mechanical ventilation Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2007;19(3):393-398
DOI 10.1590/S0103-507X2007000300022
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based Medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Intraoperative mechanical ventilation has been one of the updated topics. This objective was described the most important topics on the intraoperative mechanical ventilation. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words: mechanical ventilation, intraoperative and anesthesia. RESULTS: Recommendations on how to prevent pulmonary complications during anesthesia/postoperative period and which are the best intraoperative ventilatory techniques. CONCLUSIONS: Pulmonary atelectasis is a common complication observed in the postoperative period, thus ventilatory techniques has been adapted to prevent these complications.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):393-398
DOI 10.1590/S0103-507X2007000300022
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based Medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Intraoperative mechanical ventilation has been one of the updated topics. This objective was described the most important topics on the intraoperative mechanical ventilation. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words: mechanical ventilation, intraoperative and anesthesia. RESULTS: Recommendations on how to prevent pulmonary complications during anesthesia/postoperative period and which are the best intraoperative ventilatory techniques. CONCLUSIONS: Pulmonary atelectasis is a common complication observed in the postoperative period, thus ventilatory techniques has been adapted to prevent these complications.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):284-291
DOI 10.1590/S0103-507X2007000300003
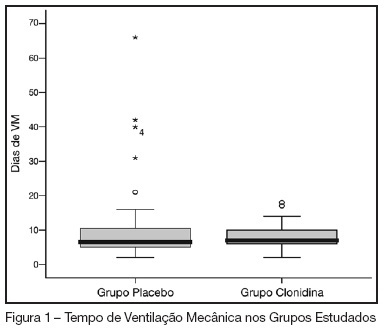
BACKGROUND AND OBJECTIVES: In our country, the abstinence syndrome has high prevalence and besides the distress prolongs the length of hospital stay. The aim of this study was to evaluate the influence of associating oral clonidine to the intravenous morphine plus midazolam continuous infusion in children submitted to mechanical ventilation. METHODS: Randomized, double blind, placebo controlled study, conducted in the PICU at the Hospital Geral of Caxias do Sul. All children (1-36 months) submitted to mechanical ventilation over 12 hours (May-2005/August-2006), which had used intravenous morphine and midazolam continuous infusion were included. They were randomized to received clonidine (5 µg/kg) or placebo associated to the sedative continuous infusion. The infusion sedative doses were at the discretion of the assistant physician. The administered doses in the previous 24 hours and the doses of intermittent sedation were daily collected. The abstinence syndrome was defined based on Finnegan Score. The groups were compared regarding the cumulative doses of sedatives, length of use of sedative continuous infusion, presence and duration of the abstinence. RESULTS: Were included 69 patients (31 in the clonidine group and 38 in the placebo group). The two groups were similar regarding the general characteristics (weight, age, gender, indication of mechanical ventilation). The midazolam and morphine doses (cumulative and intermittent doses) were not different in both groups. Completed the study 59 patients, 25 in clonidine group and 34 in placebo group. The prevalence of the abstinence was similar (72% and 75%, respectively), without difference in the recovery time neither related to the length of mechanical ventilation. CONCLUSIONS: In children submitted to mechanical ventilation using high dose of opioids and diazepinic infusion the addiction of clonidine did not decrease the daily doses neither the cumulative doses and nevertheless reduced the prevalence and the evolution of abstinence syndrome.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):284-291
DOI 10.1590/S0103-507X2007000300003
BACKGROUND AND OBJECTIVES: In our country, the abstinence syndrome has high prevalence and besides the distress prolongs the length of hospital stay. The aim of this study was to evaluate the influence of associating oral clonidine to the intravenous morphine plus midazolam continuous infusion in children submitted to mechanical ventilation. METHODS: Randomized, double blind, placebo controlled study, conducted in the PICU at the Hospital Geral of Caxias do Sul. All children (1-36 months) submitted to mechanical ventilation over 12 hours (May-2005/August-2006), which had used intravenous morphine and midazolam continuous infusion were included. They were randomized to received clonidine (5 µg/kg) or placebo associated to the sedative continuous infusion. The infusion sedative doses were at the discretion of the assistant physician. The administered doses in the previous 24 hours and the doses of intermittent sedation were daily collected. The abstinence syndrome was defined based on Finnegan Score. The groups were compared regarding the cumulative doses of sedatives, length of use of sedative continuous infusion, presence and duration of the abstinence. RESULTS: Were included 69 patients (31 in the clonidine group and 38 in the placebo group). The two groups were similar regarding the general characteristics (weight, age, gender, indication of mechanical ventilation). The midazolam and morphine doses (cumulative and intermittent doses) were not different in both groups. Completed the study 59 patients, 25 in clonidine group and 34 in placebo group. The prevalence of the abstinence was similar (72% and 75%, respectively), without difference in the recovery time neither related to the length of mechanical ventilation. CONCLUSIONS: In children submitted to mechanical ventilation using high dose of opioids and diazepinic infusion the addiction of clonidine did not decrease the daily doses neither the cumulative doses and nevertheless reduced the prevalence and the evolution of abstinence syndrome.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):331-336
DOI 10.1590/S0103-507X2007000300011
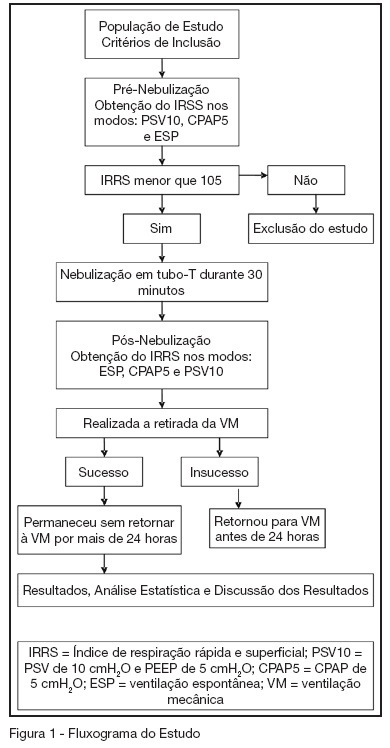
BACKGROUND AND OBJECTIVES: To compare the attainment of the rapid shallow breathing index (IRRS) in modalities PSV 10 cmH2O and PEEP 5 cmH2O (PSV10), CPAP 5 cmH2O (CPAP5) and spontaneous breathing (SB), correlating them with success on failure in the withdrawal of mechanical ventilation (MV). METHODS: Prospective study including 54 patients in MV > 48 hours, submitted to the IRRS in three ventilatory modalities: PSV10, CPAP5 and SB at the moments before and after T-tube spontaneous breathing. The patients were removed from MV when IRRS was < 105. RESULTS: There wasn't statistically significant difference between IRRS values at the moments before and after T-tube SB. There was statistically significant difference IRRS value between the modalities CPAP5 and PSV10 (p = 0.008), and between the modalities SB and PSV10 (p = 0.01) at the moment before T-Tube SB and of IRRS value, gotten between CPAP5 and PSV10 (p = 0.01) at the moment after T-tube SB. CONCLUSIONS: From this sample, it can be observed that IRRS values are overestimated when gotten in modality PSV10. It was also evidenced that there is no need of a 30 min T-tube SB before extubation, when the weaning is performed with the technique of gradual reduction of PSV. This study suggested that IRRS is able to predict weaning success; however it is not able to determine failure when it was < 105. It is recommended that IRRS must be analyzed in association with other predictive weaning parameters.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):331-336
DOI 10.1590/S0103-507X2007000300011
BACKGROUND AND OBJECTIVES: To compare the attainment of the rapid shallow breathing index (IRRS) in modalities PSV 10 cmH2O and PEEP 5 cmH2O (PSV10), CPAP 5 cmH2O (CPAP5) and spontaneous breathing (SB), correlating them with success on failure in the withdrawal of mechanical ventilation (MV). METHODS: Prospective study including 54 patients in MV > 48 hours, submitted to the IRRS in three ventilatory modalities: PSV10, CPAP5 and SB at the moments before and after T-tube spontaneous breathing. The patients were removed from MV when IRRS was < 105. RESULTS: There wasn't statistically significant difference between IRRS values at the moments before and after T-tube SB. There was statistically significant difference IRRS value between the modalities CPAP5 and PSV10 (p = 0.008), and between the modalities SB and PSV10 (p = 0.01) at the moment before T-Tube SB and of IRRS value, gotten between CPAP5 and PSV10 (p = 0.01) at the moment after T-tube SB. CONCLUSIONS: From this sample, it can be observed that IRRS values are overestimated when gotten in modality PSV10. It was also evidenced that there is no need of a 30 min T-tube SB before extubation, when the weaning is performed with the technique of gradual reduction of PSV. This study suggested that IRRS is able to predict weaning success; however it is not able to determine failure when it was < 105. It is recommended that IRRS must be analyzed in association with other predictive weaning parameters.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):374-383
DOI 10.1590/S0103-507X2007000300020
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Acute Respiratory Distress Syndrome (ARDS) has been one of the updated topics. This objective was described the most important topics related to mechanical ventilation in patients with acute respiratory distress syndrome. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words mechanical ventilation and acute respiratory distress syndrome. RESULTS: Recommendations on the use of lung protective strategies during mechanical ventilation based on reduced tidal volumes and limitation of plateau pressure. The state of the art of recruitment maneuvers and PEEP titration is also discussed. CONCLUSIONS: The mechanical ventilation of patients with ADRS changed in the last few years. We presented the role of lung protective strategies that could be applied to these patients.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):374-383
DOI 10.1590/S0103-507X2007000300020
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Acute Respiratory Distress Syndrome (ARDS) has been one of the updated topics. This objective was described the most important topics related to mechanical ventilation in patients with acute respiratory distress syndrome. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words mechanical ventilation and acute respiratory distress syndrome. RESULTS: Recommendations on the use of lung protective strategies during mechanical ventilation based on reduced tidal volumes and limitation of plateau pressure. The state of the art of recruitment maneuvers and PEEP titration is also discussed. CONCLUSIONS: The mechanical ventilation of patients with ADRS changed in the last few years. We presented the role of lung protective strategies that could be applied to these patients.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):384-392
DOI 10.1590/S0103-507X2007000300021
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Weaning from mechanical ventilation has been one of the updated topics. This objective was described the most important topics related to weaning from mechanical ventilation. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the keywords weaning and mechanical ventilation. RESULTS: Recommendations on the weaning from mechanical ventilation and how to select patients applying weaning protocols and spontaneous breathing test. CONCLUSIONS: Weaning is a very important period of mechanical ventilatory support. Weaning protocols are recommended to select patients ready to be extubated.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):384-392
DOI 10.1590/S0103-507X2007000300021
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Weaning from mechanical ventilation has been one of the updated topics. This objective was described the most important topics related to weaning from mechanical ventilation. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the keywords weaning and mechanical ventilation. RESULTS: Recommendations on the weaning from mechanical ventilation and how to select patients applying weaning protocols and spontaneous breathing test. CONCLUSIONS: Weaning is a very important period of mechanical ventilatory support. Weaning protocols are recommended to select patients ready to be extubated.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):170-175
DOI 10.1590/S0103-507X2007000200005
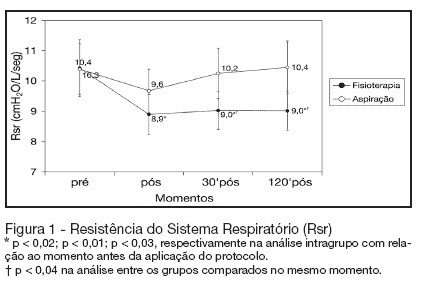
BACKGROUND AND OBJECTIVES: The chest physiotherapy (CP) in patients submitted to invasive support ventilation acts directly in the breathing system, and it could alter the lung mechanics through the dynamic lung compliance (DynC) and resistance of the breathing system (Rbs). However the alterations after the accomplishment of CP are still controversy. The objective of this study was to evaluate the alterations of the lung mechanics in patients in invasive mechanical ventilation (IMV). METHODS: It was a prospective, randomized, and controlled and crossover study, with patient with more than 48 hours in IMV. The protocol of chest physiotherapy and isolated tracheal aspiration they were randomized for the application order with a window of 24 hours among them. Data of lung mechanics and its varied cardiorespiratory were collected moments before the protocol, immediately after the application of the protocol, 30 minutes and 120 minutes after the application of the protocols. RESULTS: Twelve patients completed the study. Pneumonia was the mean cause respiratory failure (RF). There was not statistical difference among the groups in relation to Cdyn, volume tidal (Vt) and volume minute (Ve). Rbs decreased in a significant way immediately after (of 10.4 ± 3 cmH2O/L/seg for 8.9 ± 2 cmH2O/L/seg; p < 0.02), 30 minutes after (of 10.4 ± 3 cmH2O/L/seg for 9 ± 2 cmH2O/L/seg; p < 0.01) and 120 minutes after (of 10.4 ± 3 cmH2O/L/seg for 9 ± 2 cmH2O/L/seg; p < 0.03) application the protocol of chest physiotherapy. When compared with the protocol of isolated tracheal aspiration it was significantly smaller in the 30 (9 ± 2 cmH2O/L/seg versus10.2 ± 2 cmH2O/L/seg; p < 0.04) and 120 minutes (9 ± 2 cmH2O/L/seg versus 10.4 ± 3 cmH2O/L/seg; p < 0.04). CONCLUSIONS: The protocol of chest physiotherapy was effective in the decrease of Rsr when compared with the aspiration protocol. That decrease was maintained for two hours after its application, what did not happen when only the just accomplished the tracheal aspiration was performed isolated.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):170-175
DOI 10.1590/S0103-507X2007000200005
BACKGROUND AND OBJECTIVES: The chest physiotherapy (CP) in patients submitted to invasive support ventilation acts directly in the breathing system, and it could alter the lung mechanics through the dynamic lung compliance (DynC) and resistance of the breathing system (Rbs). However the alterations after the accomplishment of CP are still controversy. The objective of this study was to evaluate the alterations of the lung mechanics in patients in invasive mechanical ventilation (IMV). METHODS: It was a prospective, randomized, and controlled and crossover study, with patient with more than 48 hours in IMV. The protocol of chest physiotherapy and isolated tracheal aspiration they were randomized for the application order with a window of 24 hours among them. Data of lung mechanics and its varied cardiorespiratory were collected moments before the protocol, immediately after the application of the protocol, 30 minutes and 120 minutes after the application of the protocols. RESULTS: Twelve patients completed the study. Pneumonia was the mean cause respiratory failure (RF). There was not statistical difference among the groups in relation to Cdyn, volume tidal (Vt) and volume minute (Ve). Rbs decreased in a significant way immediately after (of 10.4 ± 3 cmH2O/L/seg for 8.9 ± 2 cmH2O/L/seg; p < 0.02), 30 minutes after (of 10.4 ± 3 cmH2O/L/seg for 9 ± 2 cmH2O/L/seg; p < 0.01) and 120 minutes after (of 10.4 ± 3 cmH2O/L/seg for 9 ± 2 cmH2O/L/seg; p < 0.03) application the protocol of chest physiotherapy. When compared with the protocol of isolated tracheal aspiration it was significantly smaller in the 30 (9 ± 2 cmH2O/L/seg versus10.2 ± 2 cmH2O/L/seg; p < 0.04) and 120 minutes (9 ± 2 cmH2O/L/seg versus 10.4 ± 3 cmH2O/L/seg; p < 0.04). CONCLUSIONS: The protocol of chest physiotherapy was effective in the decrease of Rsr when compared with the aspiration protocol. That decrease was maintained for two hours after its application, what did not happen when only the just accomplished the tracheal aspiration was performed isolated.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):264-272
DOI 10.1590/S0103-507X2007000200021
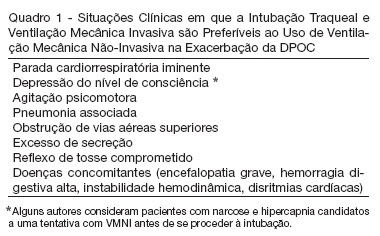
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Mechanical ventilation in COPD exacerbation has been one of the updated topics. Describe the most important topics on the mechanical ventilation during the COPD exacerbation and suggest the main therapeutic approaches. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the keywords "mechanical ventilation" and "COPD". RESULTS: We present recommendations on the ventilatory modes and settings to be adopted when ventilating a patient during an asthma attack, as well as the recommended monitoring. Alternative ventilation techniques are also presented. CONCLUSIONS: Protective ventilatory strategies are recommended when ventilating a patient during a.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):264-272
DOI 10.1590/S0103-507X2007000200021
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Mechanical ventilation in COPD exacerbation has been one of the updated topics. Describe the most important topics on the mechanical ventilation during the COPD exacerbation and suggest the main therapeutic approaches. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the keywords "mechanical ventilation" and "COPD". RESULTS: We present recommendations on the ventilatory modes and settings to be adopted when ventilating a patient during an asthma attack, as well as the recommended monitoring. Alternative ventilation techniques are also presented. CONCLUSIONS: Protective ventilatory strategies are recommended when ventilating a patient during a.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):176-181
DOI 10.1590/S0103-507X2007000200006
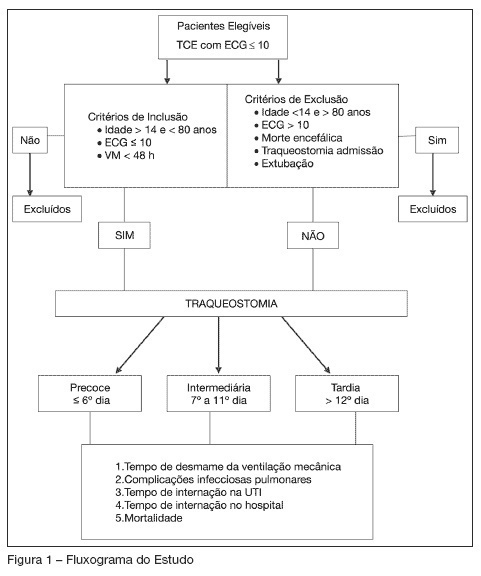
BACKGROUND AND OBJECTIVES: Actually, It’s doubtful if early tracheostomy (ET) can influence mechanical ventilation (MV) weaning time or the hospital length of stay in patients with traumatic brain injury (TBI). The main objective of this trial was to verify the influence of ET on weaning time of patients with severe TBI. METHODS: Prospective, observational study, including 33 patients with severe TBI (GCS < 10 at hospital admission), evaluated according to tracheostomy performance time (early: t < 6 days; intermediate: t = 7 to 11 days; and late: t > 12 days) and the weaning from MV. RESULTS: Total ventilation mechanical time has been reduced in the early tracheostomy group (n = 10; p < 0.0001). A lower GCS punctuation (mean 5.3 ± 2.5) in ET group has been negatively correlated with hospital length of stay (LOS) (p = 0.02). CONCLUSIONS: Early tracheostomy can decrease mechanical ventilation time, but does not influence hospital LOS in patients with severe traumatic brain injury.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):176-181
DOI 10.1590/S0103-507X2007000200006
BACKGROUND AND OBJECTIVES: Actually, It’s doubtful if early tracheostomy (ET) can influence mechanical ventilation (MV) weaning time or the hospital length of stay in patients with traumatic brain injury (TBI). The main objective of this trial was to verify the influence of ET on weaning time of patients with severe TBI. METHODS: Prospective, observational study, including 33 patients with severe TBI (GCS < 10 at hospital admission), evaluated according to tracheostomy performance time (early: t < 6 days; intermediate: t = 7 to 11 days; and late: t > 12 days) and the weaning from MV. RESULTS: Total ventilation mechanical time has been reduced in the early tracheostomy group (n = 10; p < 0.0001). A lower GCS punctuation (mean 5.3 ± 2.5) in ET group has been negatively correlated with hospital length of stay (LOS) (p = 0.02). CONCLUSIONS: Early tracheostomy can decrease mechanical ventilation time, but does not influence hospital LOS in patients with severe traumatic brain injury.