
You searched for:"Andrew Rhodes"
We found (4) results for your search.-
Viewpoint
Why the Sequential Organ Failure Assessment score needs updating?
Crit Care Sci. 2024;36:e20240296en
Abstract
ViewpointWhy the Sequential Organ Failure Assessment score needs updating?
Crit Care Sci. 2024;36:e20240296en
DOI 10.62675/2965-2774.20240296-pt
Views179The Sequential Organ Failure Assessment (SOFA) score was developed almost 30 years ago. It rapidly became one of the most widely used scoring systems in intensive care, both for clinical practice and research,(,) and remains one of the most cited scores in our speciality. Since its original description, there have been substantial changes in clinical […]See moreViews179

Abstract
ViewpointWhy the Sequential Organ Failure Assessment score needs updating?
Crit Care Sci. 2024;36:e20240296en
DOI 10.62675/2965-2774.20240296-pt
Views179The Sequential Organ Failure Assessment (SOFA) score was developed almost 30 years ago. It rapidly became one of the most widely used scoring systems in intensive care, both for clinical practice and research,(,) and remains one of the most cited scores in our speciality. Since its original description, there have been substantial changes in clinical […]See more -
Original Articles
American Society of Anesthesiologists Score: still useful after 60 years? Results of the EuSOS Study
Rev Bras Ter Intensiva. 2015;27(2):105-112
Abstract
Original ArticlesAmerican Society of Anesthesiologists Score: still useful after 60 years? Results of the EuSOS Study
Rev Bras Ter Intensiva. 2015;27(2):105-112
DOI 10.5935/0103-507X.20150020
Views0See moreABSTRACT
Objective:
The European Surgical Outcomes Study described mortality following in-patient surgery. Several factors were identified that were able to predict poor outcomes in a multivariate analysis. These included age, procedure urgency, severity and type and the American Association of Anaesthesia score. This study describes in greater detail the relationship between the American Association of Anaesthesia score and postoperative mortality.
Methods:
Patients in this 7-day cohort study were enrolled in April 2011. Consecutive patients aged 16 years and older undergoing inpatient non-cardiac surgery with a recorded American Association of Anaesthesia score in 498 hospitals across 28 European nations were included and followed up for a maximum of 60 days. The primary endpoint was in-hospital mortality. Decision tree analysis with the CHAID (SPSS) system was used to delineate nodes associated with mortality.
Results:
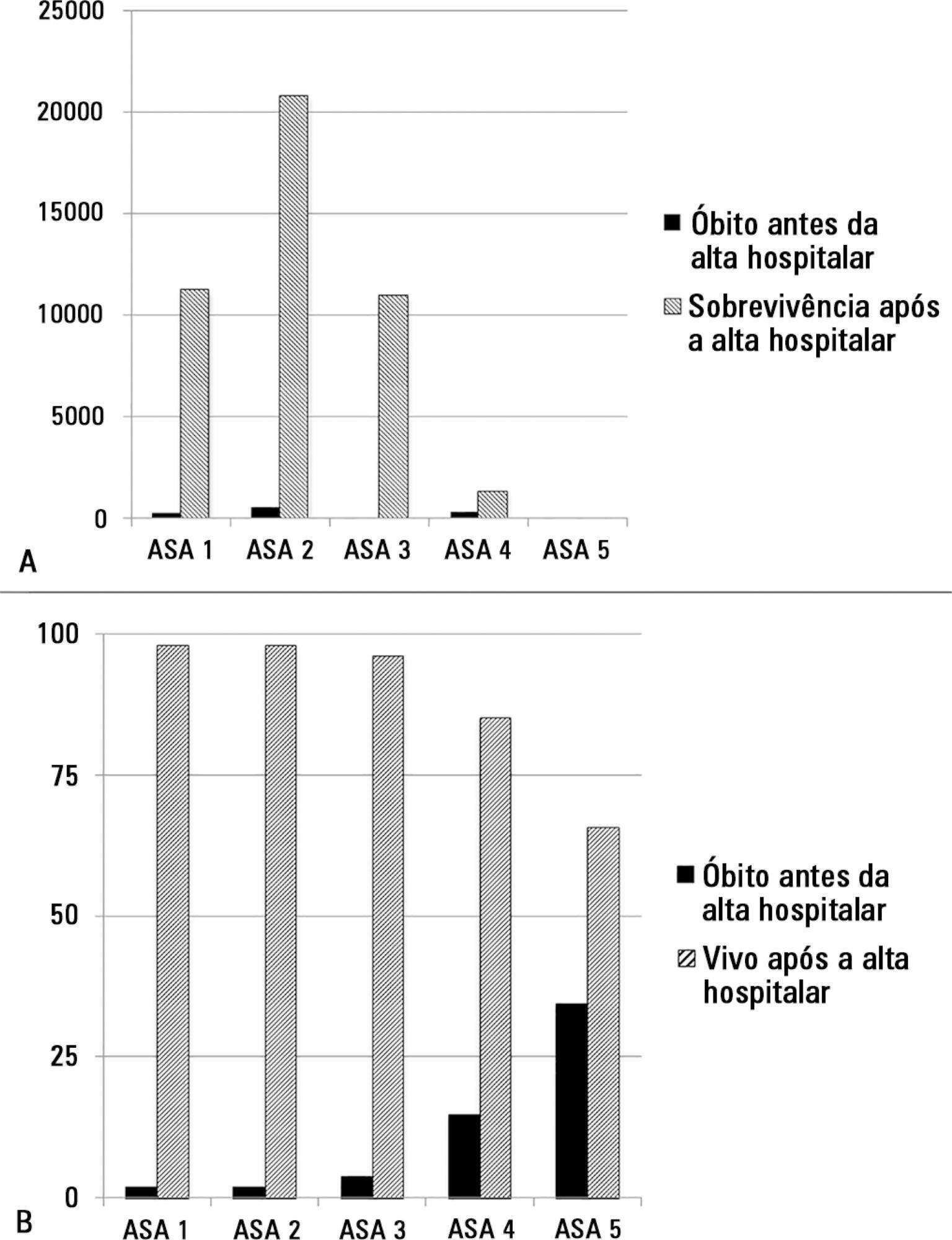
The study enrolled 46,539 patients. Due to missing values, 873 patients were excluded, resulting in the analysis of 45,666 patients. Increasing American Association of Anaesthesia scores were associated with increased admission rates to intensive care and higher mortality rates. Despite a progressive relationship with mortality, discrimination was poor, with an area under the ROC curve of 0.658 (95% CI 0.642 – 0.6775). Using regression trees (CHAID), we identified four discrete American Association of Anaesthesia nodes associated with mortality, with American Association of Anaesthesia 1 and American Association of Anaesthesia 2 compressed into the same node.
Conclusion:
The American Association of Anaesthesia score can be used to determine higher risk groups of surgical patients, but clinicians cannot use the score to discriminate between grades 1 and 2. Overall, the discriminatory power of the model was less than acceptable for widespread use.
Views0Abstract
Original ArticlesAmerican Society of Anesthesiologists Score: still useful after 60 years? Results of the EuSOS Study
Rev Bras Ter Intensiva. 2015;27(2):105-112
DOI 10.5935/0103-507X.20150020
Views0See moreABSTRACT
Objective:
The European Surgical Outcomes Study described mortality following in-patient surgery. Several factors were identified that were able to predict poor outcomes in a multivariate analysis. These included age, procedure urgency, severity and type and the American Association of Anaesthesia score. This study describes in greater detail the relationship between the American Association of Anaesthesia score and postoperative mortality.
Methods:
Patients in this 7-day cohort study were enrolled in April 2011. Consecutive patients aged 16 years and older undergoing inpatient non-cardiac surgery with a recorded American Association of Anaesthesia score in 498 hospitals across 28 European nations were included and followed up for a maximum of 60 days. The primary endpoint was in-hospital mortality. Decision tree analysis with the CHAID (SPSS) system was used to delineate nodes associated with mortality.
Results:
The study enrolled 46,539 patients. Due to missing values, 873 patients were excluded, resulting in the analysis of 45,666 patients. Increasing American Association of Anaesthesia scores were associated with increased admission rates to intensive care and higher mortality rates. Despite a progressive relationship with mortality, discrimination was poor, with an area under the ROC curve of 0.658 (95% CI 0.642 – 0.6775). Using regression trees (CHAID), we identified four discrete American Association of Anaesthesia nodes associated with mortality, with American Association of Anaesthesia 1 and American Association of Anaesthesia 2 compressed into the same node.
Conclusion:
The American Association of Anaesthesia score can be used to determine higher risk groups of surgical patients, but clinicians cannot use the score to discriminate between grades 1 and 2. Overall, the discriminatory power of the model was less than acceptable for widespread use.
-
Review Article
Hemodynamic optimization in severe trauma: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2014;26(4):397-406
Abstract
Review ArticleHemodynamic optimization in severe trauma: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2014;26(4):397-406
DOI 10.5935/0103-507X.20140061
Views0Objective:
Severe trauma can be associated with significant hemorrhagic shock and impaired organ perfusion. We hypothesized that goal-directed therapy would confer morbidity and mortality benefits in major trauma.
Methods:
The MedLine, Embase and Cochrane Controlled Clinical Trials Register databases were systematically searched for randomized, controlled trials of goal-directed therapy in severe trauma patients. Mortality was the primary outcome of this review. Secondary outcomes included complication rates, length of hospital and intensive care unit stay, and the volume of fluid and blood administered. Meta-analysis was performed using RevMan software, and the data presented are as odds ratios for dichotomous outcomes and as mean differences (MDs) and standard MDs for continuous outcomes.
Results:
Four randomized, controlled trials including 419 patients were analyzed. Mortality risk was significantly reduced in goal-directed therapy-treated patients, compared to the control group (OR=0.56, 95%CI: 0.34-0.92). Intensive care (MD: 3.7 days 95%CI: 1.06-6.5) and hospital length of stay (MD: 3.5 days, 95%CI: 2.75-4.25) were significantly shorter in the protocol group patients. There were no differences in reported total fluid volume or blood transfusions administered. Heterogeneity in reporting among the studies prevented quantitative analysis of complications.
Conclusion:
Following severe trauma, early goal-directed therapy was associated with lower mortality and shorter durations of intensive care unit and hospital stays. The findings of this analysis should be interpreted with caution due to the presence of significant heterogeneity and the small number of the randomized, controlled trials included.
Keywords:Fluid therapy/methodsHemodynamics/physiologyShock, hemorrhagicTrauma severity indicesWound and injuriesSee moreViews0Abstract
Review ArticleHemodynamic optimization in severe trauma: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2014;26(4):397-406
DOI 10.5935/0103-507X.20140061
Views0Objective:
Severe trauma can be associated with significant hemorrhagic shock and impaired organ perfusion. We hypothesized that goal-directed therapy would confer morbidity and mortality benefits in major trauma.
Methods:
The MedLine, Embase and Cochrane Controlled Clinical Trials Register databases were systematically searched for randomized, controlled trials of goal-directed therapy in severe trauma patients. Mortality was the primary outcome of this review. Secondary outcomes included complication rates, length of hospital and intensive care unit stay, and the volume of fluid and blood administered. Meta-analysis was performed using RevMan software, and the data presented are as odds ratios for dichotomous outcomes and as mean differences (MDs) and standard MDs for continuous outcomes.
Results:
Four randomized, controlled trials including 419 patients were analyzed. Mortality risk was significantly reduced in goal-directed therapy-treated patients, compared to the control group (OR=0.56, 95%CI: 0.34-0.92). Intensive care (MD: 3.7 days 95%CI: 1.06-6.5) and hospital length of stay (MD: 3.5 days, 95%CI: 2.75-4.25) were significantly shorter in the protocol group patients. There were no differences in reported total fluid volume or blood transfusions administered. Heterogeneity in reporting among the studies prevented quantitative analysis of complications.
Conclusion:
Following severe trauma, early goal-directed therapy was associated with lower mortality and shorter durations of intensive care unit and hospital stays. The findings of this analysis should be interpreted with caution due to the presence of significant heterogeneity and the small number of the randomized, controlled trials included.
Keywords:Fluid therapy/methodsHemodynamics/physiologyShock, hemorrhagicTrauma severity indicesWound and injuriesSee more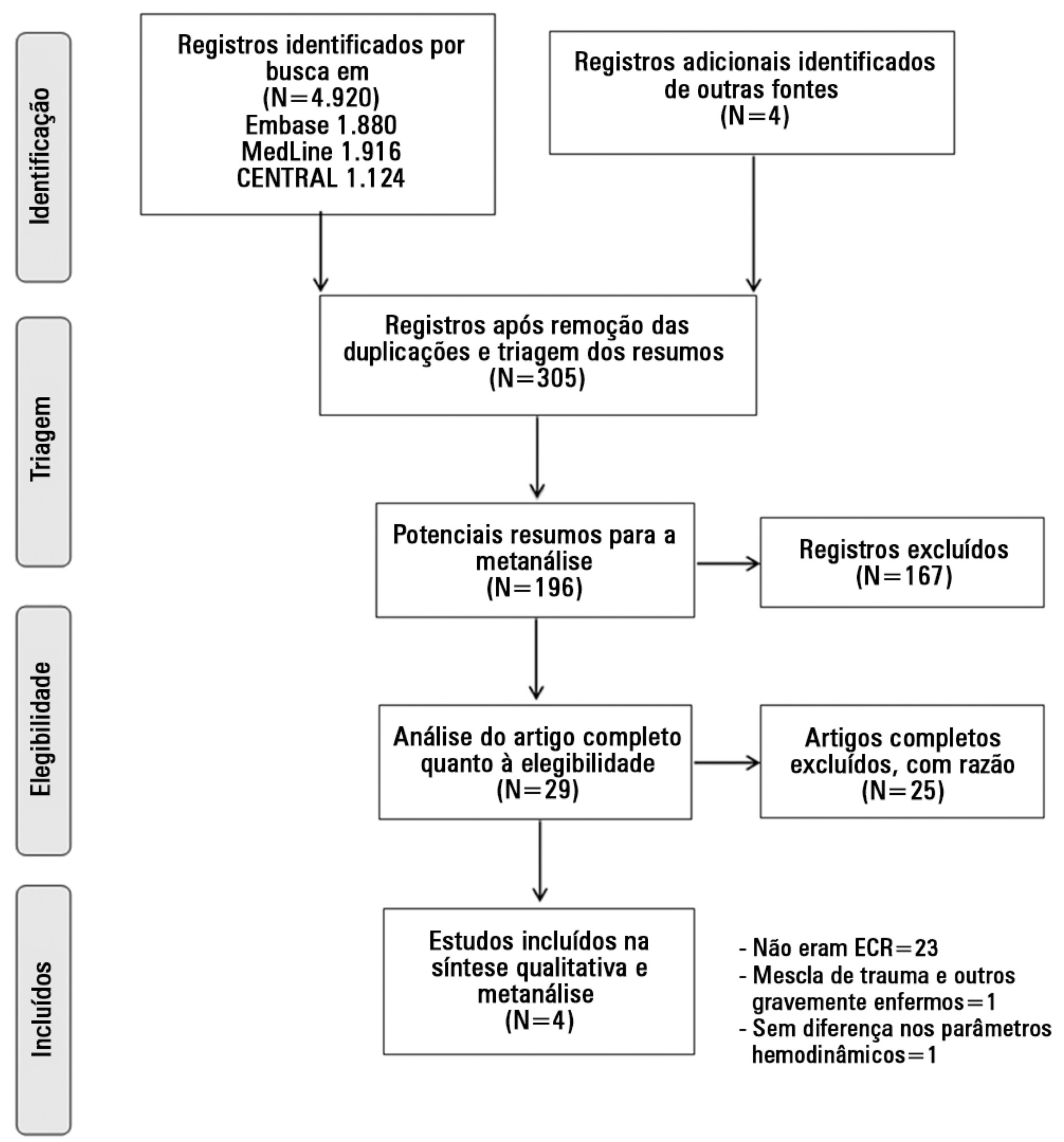
-
Special Article
Intensive care provision: a global problem
Rev Bras Ter Intensiva. 2012;24(4):322-325
Abstract
Views0Abstract
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness ICU Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis