Pulmonary Artery Catheter Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(4):474-482
DOI 10.5935/0103-507X.20190073
To compare cardiac output measurements by transthoracic echocardiography and a pulmonary artery catheter in mechanically ventilated patients with high positive end-expiratory pressure. To evaluate the effect of tricuspid regurgitation.
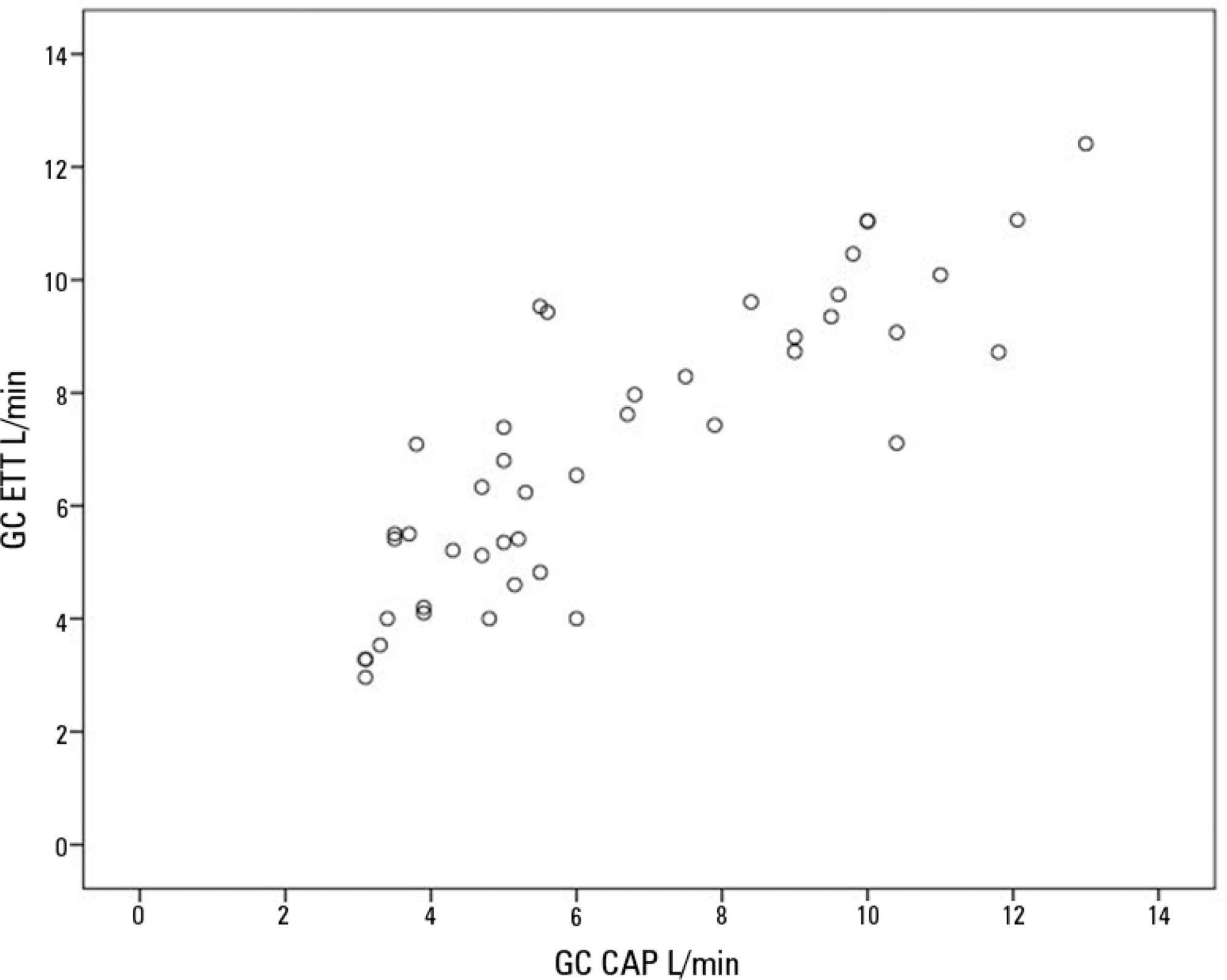
Sixteen mechanically ventilated patients were studied. Cardiac output was measured by pulmonary artery catheterization and transthoracic echocardiography. Measurements were performed at different levels of positive end-expiratory pressure (10cmH2O, 15cmH2O, and 20cmH2O). The effect of tricuspid regurgitation on cardiac output measurement was evaluated. The intraclass correlation coefficient was studied; the mean error and limits of agreement were studied with the Bland-Altman plot. The error rate was calculated.
Forty-four pairs of cardiac output measurements were obtained. An intraclass correlation coefficient of 0.908 was found (p < 0.001). The mean error was 0.44L/min for cardiac output values between 5 and 13L/min. The limits of agreement were 3.25L/min and -2.37L/min. With tricuspid insufficiency, the intraclass correlation coefficient was 0.791, and without tricuspid insufficiency, 0.935. Tricuspid insufficiency increased the error rate from 32% to 52%.
In patients with high positive end-expiratory pressure, cardiac output measurement by transthoracic echocardiography is comparable to that with a pulmonary artery catheter. Tricuspid regurgitation influences the intraclass correlation coefficient. In patients with high positive end-expiratory pressure, the use of transthoracic echocardiography to measure cardiac output is comparable to invasive measures.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):474-482
DOI 10.5935/0103-507X.20190073
To compare cardiac output measurements by transthoracic echocardiography and a pulmonary artery catheter in mechanically ventilated patients with high positive end-expiratory pressure. To evaluate the effect of tricuspid regurgitation.
Sixteen mechanically ventilated patients were studied. Cardiac output was measured by pulmonary artery catheterization and transthoracic echocardiography. Measurements were performed at different levels of positive end-expiratory pressure (10cmH2O, 15cmH2O, and 20cmH2O). The effect of tricuspid regurgitation on cardiac output measurement was evaluated. The intraclass correlation coefficient was studied; the mean error and limits of agreement were studied with the Bland-Altman plot. The error rate was calculated.
Forty-four pairs of cardiac output measurements were obtained. An intraclass correlation coefficient of 0.908 was found (p < 0.001). The mean error was 0.44L/min for cardiac output values between 5 and 13L/min. The limits of agreement were 3.25L/min and -2.37L/min. With tricuspid insufficiency, the intraclass correlation coefficient was 0.791, and without tricuspid insufficiency, 0.935. Tricuspid insufficiency increased the error rate from 32% to 52%.
In patients with high positive end-expiratory pressure, cardiac output measurement by transthoracic echocardiography is comparable to that with a pulmonary artery catheter. Tricuspid regurgitation influences the intraclass correlation coefficient. In patients with high positive end-expiratory pressure, the use of transthoracic echocardiography to measure cardiac output is comparable to invasive measures.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
BACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
BACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):137-142
DOI 10.1590/S0103-507X2006000200006
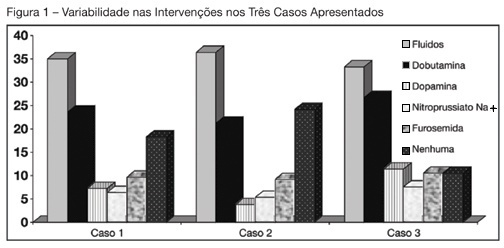
BACKGROUND AND OBJECTIVES: Use of Pulmonary Artery Catheter (PAC) is still a debatable issue, mainly due to questions raised about its security and efficacy. This study reproduced in a sample of Brazilian physicians, another one conducted amidst American doctors, in which was pointed out the heterogeneity of clinical decisions guided by data obtained from PAC. METHODS: During the Brazilian Congress of Intensive Care Medicine (Curitiba 2004), doctors were asked to answer a survey form with three vignettes. Each of them contained PAC data and one half of the surveys contained echocardiographic information. Every doctor was asked to select one of six interventions for each vignette. A homogeneous answer was considered when it was selected by at least 80% of the respondents. RESULTS: Two hundred and thirty seven doctors answered the questionnaires. They selected completely different therapeutic interventions in all three vignettes and none of the interventions achieved more than 80% agreement. Variability persisted with the choices guided by echocardiography. CONCLUSIONS: As in the original study, we observed total heterogeneity of therapeutic interventions guided by CAP and echocardiography. These results could be caused by lack of knowledge about basic pathophysiologic concepts and maybe we had to improve its teaching at the medical school benches.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):137-142
DOI 10.1590/S0103-507X2006000200006
BACKGROUND AND OBJECTIVES: Use of Pulmonary Artery Catheter (PAC) is still a debatable issue, mainly due to questions raised about its security and efficacy. This study reproduced in a sample of Brazilian physicians, another one conducted amidst American doctors, in which was pointed out the heterogeneity of clinical decisions guided by data obtained from PAC. METHODS: During the Brazilian Congress of Intensive Care Medicine (Curitiba 2004), doctors were asked to answer a survey form with three vignettes. Each of them contained PAC data and one half of the surveys contained echocardiographic information. Every doctor was asked to select one of six interventions for each vignette. A homogeneous answer was considered when it was selected by at least 80% of the respondents. RESULTS: Two hundred and thirty seven doctors answered the questionnaires. They selected completely different therapeutic interventions in all three vignettes and none of the interventions achieved more than 80% agreement. Variability persisted with the choices guided by echocardiography. CONCLUSIONS: As in the original study, we observed total heterogeneity of therapeutic interventions guided by CAP and echocardiography. These results could be caused by lack of knowledge about basic pathophysiologic concepts and maybe we had to improve its teaching at the medical school benches.