
You searched for:"Gastón Burghi"
We found (4) results for your search.-
Original Article
Correlation between tomographic scales and vasospasm and delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage
Crit Care Sci. 2023;35(3):311-319
Abstract
Original ArticleCorrelation between tomographic scales and vasospasm and delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage
Crit Care Sci. 2023;35(3):311-319
DOI 10.5935/2965-2774.20230119-es
Views4See moreABSTRACT
Objective:
To determine the prevalence of sonographic vasospasm and delayed ischemic deficit in patients with aneurysmal subarachnoid hemorrhage, to evaluate the correlation between different tomographic scales and these complications, and to study prognostic factors in this group of patients.
Methods:
This was a prospective study of patients admitted to the intensive care unit with a diagnosis of aneurysmal subarachnoid hemorrhage. The prevalence of sonographic vasospasm and radiological delayed cerebral ischemia was analyzed, as was the correlation between different tomographic scales and these complications.
Results:
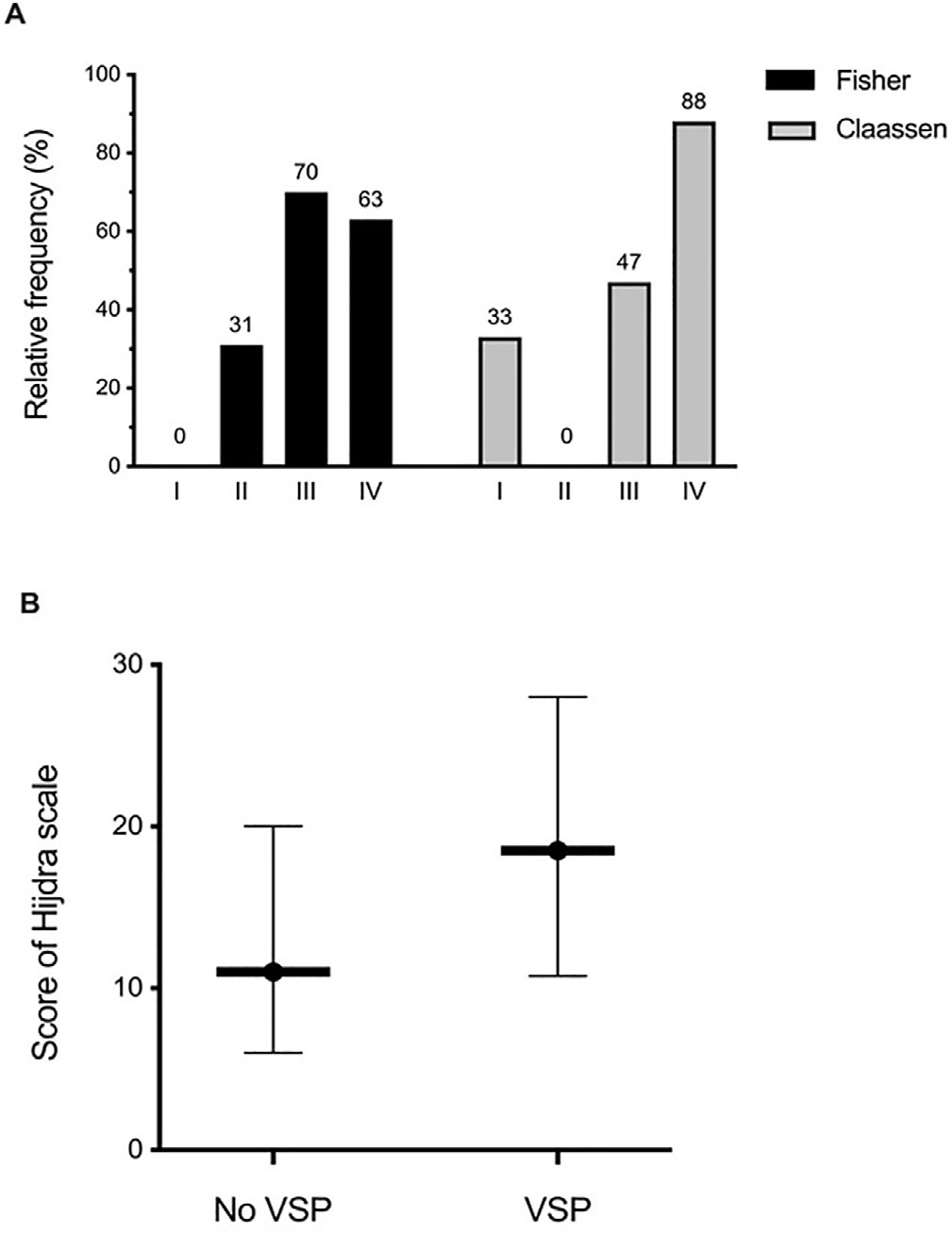
A total of 57 patients were studied. Sixty percent of the patients developed sonographic vasospasm, which was significantly associated with delayed cerebral ischemia and mortality. The Claassen and Hijdra scales were better correlated with the development of cerebral vasospasm (areas under the curve of 0.78 and 0.68) than was Fisher’s scale (0.62). Thirty-two patients (56.1%) developed cerebral infarction on CT; the significantly associated factors were poor clinical grade at admission (p = 0.04), sonographic vasospasm (p = 0.008) and severity of vasospasm (p = 0.015). Only the semiquantitative Hijdra scale was significantly correlated with the development of radiological delayed cerebral ischemia (p = 0.009). The patients who presented cerebral infarction had worse neurological evolution and higher mortality.
Conclusion:
This is the first study in our environment on the subject. The Claassen and Hijdra tomographic scales showed better prognostic performance than the Fisher scale for the development of cerebral vasospasm. The finding of sonographic vasospasm could be a noninvasive criterion for the early detection of delayed cerebral ischemia and neurological deterioration in patients with aneurysmal subarachnoid hemorrhage.
Views4

Abstract
Original ArticleCorrelation between tomographic scales and vasospasm and delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage
Crit Care Sci. 2023;35(3):311-319
DOI 10.5935/2965-2774.20230119-es
Views4See moreABSTRACT
Objective:
To determine the prevalence of sonographic vasospasm and delayed ischemic deficit in patients with aneurysmal subarachnoid hemorrhage, to evaluate the correlation between different tomographic scales and these complications, and to study prognostic factors in this group of patients.
Methods:
This was a prospective study of patients admitted to the intensive care unit with a diagnosis of aneurysmal subarachnoid hemorrhage. The prevalence of sonographic vasospasm and radiological delayed cerebral ischemia was analyzed, as was the correlation between different tomographic scales and these complications.
Results:
A total of 57 patients were studied. Sixty percent of the patients developed sonographic vasospasm, which was significantly associated with delayed cerebral ischemia and mortality. The Claassen and Hijdra scales were better correlated with the development of cerebral vasospasm (areas under the curve of 0.78 and 0.68) than was Fisher’s scale (0.62). Thirty-two patients (56.1%) developed cerebral infarction on CT; the significantly associated factors were poor clinical grade at admission (p = 0.04), sonographic vasospasm (p = 0.008) and severity of vasospasm (p = 0.015). Only the semiquantitative Hijdra scale was significantly correlated with the development of radiological delayed cerebral ischemia (p = 0.009). The patients who presented cerebral infarction had worse neurological evolution and higher mortality.
Conclusion:
This is the first study in our environment on the subject. The Claassen and Hijdra tomographic scales showed better prognostic performance than the Fisher scale for the development of cerebral vasospasm. The finding of sonographic vasospasm could be a noninvasive criterion for the early detection of delayed cerebral ischemia and neurological deterioration in patients with aneurysmal subarachnoid hemorrhage.
-
Original Article
Mortality analysis of adult burn patients in Uruguay
Rev Bras Ter Intensiva. 2020;32(1):43-48
Abstract
Original ArticleMortality analysis of adult burn patients in Uruguay
Rev Bras Ter Intensiva. 2020;32(1):43-48
DOI 10.5935/0103-507X.20200008
Views0See moreABSTRACT
Objective:
To determine the independent risk factors associated with mortality in adult burn patients.
Methods:
This was a retrospective, observational study performed at the Centro Nacional de Queimados do Uruguai. All patients with skin burns admitted to the unit since its opening on July 1, 1995 through December 31, 2018 were included. The demographic data, burn profiles, length of stay, mechanical ventilation duration and hospital mortality were studied. A multivariate logistic regression was used to identify the risk factors for mortality. The standardized mortality ratio was calculated by dividing the number of observed deaths by the number of expected deaths (according to the Abbreviated Burn Severity Index).
Results:
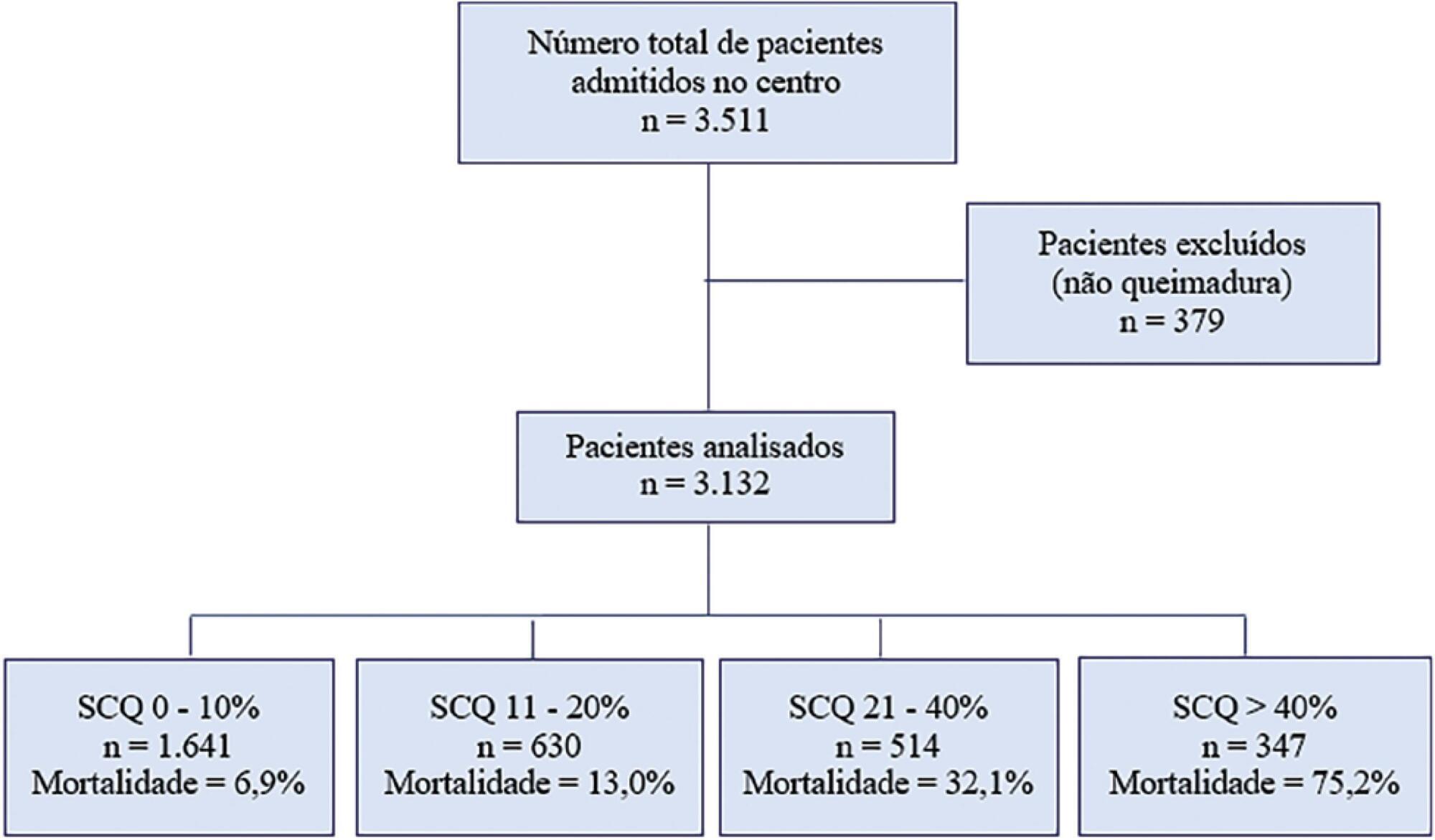
During the study period, 3,132 patients were included. The median total body surface area burned was 10% (3%-22%). The Abbreviated Burn Severity Index was 6 (4 – 7). Invasive mechanical ventilation was required in 60% of the patients for a median duration of 6 (3 – 16) days. The median length of stay in the unit was 17 (7 – 32) days. The global mortality was 19.9%. Crude mortality and standardized mortality ratio decreased from 1995 through 2018. The global standardized mortality ratio was 0.99. A need for mechanical ventilation (OR 8.80; 95%CI 5.68 – 13.62), older age (OR 1.07 per year; 95%CI 1.06 – 1.09), total body surface area burned (OR 1.05 per 1%; 95%CI 1.03 – 1.08) and extension of third-degree burns (OR 1.05 per 1%; 95%CI 1.03 – 1.07) were independent risk factors for mortality.
Conclusion:
The need for mechanical ventilation, older age and burn extension were independent risk factors for mortality in the burned adult Uruguayan population.
Views0Abstract
Original ArticleMortality analysis of adult burn patients in Uruguay
Rev Bras Ter Intensiva. 2020;32(1):43-48
DOI 10.5935/0103-507X.20200008
Views0See moreABSTRACT
Objective:
To determine the independent risk factors associated with mortality in adult burn patients.
Methods:
This was a retrospective, observational study performed at the Centro Nacional de Queimados do Uruguai. All patients with skin burns admitted to the unit since its opening on July 1, 1995 through December 31, 2018 were included. The demographic data, burn profiles, length of stay, mechanical ventilation duration and hospital mortality were studied. A multivariate logistic regression was used to identify the risk factors for mortality. The standardized mortality ratio was calculated by dividing the number of observed deaths by the number of expected deaths (according to the Abbreviated Burn Severity Index).
Results:
During the study period, 3,132 patients were included. The median total body surface area burned was 10% (3%-22%). The Abbreviated Burn Severity Index was 6 (4 – 7). Invasive mechanical ventilation was required in 60% of the patients for a median duration of 6 (3 – 16) days. The median length of stay in the unit was 17 (7 – 32) days. The global mortality was 19.9%. Crude mortality and standardized mortality ratio decreased from 1995 through 2018. The global standardized mortality ratio was 0.99. A need for mechanical ventilation (OR 8.80; 95%CI 5.68 – 13.62), older age (OR 1.07 per year; 95%CI 1.06 – 1.09), total body surface area burned (OR 1.05 per 1%; 95%CI 1.03 – 1.08) and extension of third-degree burns (OR 1.05 per 1%; 95%CI 1.03 – 1.07) were independent risk factors for mortality.
Conclusion:
The need for mechanical ventilation, older age and burn extension were independent risk factors for mortality in the burned adult Uruguayan population.
-
Original Articles
Prognostic impact of the time of admission and discharge from the intensive care unit
Rev Bras Ter Intensiva. 2017;29(1):63-69
Abstract
Original ArticlesPrognostic impact of the time of admission and discharge from the intensive care unit
Rev Bras Ter Intensiva. 2017;29(1):63-69
DOI 10.5935/0103-507X.20170010
Views0See moreABSTRACT
Objective:
To determine the impact of the day and time of admission and discharge from the intensive care unit on mortality.
Methods:
Prospective observational study that included patients admitted to the intensive care unit of the Hospital Maciel in Montevideo between April and November 2014.
Results:
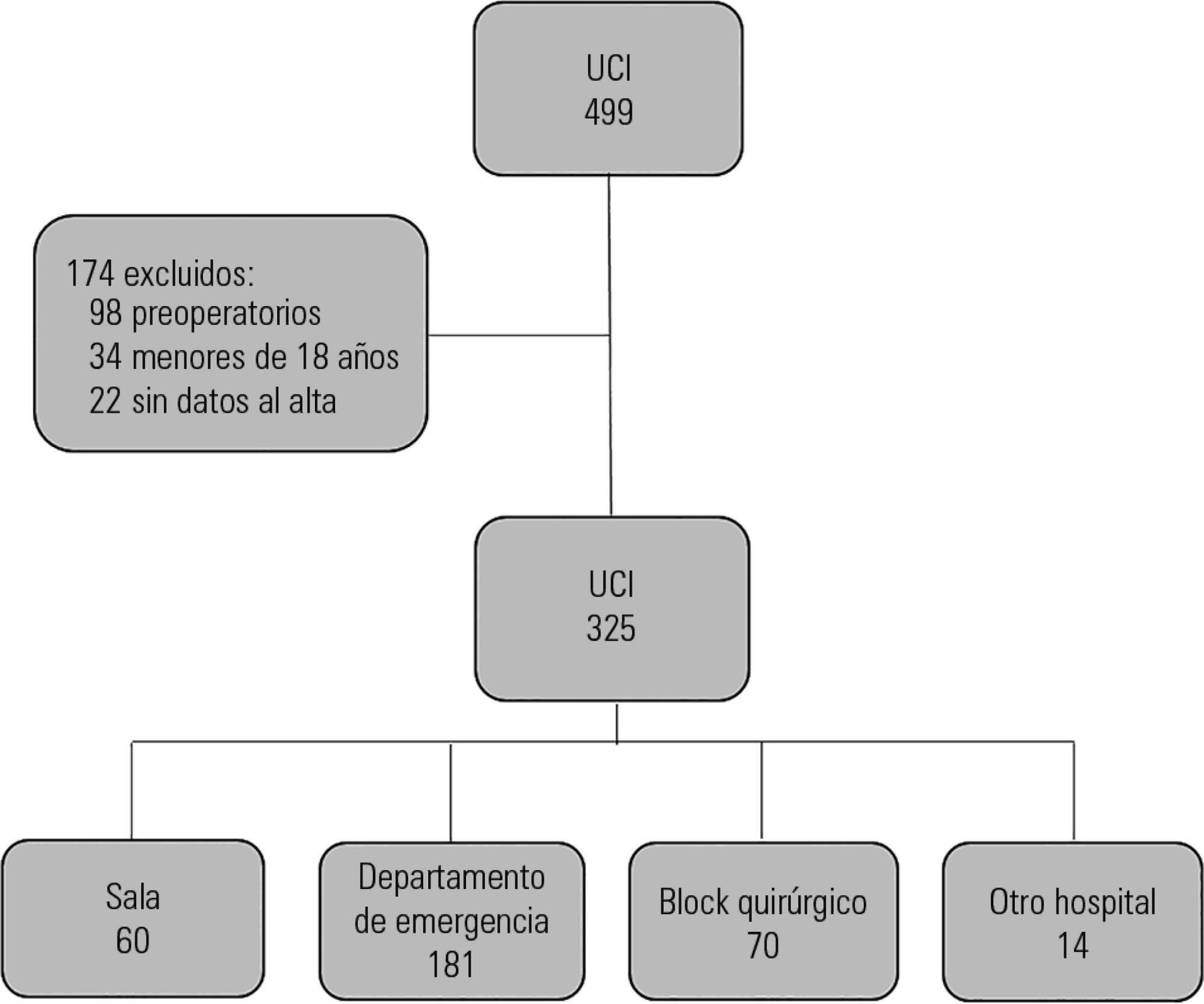
We analyzed 325 patients with an average age of 55 (36 – 71) years and a SAPS II value of 43 (29 – 58) points. No differences were found in the mortality of patients in the intensive care unit when time of admission (35% on the weekend versus 31% on weekdays, p = ns) or the hour of entry (35% at night versus 31% in the daytime, p = ns) were compared. The time of discharge was associated with higher hospital mortality rates (57% for weekend discharges versus 14% for weekday discharges, p = 0.000). The factors independently associated with hospital mortality after discharge from the intensive care unit were age > 50 years (OR 2.4, 95%CI, 1.1 – 5.4) and weekend discharge (OR 7.7, 95%CI, 3.8-15.6).
Conclusion:
This study identified the time of discharge from the intensive care unit as a factor that was independently associated with hospital mortality.
Views0Abstract
Original ArticlesPrognostic impact of the time of admission and discharge from the intensive care unit
Rev Bras Ter Intensiva. 2017;29(1):63-69
DOI 10.5935/0103-507X.20170010
Views0See moreABSTRACT
Objective:
To determine the impact of the day and time of admission and discharge from the intensive care unit on mortality.
Methods:
Prospective observational study that included patients admitted to the intensive care unit of the Hospital Maciel in Montevideo between April and November 2014.
Results:
We analyzed 325 patients with an average age of 55 (36 – 71) years and a SAPS II value of 43 (29 – 58) points. No differences were found in the mortality of patients in the intensive care unit when time of admission (35% on the weekend versus 31% on weekdays, p = ns) or the hour of entry (35% at night versus 31% in the daytime, p = ns) were compared. The time of discharge was associated with higher hospital mortality rates (57% for weekend discharges versus 14% for weekday discharges, p = 0.000). The factors independently associated with hospital mortality after discharge from the intensive care unit were age > 50 years (OR 2.4, 95%CI, 1.1 – 5.4) and weekend discharge (OR 7.7, 95%CI, 3.8-15.6).
Conclusion:
This study identified the time of discharge from the intensive care unit as a factor that was independently associated with hospital mortality.
-
Review Articles
Dysglycemia in the critically ill patient: current evidence and future perspectives
Rev Bras Ter Intensiva. 2017;29(3):364-372
Abstract
Review ArticlesDysglycemia in the critically ill patient: current evidence and future perspectives
Rev Bras Ter Intensiva. 2017;29(3):364-372
DOI 10.5935/0103-507X.20170054
Views0ABSTRACT
Dysglycemia in critically ill patients (hyperglycemia, hypoglycemia, glycemic variability and time in range) is a biomarker of disease severity and is associated with higher mortality. However, this impact appears to be weakened in patients with previous diabetes mellitus, particularly in those with poor premorbid glycemic control; this phenomenon has been called “diabetes paradox”. This phenomenon determines that glycated hemoglobin (HbA1c) values should be considered in choosing glycemic control protocols on admission to an intensive care unit and that patients’ target blood glucose ranges should be adjusted according to their HbA1c values. Therefore, HbA1c emerges as a simple tool that allows information that has therapeutic utility and prognostic value to be obtained in the intensive care unit.
Keywords:Blood glucoseHemoglobin A, glycosylatedhyperglycemiaHypoglycemiaIntensive care unitsMortalitySeverity of illness indexSee moreViews0Abstract
Review ArticlesDysglycemia in the critically ill patient: current evidence and future perspectives
Rev Bras Ter Intensiva. 2017;29(3):364-372
DOI 10.5935/0103-507X.20170054
Views0ABSTRACT
Dysglycemia in critically ill patients (hyperglycemia, hypoglycemia, glycemic variability and time in range) is a biomarker of disease severity and is associated with higher mortality. However, this impact appears to be weakened in patients with previous diabetes mellitus, particularly in those with poor premorbid glycemic control; this phenomenon has been called “diabetes paradox”. This phenomenon determines that glycated hemoglobin (HbA1c) values should be considered in choosing glycemic control protocols on admission to an intensive care unit and that patients’ target blood glucose ranges should be adjusted according to their HbA1c values. Therefore, HbA1c emerges as a simple tool that allows information that has therapeutic utility and prognostic value to be obtained in the intensive care unit.
Keywords:Blood glucoseHemoglobin A, glycosylatedhyperglycemiaHypoglycemiaIntensive care unitsMortalitySeverity of illness indexSee more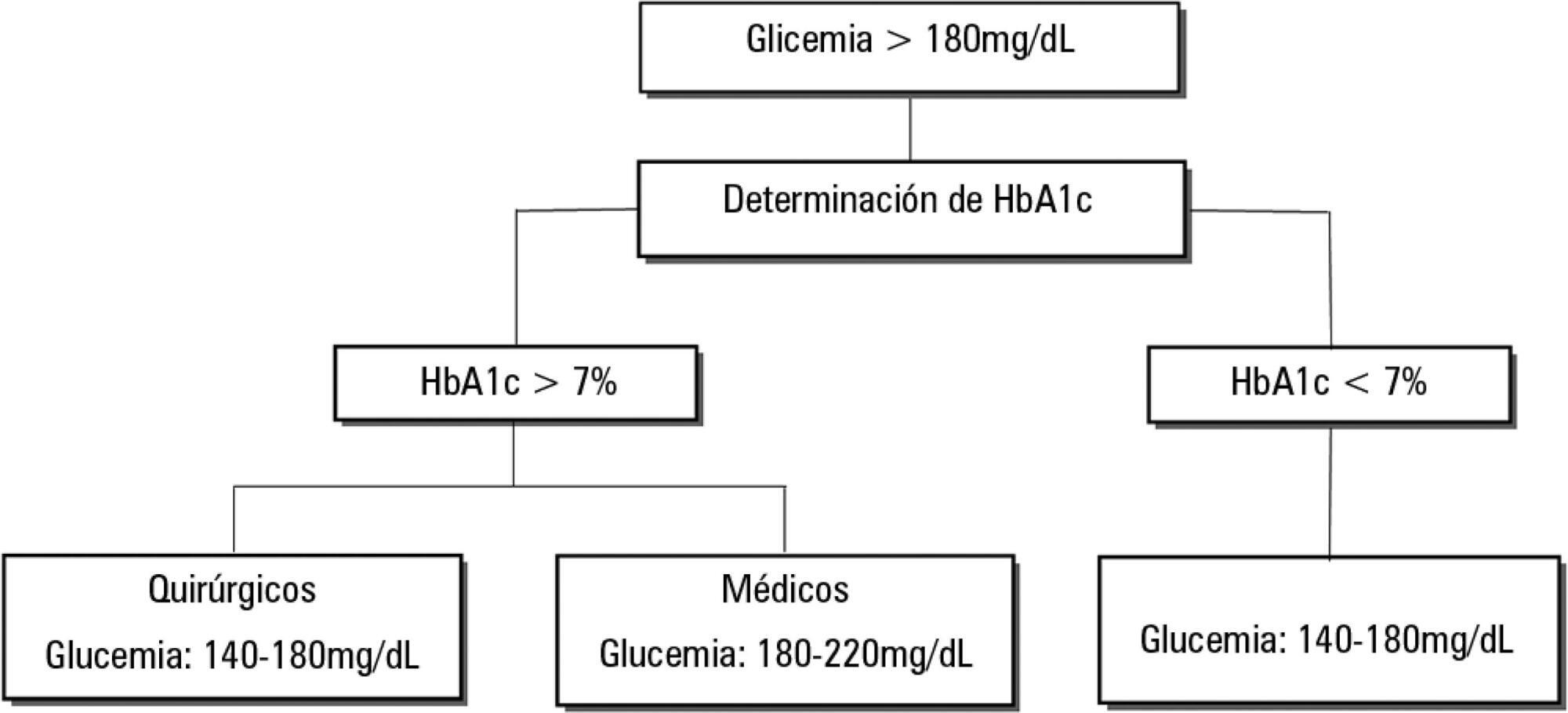
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis