
You searched for:"Flávio Geraldo Rezende de Freitas"
We found (6) results for your search.-
Original Article
Resuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
- Flavio Geraldo Rezende de Freitas
 ,
, - Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti , [ … ],
- Flavia Ribeiro Machado
Abstract
Original ArticleResuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
Rev Bras Ter Intensiva. 2021;33(2):206-218
DOI 10.5935/0103-507X.20210028
- Flavio Geraldo Rezende de Freitas ,
- Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti ,
- Leandro Taniguchi ,
- André Gobatto,
- André Miguel Japiassú ,
- Antonio Tonete Bafi,
- Bruno Franco Mazza,
- Danilo Teixeira Noritomi,
- Felipe Dal-Pizzol ,
- Fernando Bozza ,
- Jorge Ibrahin Figueira Salluh ,
- Glauco Adrieno Westphal ,
- Márcio Soares ,
- Murillo Santucci César de Assunção ,
- Thiago Lisboa,
- Suzana Margarete Ajeje Lobo,
- Achilles Rohlfs Barbosa,
- Adriana Fonseca Ventura,
- Ailson Faria de Souza,
- Alexandre Francisco Silva,
- Alexandre Toledo,
- Aline Reis,
- Allan Cembranel,
- Alvaro Rea Neto,
- Ana Lúcia Gut,
- Ana Patricia Pierre Justo,
- Ana Paula Santos,
- André Campos D. de Albuquerque,
- André Scazufka,
- Antonio Babo Rodrigues,
- Bruno Bonaccorsi Fernandino,
- Bruno Goncalves Silva,
- Bruno Sarno Vidal,
- Bruno Valle Pinheiro,
- Bruno Vilela Costa Pinto,
- Carlos Augusto Ramos Feijo,
- Carlos de Abreu Filho,
- Carlos Eduardo da Costa Nunes Bosso,
- Carlos Eduardo Nassif Moreira,
- Carlos Henrique Ferreira Ramos,
- Carmen Tavares,
- Cidamaiá Arantes,
- Cintia Grion,
- Ciro Leite Mendes,
- Claudio Kmohan,
- Claudio Piras,
- Cristine Pilati Pileggi Castro,
- Cyntia Lins,
- Daniel Beraldo,
- Daniel Fontes,
- Daniela Boni,
- Débora Castiglioni,
- Denise de Moraes Paisani,
- Durval Ferreira Fonseca Pedroso,
- Ederson Roberto Mattos,
- Edgar de Brito Sobrinho,
- Edgar M. V. Troncoso,
- Edison Moraes Rodrigues Filho,
- Eduardo Enrico Ferrari Nogueira,
- Eduardo Leme Ferreira,
- Eduardo Souza Pacheco,
- Euzebio Jodar,
- Evandro L. A. Ferreira,
- Fabiana Fernandes de Araujo,
- Fabiana Schuelter Trevisol,
- Fábio Ferreira Amorim,
- Fabio Poianas Giannini,
- Fabrício Primitivo Matos Santos,
- Fátima Buarque,
- Felipe Gallego Lima,
- Fernando Antonio Alvares da Costa,
- Fernando Cesar dos Anjos Sad,
- Fernando G. Aranha,
- Fernando Ganem,
- Flavio Callil,
- Francisco Flávio Costa Filho,
- Frederico Toledo Campo Dall´Arto,
- Geovani Moreno,
- Gilberto Friedman,
- Giulliana Martines Moralez,
- Guilherme Abdalla da Silva,
- Guilherme Costa,
- Guilherme Silva Cavalcanti,
- Guilherme Silva Cavalcanti,
- Gustavo Navarro Betônico,
- Gustavo Navarro Betônico,
- Hélder Reis,
- Helia Beatriz N. Araujo,
- Helio Anjos Hortiz Júnior,
- Helio Penna Guimaraes,
- Hugo Urbano,
- Israel Maia,
- Ivan Lopes Santiago Filho,
- Jamil Farhat Júnior,
- Janu Rangel Alvarez,
- Joel Tavares Passos,
- Jorge Eduardo da Rocha Paranhos,
- José Aurelio Marques,
- José Gonçalves Moreira Filho,
- Jose Neto Andrade,
- José Onofre de C Sobrinho,
- Jose Terceiro de Paiva Bezerra,
- Juliana Apolônio Alves,
- Juliana Ferreira,
- Jussara Gomes,
- Karina Midori Sato,
- Karine Gerent,
- Kathia Margarida Costa Teixeira,
- Katia Aparecida Pessoa Conde,
- Laércia Ferreira Martins,
- Lanese Figueirêdo,
- Leila Rezegue,
- Leonardo Tcherniacovsk,
- Leone Oliveira Ferraz,
- Liane Cavalcante,
- Ligia Rabelo,
- Lilian Miilher,
- Lisiane Garcia,
- Luana Tannous,
- Ludhmila Abrahão Hajjar,
- Luís Eduardo Miranda Paciência,
- Luiz Monteiro da Cruz Neto,
- Macia Valeria Bley,
- Marcelo Ferreira Sousa,
- Marcelo Lourencini Puga,
- Marcelo Luz Pereira Romano,
- Marciano Nobrega,
- Marcio Arbex,
- Márcio Leite Rodrigues,
- Márcio Osório Guerreiro,
- Marcone Rocha,
- Maria Angela Pangoni Alves,
- Maria Angela Pangoni Alves,
- Maria Doroti Rosa,
- Mariza D’Agostino Dias,
- Miquéias Martins,
- Mirella de Oliveira,
- Miriane Melo Silveira Moretti,
- Mirna Matsui,
- Octavio Messender,
- Orlando Luís de Andrade Santarém,
- Patricio Júnior Henrique da Silveira,
- Paula Frizera Vassallo,
- Paulo Antoniazzi,
- Paulo César Gottardo,
- Paulo Correia,
- Paulo Ferreira,
- Paulo Torres,
- Pedro Gabrile M. de Barros e Silva,
- Rafael Foernges,
- Rafael Gomes,
- Rafael Moraes,
- Raimundo Nonato filho,
- Renato Luis Borba,
- Renato V Gomes,
- Ricardo Cordioli,
- Ricardo Lima,
- Ricardo Pérez López,
- Ricardo Rath de Oliveira Gargioni,
- Richard Rosenblat,
- Roberta Machado de Souza,
- Roberto Almeida,
- Roberto Camargo Narciso,
- Roberto Marco,
- Roberto waltrick,
- Rodrigo Biondi,
- Rodrigo Figueiredo,
- Rodrigo Santana Dutra,
- Roseane Batista,
- Rouge Felipe,
- Rubens Sergio da Silva Franco,
- Sandra Houly,
- Sara Socorro Faria,
- Sergio Felix Pinto,
- Sergio Luzzi,
- Sergio Sant’ana,
- Sergio Sonego Fernandes,
- Sérgio Yamada,
- Sérgio Zajac,
- Sidiner Mesquita Vaz,
- Silvia Aparecida Bezerra Bezerra,
- Tatiana Bueno Tardivo Farhat,
- Thiago Martins Santos,
- Tiago Smith,
- Ulysses V. A. Silva,
- Valnei Bento Damasceno,
- Vandack Nobre,
- Vicente Cés de Souza Dantas,
- Vivian Menezes Irineu,
- Viviane Bogado,
- Wagner Nedel,
- Walther Campos Filho,
- Weidson Dantas,
- William Viana,
- Wilson de Oliveira Filho,
- Wilson Martins Delgadinho,
- Simon Finfer,
- Flavia Ribeiro Machado
Views1See moreAbstract
Objective:
To describe fluid resuscitation practices in Brazilian intensive care units and to compare them with those of other countries participating in the Fluid-TRIPS.
Methods:
This was a prospective, international, cross-sectional, observational study in a convenience sample of intensive care units in 27 countries (including Brazil) using the Fluid-TRIPS database compiled in 2014. We described the patterns of fluid resuscitation use in Brazil compared with those in other countries and identified the factors associated with fluid choice.
Results:
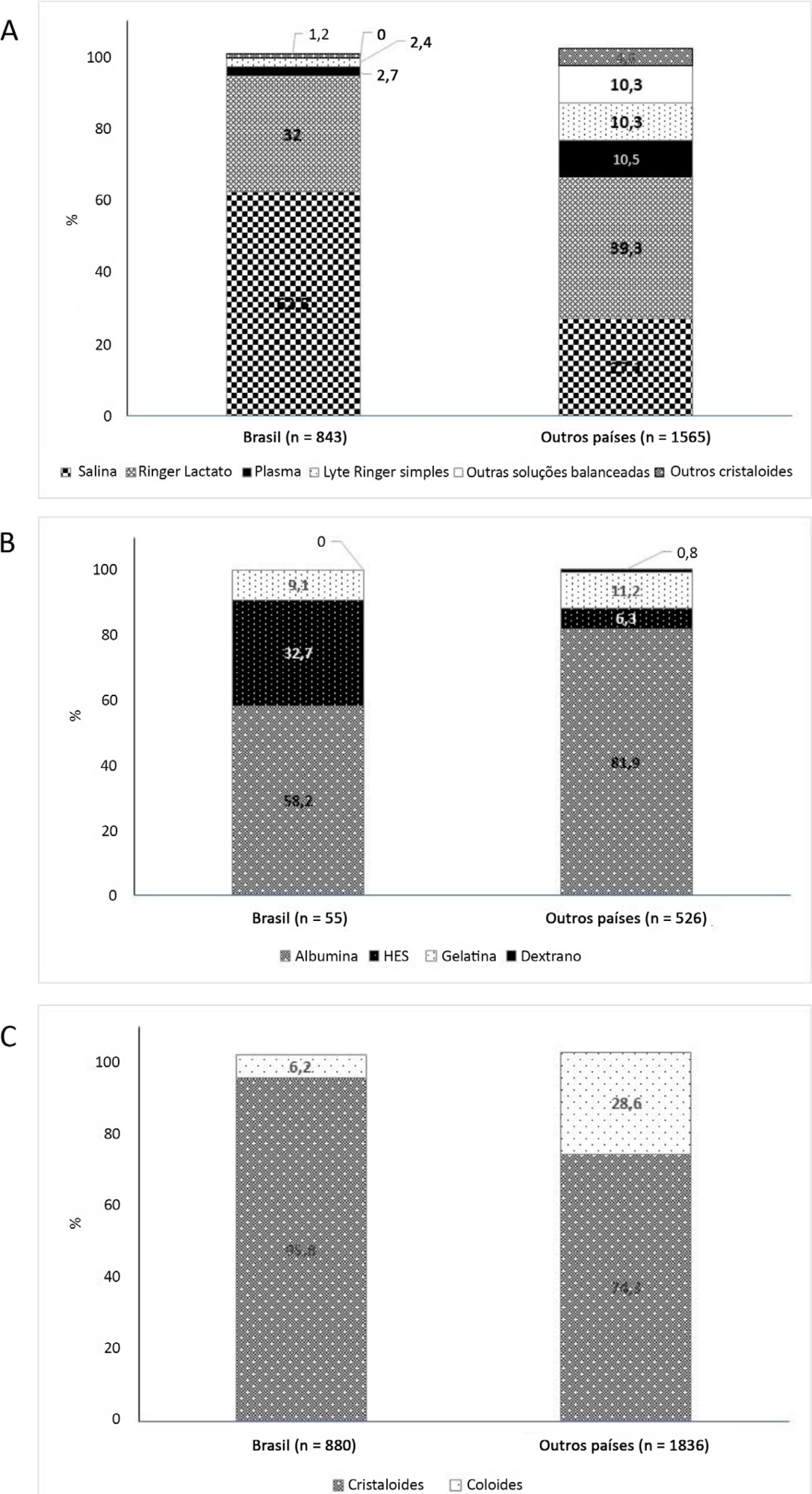
On the study day, 3,214 patients in Brazil and 3,493 patients in other countries were included, of whom 16.1% and 26.8% (p < 0.001) received fluids, respectively. The main indication for fluid resuscitation was impaired perfusion and/or low cardiac output (Brazil: 71.7% versus other countries: 56.4%, p < 0.001). In Brazil, the percentage of patients receiving crystalloid solutions was higher (97.7% versus 76.8%, p < 0.001), and 0.9% sodium chloride was the most commonly used crystalloid (62.5% versus 27.1%, p < 0.001). The multivariable analysis suggested that the albumin levels were associated with the use of both crystalloids and colloids, whereas the type of fluid prescriber was associated with crystalloid use only.
Conclusion:
Our results suggest that crystalloids are more frequently used than colloids for fluid resuscitation in Brazil, and this discrepancy in frequencies is higher than that in other countries. Sodium chloride (0.9%) was the crystalloid most commonly prescribed. Serum albumin levels and the type of fluid prescriber were the factors associated with the choice of crystalloids or colloids for fluid resuscitation.
Views1

Abstract
Original ArticleResuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
Rev Bras Ter Intensiva. 2021;33(2):206-218
DOI 10.5935/0103-507X.20210028
- Flavio Geraldo Rezende de Freitas ,
- Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti ,
- Leandro Taniguchi ,
- André Gobatto,
- André Miguel Japiassú ,
- Antonio Tonete Bafi,
- Bruno Franco Mazza,
- Danilo Teixeira Noritomi,
- Felipe Dal-Pizzol ,
- Fernando Bozza ,
- Jorge Ibrahin Figueira Salluh ,
- Glauco Adrieno Westphal ,
- Márcio Soares ,
- Murillo Santucci César de Assunção ,
- Thiago Lisboa,
- Suzana Margarete Ajeje Lobo,
- Achilles Rohlfs Barbosa,
- Adriana Fonseca Ventura,
- Ailson Faria de Souza,
- Alexandre Francisco Silva,
- Alexandre Toledo,
- Aline Reis,
- Allan Cembranel,
- Alvaro Rea Neto,
- Ana Lúcia Gut,
- Ana Patricia Pierre Justo,
- Ana Paula Santos,
- André Campos D. de Albuquerque,
- André Scazufka,
- Antonio Babo Rodrigues,
- Bruno Bonaccorsi Fernandino,
- Bruno Goncalves Silva,
- Bruno Sarno Vidal,
- Bruno Valle Pinheiro,
- Bruno Vilela Costa Pinto,
- Carlos Augusto Ramos Feijo,
- Carlos de Abreu Filho,
- Carlos Eduardo da Costa Nunes Bosso,
- Carlos Eduardo Nassif Moreira,
- Carlos Henrique Ferreira Ramos,
- Carmen Tavares,
- Cidamaiá Arantes,
- Cintia Grion,
- Ciro Leite Mendes,
- Claudio Kmohan,
- Claudio Piras,
- Cristine Pilati Pileggi Castro,
- Cyntia Lins,
- Daniel Beraldo,
- Daniel Fontes,
- Daniela Boni,
- Débora Castiglioni,
- Denise de Moraes Paisani,
- Durval Ferreira Fonseca Pedroso,
- Ederson Roberto Mattos,
- Edgar de Brito Sobrinho,
- Edgar M. V. Troncoso,
- Edison Moraes Rodrigues Filho,
- Eduardo Enrico Ferrari Nogueira,
- Eduardo Leme Ferreira,
- Eduardo Souza Pacheco,
- Euzebio Jodar,
- Evandro L. A. Ferreira,
- Fabiana Fernandes de Araujo,
- Fabiana Schuelter Trevisol,
- Fábio Ferreira Amorim,
- Fabio Poianas Giannini,
- Fabrício Primitivo Matos Santos,
- Fátima Buarque,
- Felipe Gallego Lima,
- Fernando Antonio Alvares da Costa,
- Fernando Cesar dos Anjos Sad,
- Fernando G. Aranha,
- Fernando Ganem,
- Flavio Callil,
- Francisco Flávio Costa Filho,
- Frederico Toledo Campo Dall´Arto,
- Geovani Moreno,
- Gilberto Friedman,
- Giulliana Martines Moralez,
- Guilherme Abdalla da Silva,
- Guilherme Costa,
- Guilherme Silva Cavalcanti,
- Guilherme Silva Cavalcanti,
- Gustavo Navarro Betônico,
- Gustavo Navarro Betônico,
- Hélder Reis,
- Helia Beatriz N. Araujo,
- Helio Anjos Hortiz Júnior,
- Helio Penna Guimaraes,
- Hugo Urbano,
- Israel Maia,
- Ivan Lopes Santiago Filho,
- Jamil Farhat Júnior,
- Janu Rangel Alvarez,
- Joel Tavares Passos,
- Jorge Eduardo da Rocha Paranhos,
- José Aurelio Marques,
- José Gonçalves Moreira Filho,
- Jose Neto Andrade,
- José Onofre de C Sobrinho,
- Jose Terceiro de Paiva Bezerra,
- Juliana Apolônio Alves,
- Juliana Ferreira,
- Jussara Gomes,
- Karina Midori Sato,
- Karine Gerent,
- Kathia Margarida Costa Teixeira,
- Katia Aparecida Pessoa Conde,
- Laércia Ferreira Martins,
- Lanese Figueirêdo,
- Leila Rezegue,
- Leonardo Tcherniacovsk,
- Leone Oliveira Ferraz,
- Liane Cavalcante,
- Ligia Rabelo,
- Lilian Miilher,
- Lisiane Garcia,
- Luana Tannous,
- Ludhmila Abrahão Hajjar,
- Luís Eduardo Miranda Paciência,
- Luiz Monteiro da Cruz Neto,
- Macia Valeria Bley,
- Marcelo Ferreira Sousa,
- Marcelo Lourencini Puga,
- Marcelo Luz Pereira Romano,
- Marciano Nobrega,
- Marcio Arbex,
- Márcio Leite Rodrigues,
- Márcio Osório Guerreiro,
- Marcone Rocha,
- Maria Angela Pangoni Alves,
- Maria Angela Pangoni Alves,
- Maria Doroti Rosa,
- Mariza D’Agostino Dias,
- Miquéias Martins,
- Mirella de Oliveira,
- Miriane Melo Silveira Moretti,
- Mirna Matsui,
- Octavio Messender,
- Orlando Luís de Andrade Santarém,
- Patricio Júnior Henrique da Silveira,
- Paula Frizera Vassallo,
- Paulo Antoniazzi,
- Paulo César Gottardo,
- Paulo Correia,
- Paulo Ferreira,
- Paulo Torres,
- Pedro Gabrile M. de Barros e Silva,
- Rafael Foernges,
- Rafael Gomes,
- Rafael Moraes,
- Raimundo Nonato filho,
- Renato Luis Borba,
- Renato V Gomes,
- Ricardo Cordioli,
- Ricardo Lima,
- Ricardo Pérez López,
- Ricardo Rath de Oliveira Gargioni,
- Richard Rosenblat,
- Roberta Machado de Souza,
- Roberto Almeida,
- Roberto Camargo Narciso,
- Roberto Marco,
- Roberto waltrick,
- Rodrigo Biondi,
- Rodrigo Figueiredo,
- Rodrigo Santana Dutra,
- Roseane Batista,
- Rouge Felipe,
- Rubens Sergio da Silva Franco,
- Sandra Houly,
- Sara Socorro Faria,
- Sergio Felix Pinto,
- Sergio Luzzi,
- Sergio Sant’ana,
- Sergio Sonego Fernandes,
- Sérgio Yamada,
- Sérgio Zajac,
- Sidiner Mesquita Vaz,
- Silvia Aparecida Bezerra Bezerra,
- Tatiana Bueno Tardivo Farhat,
- Thiago Martins Santos,
- Tiago Smith,
- Ulysses V. A. Silva,
- Valnei Bento Damasceno,
- Vandack Nobre,
- Vicente Cés de Souza Dantas,
- Vivian Menezes Irineu,
- Viviane Bogado,
- Wagner Nedel,
- Walther Campos Filho,
- Weidson Dantas,
- William Viana,
- Wilson de Oliveira Filho,
- Wilson Martins Delgadinho,
- Simon Finfer,
- Flavia Ribeiro Machado
Views1See moreAbstract
Objective:
To describe fluid resuscitation practices in Brazilian intensive care units and to compare them with those of other countries participating in the Fluid-TRIPS.
Methods:
This was a prospective, international, cross-sectional, observational study in a convenience sample of intensive care units in 27 countries (including Brazil) using the Fluid-TRIPS database compiled in 2014. We described the patterns of fluid resuscitation use in Brazil compared with those in other countries and identified the factors associated with fluid choice.
Results:
On the study day, 3,214 patients in Brazil and 3,493 patients in other countries were included, of whom 16.1% and 26.8% (p < 0.001) received fluids, respectively. The main indication for fluid resuscitation was impaired perfusion and/or low cardiac output (Brazil: 71.7% versus other countries: 56.4%, p < 0.001). In Brazil, the percentage of patients receiving crystalloid solutions was higher (97.7% versus 76.8%, p < 0.001), and 0.9% sodium chloride was the most commonly used crystalloid (62.5% versus 27.1%, p < 0.001). The multivariable analysis suggested that the albumin levels were associated with the use of both crystalloids and colloids, whereas the type of fluid prescriber was associated with crystalloid use only.
Conclusion:
Our results suggest that crystalloids are more frequently used than colloids for fluid resuscitation in Brazil, and this discrepancy in frequencies is higher than that in other countries. Sodium chloride (0.9%) was the crystalloid most commonly prescribed. Serum albumin levels and the type of fluid prescriber were the factors associated with the choice of crystalloids or colloids for fluid resuscitation.
- Flavio Geraldo Rezende de Freitas
-
Original Article
Statistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo, [ … ],
- Fernando Godinho Zampieri
Abstract
Original ArticleStatistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
Rev Bras Ter Intensiva. 2020;32(4):493-505
DOI 10.5935/0103-507X.20200081
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo,
- Wilson José Lovato,
- Cristina Prata Amêndola,
- Ary Serpa Neto ,
- Jorge Luiz da Rocha Paranhos,
- Viviane Cordeiro Veiga ,
- Marco Antonio Vieira Guedes,
- Eraldo de Azevedo Lúcio,
- Lúcio Couto Oliveira Júnior,
- Thiago Costa Lisboa,
- Fabio Holanda Lacerda ,
- Tamiris Abait Miranda,
- Israel Silva Maia ,
- Cintia Magalhães Carvalho Grion ,
- Flavia Ribeiro Machado,
- Fernando Godinho Zampieri
Views1See moreAbstract
Objective:
To report the statistical analysis plan (first version) for the Balanced Solutions versus Saline in Intensive Care Study (BaSICS).
Methods:
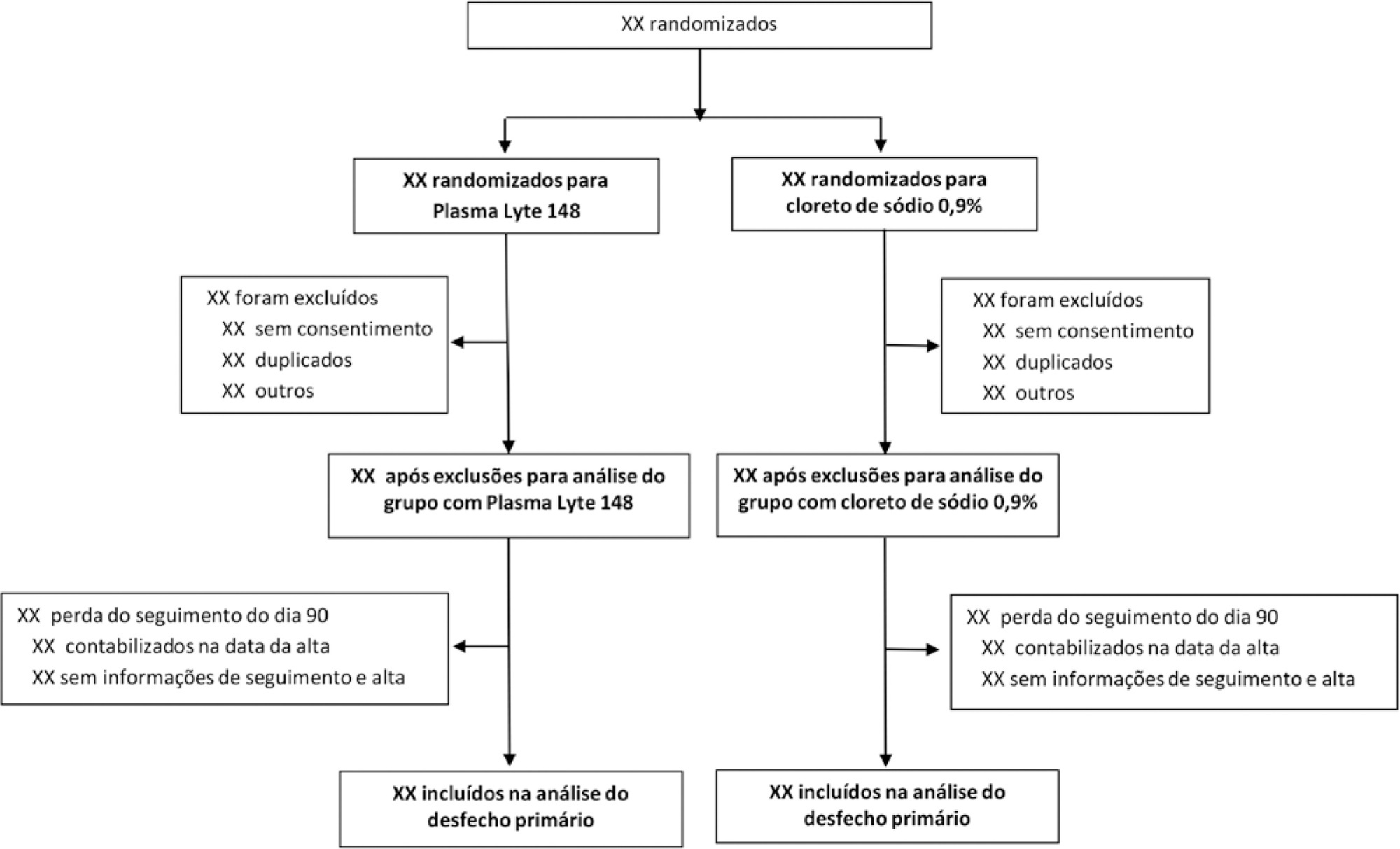
BaSICS is a multicenter factorial randomized controlled trial that will assess the effects of Plasma-Lyte 148 versus 0.9% saline as the fluid of choice in critically ill patients, as well as the effects of a slow (333mL/h) versus rapid (999mL/h) infusion speed during fluid challenges, on important patient outcomes. The fluid type will be blinded for investigators, patients and the analyses. No blinding will be possible for the infusion speed for the investigators, but all analyses will be kept blinded during the analysis procedure.
Results:
BaSICS will have 90-day mortality as its primary endpoint, which will be tested using mixed-effects Cox proportional hazard models, considering sites as a random variable (frailty models) adjusted for age, organ dysfunction and admission type. Important secondary endpoints include renal replacement therapy up to 90 days, acute renal failure, organ dysfunction at days 3 and 7, and mechanical ventilation-free days within 28 days.
Conclusion:
This manuscript provides details on the first version of the statistical analysis plan for the BaSICS trial and will guide the study’s analysis when follow-up is finished.
Views1Abstract
Original ArticleStatistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
Rev Bras Ter Intensiva. 2020;32(4):493-505
DOI 10.5935/0103-507X.20200081
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo,
- Wilson José Lovato,
- Cristina Prata Amêndola,
- Ary Serpa Neto ,
- Jorge Luiz da Rocha Paranhos,
- Viviane Cordeiro Veiga ,
- Marco Antonio Vieira Guedes,
- Eraldo de Azevedo Lúcio,
- Lúcio Couto Oliveira Júnior,
- Thiago Costa Lisboa,
- Fabio Holanda Lacerda ,
- Tamiris Abait Miranda,
- Israel Silva Maia ,
- Cintia Magalhães Carvalho Grion ,
- Flavia Ribeiro Machado,
- Fernando Godinho Zampieri
Views1See moreAbstract
Objective:
To report the statistical analysis plan (first version) for the Balanced Solutions versus Saline in Intensive Care Study (BaSICS).
Methods:
BaSICS is a multicenter factorial randomized controlled trial that will assess the effects of Plasma-Lyte 148 versus 0.9% saline as the fluid of choice in critically ill patients, as well as the effects of a slow (333mL/h) versus rapid (999mL/h) infusion speed during fluid challenges, on important patient outcomes. The fluid type will be blinded for investigators, patients and the analyses. No blinding will be possible for the infusion speed for the investigators, but all analyses will be kept blinded during the analysis procedure.
Results:
BaSICS will have 90-day mortality as its primary endpoint, which will be tested using mixed-effects Cox proportional hazard models, considering sites as a random variable (frailty models) adjusted for age, organ dysfunction and admission type. Important secondary endpoints include renal replacement therapy up to 90 days, acute renal failure, organ dysfunction at days 3 and 7, and mechanical ventilation-free days within 28 days.
Conclusion:
This manuscript provides details on the first version of the statistical analysis plan for the BaSICS trial and will guide the study’s analysis when follow-up is finished.
-
Original Article
Epidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama, [ … ],
- Suzana Margareth Ajeje Lobo
Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee moreViews1Abstract
Original ArticleEpidemiology and outcome of high-surgical-risk patients admitted to an intensive care unit in Brazil
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
- João Manoel Silva Júnior ,
- Renato Carneiro de Freitas Chaves ,
- Thiago Domingos Corrêa ,
- Murillo Santucci Cesar de Assunção ,
- Henrique Tadashi Katayama,
- Fabio Eduardo Bosso,
- Cristina Prata Amendola,
- Ary Serpa Neto ,
- Luiz Marcelo Sá Malbouisson,
- Neymar Elias de Oliveira,
- Viviane Cordeiro Veiga ,
- Salomón Soriano Ordinola Rojas,
- Natalia Fioravante Postalli,
- Thais Kawagoe Alvarisa,
- Bruno Melo Nobrega de Lucena,
- Raphael Augusto Gomes de Oliveira,
- Luciana Coelho Sanches,
- Ulysses Vasconcellos de Andrade e Silva,
- Antonio Paulo Nassar Junior ,
- Álvaro Réa-Neto,
- Alexandre Amaral,
- José Mário Teles,
- Flávio Geraldo Rezende de Freitas,
- Antônio Tonete Bafi,
- Eduardo Souza Pacheco,
- Fernando José Ramos,
- José Mauro Vieira Júnior,
- Maria Augusta Santos Rahe Pereira,
- Fábio Sartori Schwerz,
- Giovanna Padoa de Menezes,
- Danielle Dourado Magalhães,
- Cristine Pilati Pileggi Castro,
- Sabrina Frighetto Henrich,
- Diogo Oliveira Toledo,
- Bruna Fernanda Camargo Silva Parra,
- Fernando Suparregui Dias ,
- Luiza Zerman,
- Fernanda Formolo,
- Marciano de Sousa Nobrega,
- Claudio Piras,
- Stéphanie de Barros Piras,
- Rodrigo Conti,
- Paulo Lisboa Bittencourt,
- Ricardo Azevedo Cruz D’Oliveira,
- André Ricardo de Oliveira Estrela,
- Mirella Cristine de Oliveira,
- Fernanda Baeumle Reese,
- Jarbas da Silva Motta Júnior,
- Bruna Martins Dzivielevski da Câmara,
- Paula Geraldes David-João,
- Luana Alves Tannous,
- Viviane Bernardes de Oliveira Chaiben,
- Lorena Macedo Araújo Miranda,
- José Arthur dos Santos Brasil,
- Rafael Alexandre de Oliveira Deucher,
- Marcos Henrique Borges Ferreira,
- Denner Luiz Vilela,
- Guilherme Cincinato de Almeida,
- Wagner Luis Nedel ,
- Matheus Golenia dos Passos,
- Luiz Gustavo Marin,
- Wilson de Oliveira Filho,
- Raoni Machado Coutinho,
- Michele Cristina Lima de Oliveira,
- Gilberto Friedman,
- André Meregalli,
- Jorge Amilton Höher,
- Afonso José Celente Soares,
- Suzana Margareth Ajeje Lobo
Views1ABSTRACT
Objective:
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
Methods:
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Results:
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval – 95%CI 3.3% – 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 – 4.0) days, and the length of hospital stay was 9.5 (5.4 – 18.6) days. The complication rate was 29.9% (95%CI 26.4 – 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 – 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio – OR = 1.02; 95%CI 1.01 – 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 – 1.25), surgical time (OR = 1.001, 95%CI 1.000 – 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 – 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 – 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 – 1.279), SOFA (OR = 1.175, 95%CI 1.069 – 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 – 6.051).
Conclusion:
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Keywords:BrazilIntensive care unitspostoperative carePostoperative complications/mortalitySurgical procedures, operative/epidemiologySurgical procedures, operative/mortalitySee more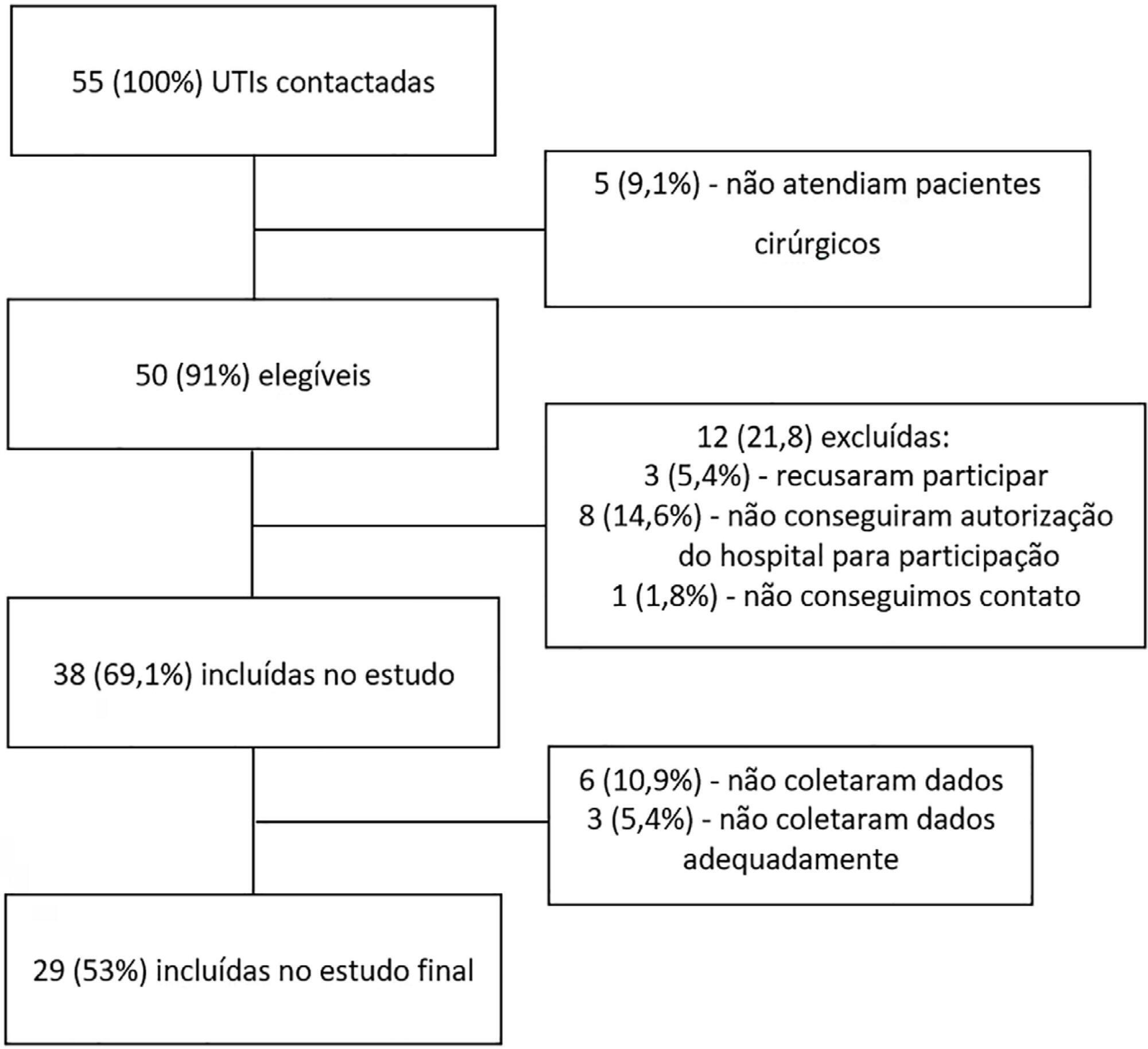
- João Manoel Silva Júnior
-
Original Articles
Prevalence of cytomegalovirus disease in kidney transplant patients in an intensive care unit
Rev Bras Ter Intensiva. 2017;29(4):436-443
Abstract
Original ArticlesPrevalence of cytomegalovirus disease in kidney transplant patients in an intensive care unit
Rev Bras Ter Intensiva. 2017;29(4):436-443
DOI 10.5935/0103-507X.20170070
Views0See moreABSTRACT
Objectives:
To define the frequency of cytomegalovirus disease among kidney transplant patients in an intensive care unit in which this complication was suspected and to identify predisposing factors and their possible impact on clinical outcome.
Methods:
Retrospective observational study in which kidney transplant patients over the age of 18 years were hospitalized for any reason in an intensive care unit with at least one collection of samples to test for the presence of antigenemia or cytomegalovirus via polymerase chain reaction during hospitalization. Cytomegalovirus disease was defined as positive antigenemia or polymerase chain reaction above 500 copies/mL in the presence of symptoms and in the appropriate clinical setting, as judged by the attending physician.
Results:
A total of 99 patients were included (age: 53.4 ± 12.8 years, 71.6% male). Cytomegalovirus disease was diagnosed in 39 patients (39.4%). Respiratory symptoms (51%), non-specific clinical worsening (20%) or gastrointestinal symptoms (14%) were the main reasons for exam collection. Transplant time was lower in those with cytomegalovirus disease than in those without this diagnosis (6.5 months and 31.2 months, p = 0.001), along with pulse therapy in the last 6 months (41% and 16.9%, p = 0.008) and previous use of thymoglobulin in the last year (35.9% and 6.8%, p < 0.001). In the logistic regression model, only the transplant time and the use of thymoglobulin were associated with a higher frequency of cytomegalovirus. There was no difference in clinical evolution between patients with and without cytomegalovirus disease.
Conclusion:
In kidney transplant patients suspected of cytomegalovirus disease, the prevalence was high. Transplant time less than 6 months, and the use of thymoglobulin in the last year should increase the intensivist’s suspicion for this complication.
Views0Abstract
Original ArticlesPrevalence of cytomegalovirus disease in kidney transplant patients in an intensive care unit
Rev Bras Ter Intensiva. 2017;29(4):436-443
DOI 10.5935/0103-507X.20170070
Views0See moreABSTRACT
Objectives:
To define the frequency of cytomegalovirus disease among kidney transplant patients in an intensive care unit in which this complication was suspected and to identify predisposing factors and their possible impact on clinical outcome.
Methods:
Retrospective observational study in which kidney transplant patients over the age of 18 years were hospitalized for any reason in an intensive care unit with at least one collection of samples to test for the presence of antigenemia or cytomegalovirus via polymerase chain reaction during hospitalization. Cytomegalovirus disease was defined as positive antigenemia or polymerase chain reaction above 500 copies/mL in the presence of symptoms and in the appropriate clinical setting, as judged by the attending physician.
Results:
A total of 99 patients were included (age: 53.4 ± 12.8 years, 71.6% male). Cytomegalovirus disease was diagnosed in 39 patients (39.4%). Respiratory symptoms (51%), non-specific clinical worsening (20%) or gastrointestinal symptoms (14%) were the main reasons for exam collection. Transplant time was lower in those with cytomegalovirus disease than in those without this diagnosis (6.5 months and 31.2 months, p = 0.001), along with pulse therapy in the last 6 months (41% and 16.9%, p = 0.008) and previous use of thymoglobulin in the last year (35.9% and 6.8%, p < 0.001). In the logistic regression model, only the transplant time and the use of thymoglobulin were associated with a higher frequency of cytomegalovirus. There was no difference in clinical evolution between patients with and without cytomegalovirus disease.
Conclusion:
In kidney transplant patients suspected of cytomegalovirus disease, the prevalence was high. Transplant time less than 6 months, and the use of thymoglobulin in the last year should increase the intensivist’s suspicion for this complication.
-
Jugular vein distensibility, a noninvasive parameter of fluid responsiveness?
Rev Bras Ter Intensiva. 2015;27(3):190-192
Abstract
Jugular vein distensibility, a noninvasive parameter of fluid responsiveness?
Rev Bras Ter Intensiva. 2015;27(3):190-192
DOI 10.5935/0103-507X.20150039
Views0Most critically ill patients in intensive care units (ICU) require fluid administration for volume expansion at some point during their hospital stay.() In most cases, initial volume expansion does not require more sophisticated or invasive measures. Clinical history data and clinical signs of low flow may suggest the likelihood of a response to the initial […]See moreViews0Abstract
Jugular vein distensibility, a noninvasive parameter of fluid responsiveness?
Rev Bras Ter Intensiva. 2015;27(3):190-192
DOI 10.5935/0103-507X.20150039
Views0Most critically ill patients in intensive care units (ICU) require fluid administration for volume expansion at some point during their hospital stay.() In most cases, initial volume expansion does not require more sophisticated or invasive measures. Clinical history data and clinical signs of low flow may suggest the likelihood of a response to the initial […]See more -
Original Article
Is venous blood drawn from femoral access adequate to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients?
Rev Bras Ter Intensiva. 2015;27(4):340-346
Abstract
Original ArticleIs venous blood drawn from femoral access adequate to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients?
Rev Bras Ter Intensiva. 2015;27(4):340-346
DOI 10.5935/0103-507X.20150058
Views0ABSTRACT
Objectives:
The purpose of this study was to test if venous blood drawn from femoral access can be used to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients.
Methods:
Bland-Altman analysis and Spearman correlations were used to compare the femoral venous oxygen saturation and central venous oxygen saturation as well as arterial lactate levels and femoral lactate. A pre-specified subgroup analysis was conducted in patients with signs of hypoperfusion. In addition, the clinical agreement was also investigated.
Results:
Blood samples were obtained in 26 patients. In 107 paired samples, there was a moderate correlation (r = 0.686, p < 0.0001) between the central venous oxygen saturation and femoral venous oxygen saturation with a bias of 8.24 ± 10.44 (95% limits of agreement: -12.23 to 28.70). In 102 paired samples, there was a strong correlation between the arterial lactate levels and femoral lactate levels (r = 0.972, p < 0.001) with a bias of -2.71 ± 9.86 (95% limits of agreement: -22.03 to 16.61). The presence of hypoperfusion did not significantly change these results. The clinical agreement for venous saturation was inadequate, with different therapeutic decisions in 22.4% of the situation; for lactate, this was the case only in 5.2% of the situations.
Conclusion:
Femoral venous oxygen saturation should not be used as a surrogate of central venous oxygen saturation. However, femoral lactate levels can be used in clinical practice, albeit with caution.
Keywords:Central venous pressure/physiologyFemoral vein/physiologyLactatesOxygen consumption/physiologySee moreViews0Abstract
Original ArticleIs venous blood drawn from femoral access adequate to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients?
Rev Bras Ter Intensiva. 2015;27(4):340-346
DOI 10.5935/0103-507X.20150058
Views0ABSTRACT
Objectives:
The purpose of this study was to test if venous blood drawn from femoral access can be used to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients.
Methods:
Bland-Altman analysis and Spearman correlations were used to compare the femoral venous oxygen saturation and central venous oxygen saturation as well as arterial lactate levels and femoral lactate. A pre-specified subgroup analysis was conducted in patients with signs of hypoperfusion. In addition, the clinical agreement was also investigated.
Results:
Blood samples were obtained in 26 patients. In 107 paired samples, there was a moderate correlation (r = 0.686, p < 0.0001) between the central venous oxygen saturation and femoral venous oxygen saturation with a bias of 8.24 ± 10.44 (95% limits of agreement: -12.23 to 28.70). In 102 paired samples, there was a strong correlation between the arterial lactate levels and femoral lactate levels (r = 0.972, p < 0.001) with a bias of -2.71 ± 9.86 (95% limits of agreement: -22.03 to 16.61). The presence of hypoperfusion did not significantly change these results. The clinical agreement for venous saturation was inadequate, with different therapeutic decisions in 22.4% of the situation; for lactate, this was the case only in 5.2% of the situations.
Conclusion:
Femoral venous oxygen saturation should not be used as a surrogate of central venous oxygen saturation. However, femoral lactate levels can be used in clinical practice, albeit with caution.
Keywords:Central venous pressure/physiologyFemoral vein/physiologyLactatesOxygen consumption/physiologySee more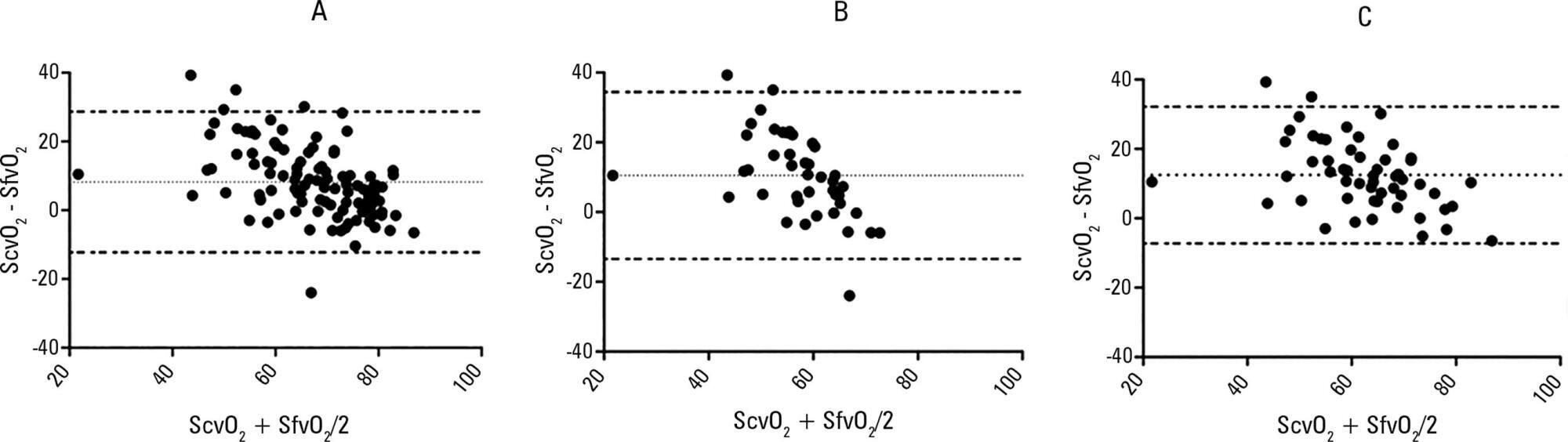
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis