morbidity Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2009;21(4):353-358
DOI 10.1590/S0103-507X2009000400004
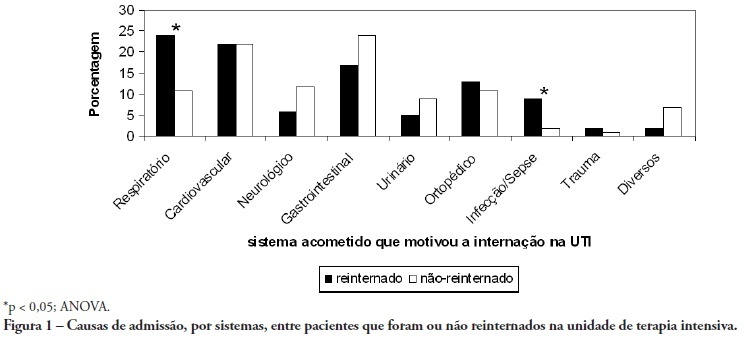
OBJECTIVE: To predict readmission in intensive care unit analyzing the first 24 hours data after intensive care unit admission. METHODS: The first intensive care unit admission of patients was analyzed from January to May 2009 in a mixed unit. Readmission to the unit was considered those during the same hospital stay or within 3 months after intensive care unit discharge. Deaths during the first admission were excluded. Demographic data, use of mechanical ventilation, and report of stay longer than 3 days were submitted to uni and multivariate analysis for readmission. RESULTS: Five hundred seventy-seven patients were included (33 excluded deaths). The readmission group had 59 patients, while 518 patients were not readmitted. The lead time between the index admission and readmission was 9 (3-28) days (18 were readmitted in less than 3 days), and 10 died. Patients readmitted at least once to the intensive care unit had the differences below in comparison to the control group: older age: 75 (67-81) versus 67 (56-78) years, P<0.01; admission for respiratory insufficiency or sepsis: 33 versus 13%, P<0.01; medical admission: 49 versus 32%, P<0.05; higher SAPS II score: 27 (21-35) versus 23 (18-29) points, P<0.01; Charlson index: 2 (1-2) versus 1 (0-2) points, P<0.01; first ICU stay longer than 3 days: 35 versus 23%, P<0.01. After logistic regression, higher age, Charlson index and admission for respiratory and sepsis were independently associated to readmissions in intensive care unit. CONCLUSION: Age, comorbidities and respiratory- and/or sepsis-related admission are associated with increased readmission risk in the studied sample.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):353-358
DOI 10.1590/S0103-507X2009000400004
OBJECTIVE: To predict readmission in intensive care unit analyzing the first 24 hours data after intensive care unit admission. METHODS: The first intensive care unit admission of patients was analyzed from January to May 2009 in a mixed unit. Readmission to the unit was considered those during the same hospital stay or within 3 months after intensive care unit discharge. Deaths during the first admission were excluded. Demographic data, use of mechanical ventilation, and report of stay longer than 3 days were submitted to uni and multivariate analysis for readmission. RESULTS: Five hundred seventy-seven patients were included (33 excluded deaths). The readmission group had 59 patients, while 518 patients were not readmitted. The lead time between the index admission and readmission was 9 (3-28) days (18 were readmitted in less than 3 days), and 10 died. Patients readmitted at least once to the intensive care unit had the differences below in comparison to the control group: older age: 75 (67-81) versus 67 (56-78) years, P<0.01; admission for respiratory insufficiency or sepsis: 33 versus 13%, P<0.01; medical admission: 49 versus 32%, P<0.05; higher SAPS II score: 27 (21-35) versus 23 (18-29) points, P<0.01; Charlson index: 2 (1-2) versus 1 (0-2) points, P<0.01; first ICU stay longer than 3 days: 35 versus 23%, P<0.01. After logistic regression, higher age, Charlson index and admission for respiratory and sepsis were independently associated to readmissions in intensive care unit. CONCLUSION: Age, comorbidities and respiratory- and/or sepsis-related admission are associated with increased readmission risk in the studied sample.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):360-365
DOI 10.1590/S0103-507X2006000400007
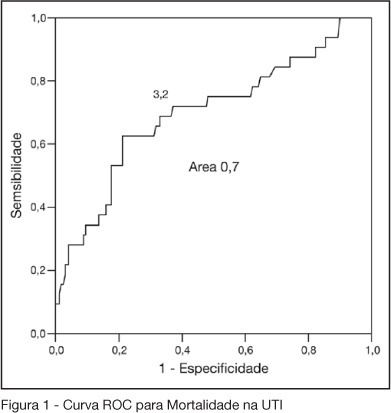
BACKGROUND AND OBJECTIVES: One of the greatest challenges found by the intensivists in their daily activities is tissue hipoperfusion control. Blood lactate is generally accepted as a marker of tissular hypoxia and several studies have demonstrated good correlation between blood lactate and prognosis during shock and resuscitation. The aim of this study was to evaluate the clinical utility of arterial blood lactate as a marker of morbidity and mortality in critically ill patients in the post-operative period of high risk non-cardiac surgeries. METHODS: Prospective and observational cohort study realized in an ICU of a tertiary hospital during a four month period. Demographic data of the patients submitted to high risk surgeries were collected, besides arterial lactate measures and number and type of complications in the post-operative period. To the statistic analysis was considered as significant a p < 0.05. The predictive ability of the indexes to differentiate survivors from non-survivors was tested using ROC curves. Lenght of ICU stay estimation where calculated by Kaplan Meier method. RESULTS: Were included 202 patients. 50.2% were female and their mean age was 66.5 ± 13.6 years. APACHE II score was 17.4 ± 3.0 and the median of MODS score was 4 (2-6). Median lenght of surgeries was 4h (3-6h). 70.7% of the surgeries were elective ones. ICU and hospital mortality were 15.6% and 33.7%, respectively. The best lactate value to discriminate mortality was 3.2 mmol/L, with sensitivity of 62.5%, specificity of 78.8% and an area under the curve of 0.7. 62.5% of patients with lactate > 3.2 did not survive versus 21.2% of survivors (OR = 2.95 IC95% 1.98- 4.38, p < 0.0001). ICU lenght of stay was greater when > 3.2 mmol/L (log rank 0.007) lactate. CONCLUSIONS: High risk patients submitted to non cardiac surgeries and admitted to the ICU with hiperlactatemia, defined as an arterial lactate > 3.2 mmol/L, are prone to a longer ICU lenght of stay and to die.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):360-365
DOI 10.1590/S0103-507X2006000400007
BACKGROUND AND OBJECTIVES: One of the greatest challenges found by the intensivists in their daily activities is tissue hipoperfusion control. Blood lactate is generally accepted as a marker of tissular hypoxia and several studies have demonstrated good correlation between blood lactate and prognosis during shock and resuscitation. The aim of this study was to evaluate the clinical utility of arterial blood lactate as a marker of morbidity and mortality in critically ill patients in the post-operative period of high risk non-cardiac surgeries. METHODS: Prospective and observational cohort study realized in an ICU of a tertiary hospital during a four month period. Demographic data of the patients submitted to high risk surgeries were collected, besides arterial lactate measures and number and type of complications in the post-operative period. To the statistic analysis was considered as significant a p < 0.05. The predictive ability of the indexes to differentiate survivors from non-survivors was tested using ROC curves. Lenght of ICU stay estimation where calculated by Kaplan Meier method. RESULTS: Were included 202 patients. 50.2% were female and their mean age was 66.5 ± 13.6 years. APACHE II score was 17.4 ± 3.0 and the median of MODS score was 4 (2-6). Median lenght of surgeries was 4h (3-6h). 70.7% of the surgeries were elective ones. ICU and hospital mortality were 15.6% and 33.7%, respectively. The best lactate value to discriminate mortality was 3.2 mmol/L, with sensitivity of 62.5%, specificity of 78.8% and an area under the curve of 0.7. 62.5% of patients with lactate > 3.2 did not survive versus 21.2% of survivors (OR = 2.95 IC95% 1.98- 4.38, p < 0.0001). ICU lenght of stay was greater when > 3.2 mmol/L (log rank 0.007) lactate. CONCLUSIONS: High risk patients submitted to non cardiac surgeries and admitted to the ICU with hiperlactatemia, defined as an arterial lactate > 3.2 mmol/L, are prone to a longer ICU lenght of stay and to die.
Abstract
Rev Bras Ter Intensiva. 2007;19(1):5-13
DOI 10.1590/S0103-507X2007000100001
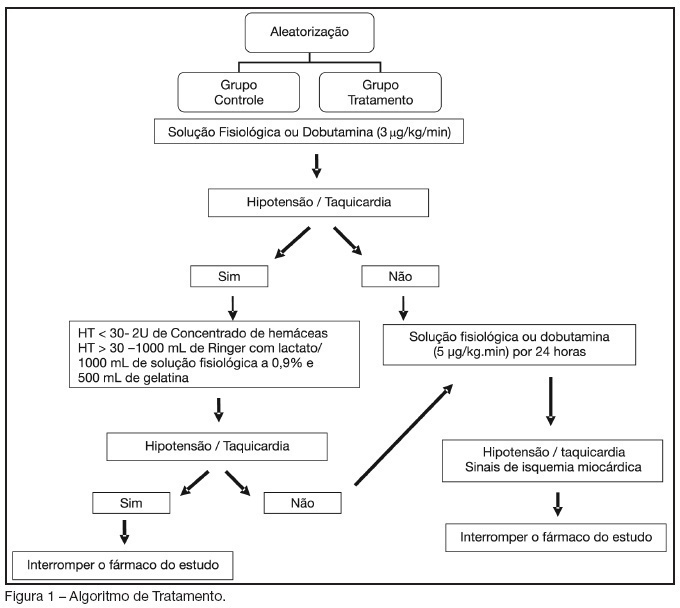
BACKGROUND AND OBJECTIVES: Dobutamine is an inotropic agent with predominant beta1- adrenergic properties frequently used to increase blood flow in critically ill patients. Dobutamine may have a role in increasing splanchnic perfusion, thereby protecting this area from further injury. We investigated the effects of low doses dobutamine (5 mug/kg/min) on tissue oxygenation, inflammatory response and postoperative complications in high-risk surgical patients. METHODS: Prospective, randomized, blinded and placebo-controlled study. One hundred surgical patients admitted in a step-down unit were evaluated and 82 patients were enrolled, 42 in the control group (saline) and 40 in the treatment group (5 mug/kg/h) during 24 hours. Similar therapeutic goals were applied to both groups. Fluids were given whenever tachycardia or hypotension developed after study drug infusion. RESULTS: The total volume of fluids given was significantly higher in treatment than in control group (7351 ± 2082 mL versus 6074 ± 2386 mL, respectively, p < 0.05). Central venous oxygen saturation (ScvO2), serum lactate and C-reactive protein were similar in both groups. Complications occurred in 35% and 50% of the patients in the treatment and control groups, respectively (RR 0, 70 IC 95% 0.41 - 1.17; NS). CONCLUSIONS: Low-doses dobutamine and fluids after surgical trauma has no effects on the prevalence of postoperative complications in high-risk surgical patients.
Abstract
Rev Bras Ter Intensiva. 2007;19(1):5-13
DOI 10.1590/S0103-507X2007000100001
BACKGROUND AND OBJECTIVES: Dobutamine is an inotropic agent with predominant beta1- adrenergic properties frequently used to increase blood flow in critically ill patients. Dobutamine may have a role in increasing splanchnic perfusion, thereby protecting this area from further injury. We investigated the effects of low doses dobutamine (5 mug/kg/min) on tissue oxygenation, inflammatory response and postoperative complications in high-risk surgical patients. METHODS: Prospective, randomized, blinded and placebo-controlled study. One hundred surgical patients admitted in a step-down unit were evaluated and 82 patients were enrolled, 42 in the control group (saline) and 40 in the treatment group (5 mug/kg/h) during 24 hours. Similar therapeutic goals were applied to both groups. Fluids were given whenever tachycardia or hypotension developed after study drug infusion. RESULTS: The total volume of fluids given was significantly higher in treatment than in control group (7351 ± 2082 mL versus 6074 ± 2386 mL, respectively, p < 0.05). Central venous oxygen saturation (ScvO2), serum lactate and C-reactive protein were similar in both groups. Complications occurred in 35% and 50% of the patients in the treatment and control groups, respectively (RR 0, 70 IC 95% 0.41 - 1.17; NS). CONCLUSIONS: Low-doses dobutamine and fluids after surgical trauma has no effects on the prevalence of postoperative complications in high-risk surgical patients.