken care of adjusted they can be used. If to occur perforation, this must be identified how much so early possible, for adequate treatment. The adequate treatment depends of each case and same the clinical therapy can be appropriate in selected cases.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):104-108
DOI 10.1590/S0103-507X2006000100017
BACKGROUND AND OBJECTIVES: This study is a case report of a patient that was submitted to implant of enteric tube (ET) in the ICU, being evidenced false passage in proximal esophagus during endoscopic procedure, demonstrating tunnel for the submucosa. CASE REPORT: A 77 years old woman, transferred to ICU, where ET was installed (due to difficulty of being carried through both nostrils) being confirmed its position through thoraco-abdominal x-ray. The patient remained around 10 days with the ET, receiving diet, without any alteration. In the 10th day she was evolved with melena and reduction of the values of Hb/Ht, without hemodynamic repercussion. Submitted to the high digestive endoscopic that evidenced ulcer injury to bulbar, of about 2.5 cm, with signals of former bleeding. During the examination, a false passage of the ET in proximal esophagus was visualized: 2 cm below of the crico-faring, tunnel for the submucosa possibly for all above-mentioned segments, following its habitual passage until gastric chamber. CONCLUSIONS: Patients of high risk for esophagus perforation for ET installation can be identified and well-taken care of adjusted they can be used. If to occur perforation, this must be identified how much so early possible, for adequate treatment. The adequate treatment depends of each case and same the clinical therapy can be appropriate in selected cases.