
You searched for:"Mônica Lajana de Almeida"
We found (3) results for your search.-
Original Articles
Comparison and effects of two different airway occlusion times during measurement of maximal inspiratory pressure in adult intensive care unit neurological patients
Rev Bras Ter Intensiva. 2010;22(1):33-39
Abstract
Original ArticlesComparison and effects of two different airway occlusion times during measurement of maximal inspiratory pressure in adult intensive care unit neurological patients
Rev Bras Ter Intensiva. 2010;22(1):33-39
DOI 10.1590/S0103-507X2010000100007
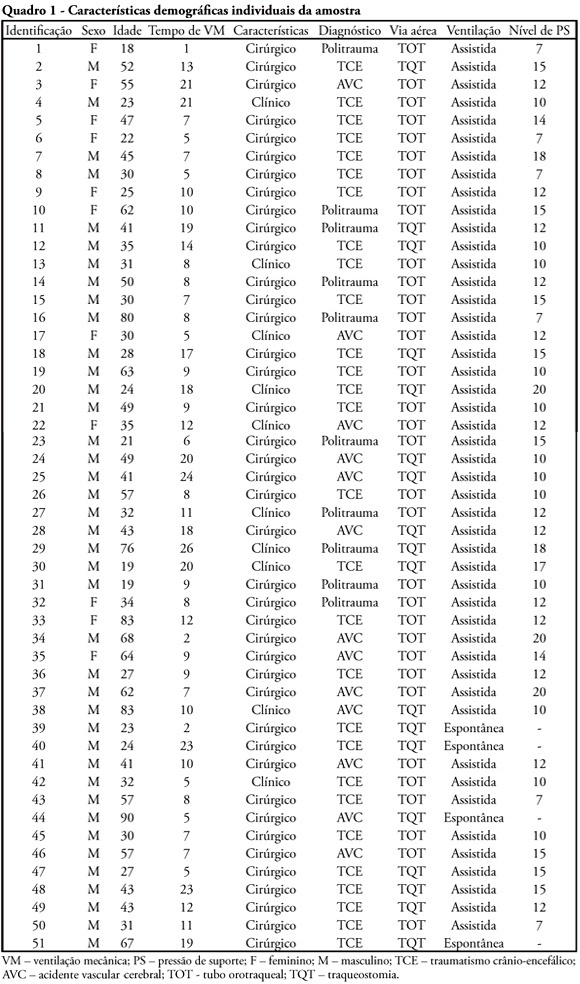
Views0See moreOBJECTIVE: To verify if the maximal inspiratory pressure values with 40 seconds occlusion time are greater than with the 20 seconds occlusion time, and the impacts on the following patient’s physiological variables: respiratory rate, pulse oxygen saturation, heart rate and blood pressure, before and after the measurements. METHODS: This was a transversal prospective randomized study. Fifty-one patients underwent maximal inspiratory pressure measurement, measured by one single investigator. The manometer was calibrated before each measurement, and then connected to the adapter and this to the unidirectional valve inspiratory branch for 20 or 40 seconds. RESULTS: The values with 40 seconds occlusion (57.6 ± 23.4 cmH2O) were significantly higher than the measurements taken with 20 seconds occlusion (40.5 ± 23.4 cmH2O; p=0.0001). The variables changes between the before and after measurement respiratory and hemodynamic parameters monitoring showed: heart rate variation for the 20 seconds occlusion 5.13 ± 8.56 beats per minute and after 40 seconds occlusion 7.94 ± 12.05 beats per minute (p = 0.053), versus baseline. The mean blood pressure change for 20 seconds occlusion was 9.29 ± 13.35 mmHg and for 40 seconds occlusion 15.52 ± 2.91 mmHg (p=0.021). The oxygen saturation change for 20 seconds occlusion was 1.66 ± 12.66%, and for 40 seconds 4.21 ± 5.53% (p=0.0001). The respiratory rate change for 20 seconds occlusion was 6.68 ± 12.66 movements per minute and for 40 seconds 6.94 ± 6.01 (p=0.883). CONCLUSION: The measurement of maximal inspiratory pressure using a longer occlusion (40 seconds) produced higher values, without triggering clinically significant stress according to the selected variables.
Views0

Abstract
Original ArticlesComparison and effects of two different airway occlusion times during measurement of maximal inspiratory pressure in adult intensive care unit neurological patients
Rev Bras Ter Intensiva. 2010;22(1):33-39
DOI 10.1590/S0103-507X2010000100007
Views0See moreOBJECTIVE: To verify if the maximal inspiratory pressure values with 40 seconds occlusion time are greater than with the 20 seconds occlusion time, and the impacts on the following patient’s physiological variables: respiratory rate, pulse oxygen saturation, heart rate and blood pressure, before and after the measurements. METHODS: This was a transversal prospective randomized study. Fifty-one patients underwent maximal inspiratory pressure measurement, measured by one single investigator. The manometer was calibrated before each measurement, and then connected to the adapter and this to the unidirectional valve inspiratory branch for 20 or 40 seconds. RESULTS: The values with 40 seconds occlusion (57.6 ± 23.4 cmH2O) were significantly higher than the measurements taken with 20 seconds occlusion (40.5 ± 23.4 cmH2O; p=0.0001). The variables changes between the before and after measurement respiratory and hemodynamic parameters monitoring showed: heart rate variation for the 20 seconds occlusion 5.13 ± 8.56 beats per minute and after 40 seconds occlusion 7.94 ± 12.05 beats per minute (p = 0.053), versus baseline. The mean blood pressure change for 20 seconds occlusion was 9.29 ± 13.35 mmHg and for 40 seconds occlusion 15.52 ± 2.91 mmHg (p=0.021). The oxygen saturation change for 20 seconds occlusion was 1.66 ± 12.66%, and for 40 seconds 4.21 ± 5.53% (p=0.0001). The respiratory rate change for 20 seconds occlusion was 6.68 ± 12.66 movements per minute and for 40 seconds 6.94 ± 6.01 (p=0.883). CONCLUSION: The measurement of maximal inspiratory pressure using a longer occlusion (40 seconds) produced higher values, without triggering clinically significant stress according to the selected variables.
-
Review Articles
Management of mechanical ventilation in brain injury: hyperventilation and positive end-expiratory pressure
Rev Bras Ter Intensiva. 2009;21(1):72-79
Abstract
Review ArticlesManagement of mechanical ventilation in brain injury: hyperventilation and positive end-expiratory pressure
Rev Bras Ter Intensiva. 2009;21(1):72-79
DOI 10.1590/S0103-507X2009000100011
Views0The study intended to make a critical review on use of pulmonary hyperventilation maneuvers and the different positive end-expiratory pressures applied to traumatic brain injury patients. As a reference were used publications in English, Spanish and Portuguese, contained in the following databases: MedLine, SciELO and LILACS, from 2000 to 2007, we included all studies about the use of pulmonary hyperventilation maneuvers and the different positive end-expiratory levels used for adult patients with brain injury at acute or chronic stage. Thirty one trials were selected, 13 about pulmonary hyperventilation, as prophylaxis, prolonged or optimized and 9 shows the levels of positive end-expiratory pressures used, ranging from 0 to 15 cmH2O. The prophylactic hyperventilation maneuver in the first 24 hours can lead to an increase of cerebral ischemia; the prolonged hyperventilation must be avoided if intracranial pressure did not increase; however optimized hyperventilation seems to be the most promising technique for control of the intracranial pressure and cerebral perfusion pressure; the rise of the positive end-expiratory pressure, up to 15cmH2O, can be applied in a conscientious form aiming to increase arterial oxygen saturation in lung injury.
Keywords:Brain traumaHyperventilationIntracranial hypertensionIntracranial pressurePositive pressure respirationSee moreViews0Abstract
Review ArticlesManagement of mechanical ventilation in brain injury: hyperventilation and positive end-expiratory pressure
Rev Bras Ter Intensiva. 2009;21(1):72-79
DOI 10.1590/S0103-507X2009000100011
Views0The study intended to make a critical review on use of pulmonary hyperventilation maneuvers and the different positive end-expiratory pressures applied to traumatic brain injury patients. As a reference were used publications in English, Spanish and Portuguese, contained in the following databases: MedLine, SciELO and LILACS, from 2000 to 2007, we included all studies about the use of pulmonary hyperventilation maneuvers and the different positive end-expiratory levels used for adult patients with brain injury at acute or chronic stage. Thirty one trials were selected, 13 about pulmonary hyperventilation, as prophylaxis, prolonged or optimized and 9 shows the levels of positive end-expiratory pressures used, ranging from 0 to 15 cmH2O. The prophylactic hyperventilation maneuver in the first 24 hours can lead to an increase of cerebral ischemia; the prolonged hyperventilation must be avoided if intracranial pressure did not increase; however optimized hyperventilation seems to be the most promising technique for control of the intracranial pressure and cerebral perfusion pressure; the rise of the positive end-expiratory pressure, up to 15cmH2O, can be applied in a conscientious form aiming to increase arterial oxygen saturation in lung injury.
Keywords:Brain traumaHyperventilationIntracranial hypertensionIntracranial pressurePositive pressure respirationSee more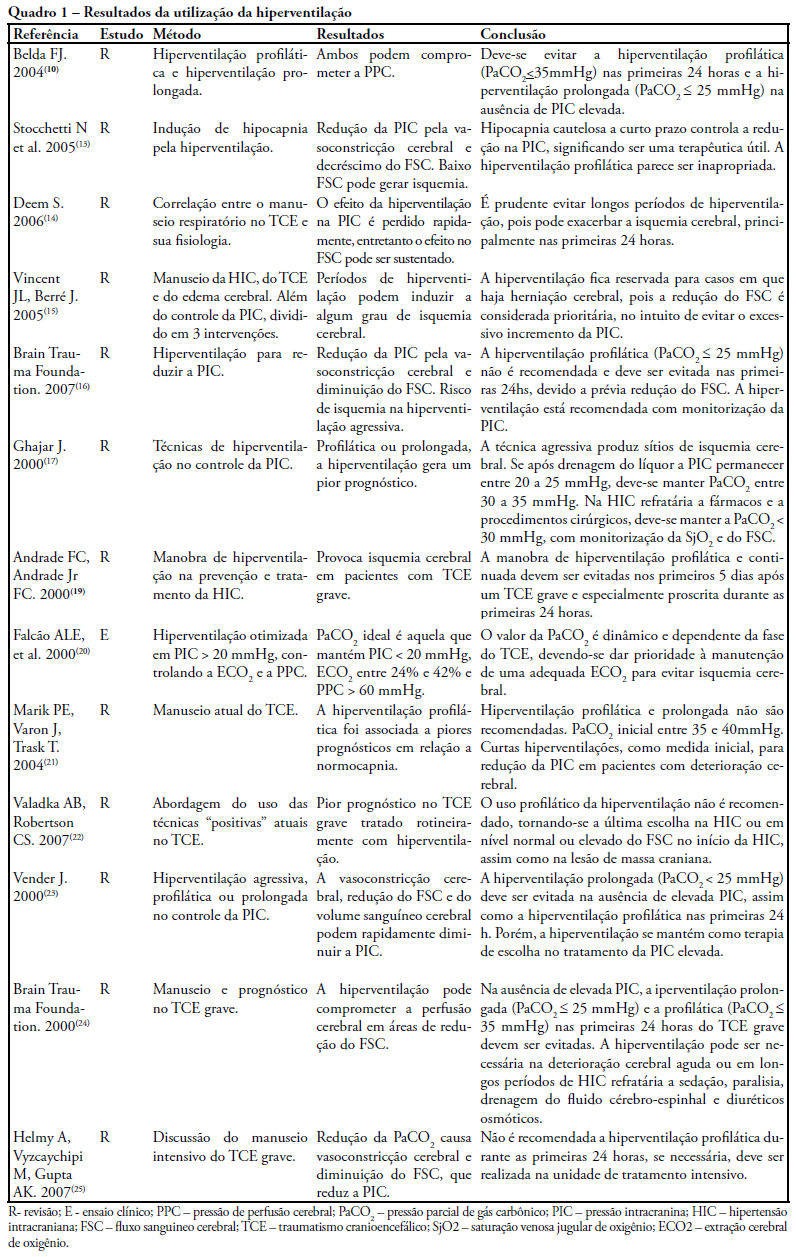
-
Artigos originais
Traumatic brain injury and acute respiratory distress syndrome: how to ventilate? Evaluation of clinical practice
Rev Bras Ter Intensiva. 2007;19(1):44-52
Abstract
Artigos originaisTraumatic brain injury and acute respiratory distress syndrome: how to ventilate? Evaluation of clinical practice
Rev Bras Ter Intensiva. 2007;19(1):44-52
DOI 10.1590/S0103-507X2007000100006
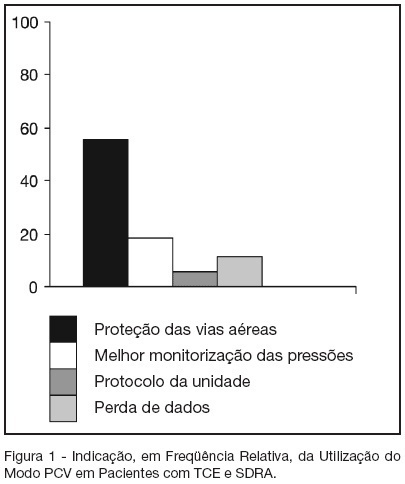
Views0See moreBACKGROUND AND OBJECTIVES: The traumatic brain injury (TBI) is a healthy-world problem, some of his patients develop respiratory failure, requiring intubation and mechanical ventilation, and the most common complications are the acute respiratory distress syndrome (ARDS). In this way, this study has the objective describe the daily clinical practice of respiratory care in this patients submit mechanical ventilation. METHODS: The methods and ventilatories parameters used to ventilate the patients with TBI and ARDS has been evaluated by a sample of physiotherapists from the city of Salvador, BA, from a descriptive study. The data were collected by face-to-face interviews in the period of October 2005 to March 2006. For in such way a half structuralized questionnaire was elaborated contends changeable social-demographic, about the hospital profile and the applied ventilatory strategy in patients with TBI that come to develop ARDS. RESULTS: The sample was composed by 70 physiotherapists, 41 (58.6%) was female, with mean of age of 31.2 ± 6.4 (24-49) years-old and graduated time 7.7 ± 6.4 (1-27) years, which 37 (52.9%) works on public hospital; 67 (95.7%) has any specialization. Sixty four physiotherapists affirm the usage of the pressure controlled ventilation mode. The peak pressure and the plateau pressure wanted to ventilate the patients with TBI and ARDS were in mean 35.6 ± 5,3 (25-50) and 28,4 ± 5,8 (15-35) cmH2O respectively. Forty eighty (68.6%) of the interviewed wants a PaCO2 in 30-35 mmHg. Thirty one (44.3%) of the interviewed finds the ideal PEEP through the best SpO2 with minor FiO2. CONCLUSIONS: It’s incontestable that the ventilatory strategy of a patient with severe TBI that become to develop ALI or ARDS is an authentic challenge; a predilection for PCV mode is observed due to the already known protective ventilation strategy.
Views0Abstract
Artigos originaisTraumatic brain injury and acute respiratory distress syndrome: how to ventilate? Evaluation of clinical practice
Rev Bras Ter Intensiva. 2007;19(1):44-52
DOI 10.1590/S0103-507X2007000100006
Views0See moreBACKGROUND AND OBJECTIVES: The traumatic brain injury (TBI) is a healthy-world problem, some of his patients develop respiratory failure, requiring intubation and mechanical ventilation, and the most common complications are the acute respiratory distress syndrome (ARDS). In this way, this study has the objective describe the daily clinical practice of respiratory care in this patients submit mechanical ventilation. METHODS: The methods and ventilatories parameters used to ventilate the patients with TBI and ARDS has been evaluated by a sample of physiotherapists from the city of Salvador, BA, from a descriptive study. The data were collected by face-to-face interviews in the period of October 2005 to March 2006. For in such way a half structuralized questionnaire was elaborated contends changeable social-demographic, about the hospital profile and the applied ventilatory strategy in patients with TBI that come to develop ARDS. RESULTS: The sample was composed by 70 physiotherapists, 41 (58.6%) was female, with mean of age of 31.2 ± 6.4 (24-49) years-old and graduated time 7.7 ± 6.4 (1-27) years, which 37 (52.9%) works on public hospital; 67 (95.7%) has any specialization. Sixty four physiotherapists affirm the usage of the pressure controlled ventilation mode. The peak pressure and the plateau pressure wanted to ventilate the patients with TBI and ARDS were in mean 35.6 ± 5,3 (25-50) and 28,4 ± 5,8 (15-35) cmH2O respectively. Forty eighty (68.6%) of the interviewed wants a PaCO2 in 30-35 mmHg. Thirty one (44.3%) of the interviewed finds the ideal PEEP through the best SpO2 with minor FiO2. CONCLUSIONS: It’s incontestable that the ventilatory strategy of a patient with severe TBI that become to develop ALI or ARDS is an authentic challenge; a predilection for PCV mode is observed due to the already known protective ventilation strategy.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis