Critical care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(2):219-230
DOI 10.5935/0103-507X.20210029
To assess the impact of intensive care unit bed availability, distractors and choice framing on intensive care unit admission decisions.
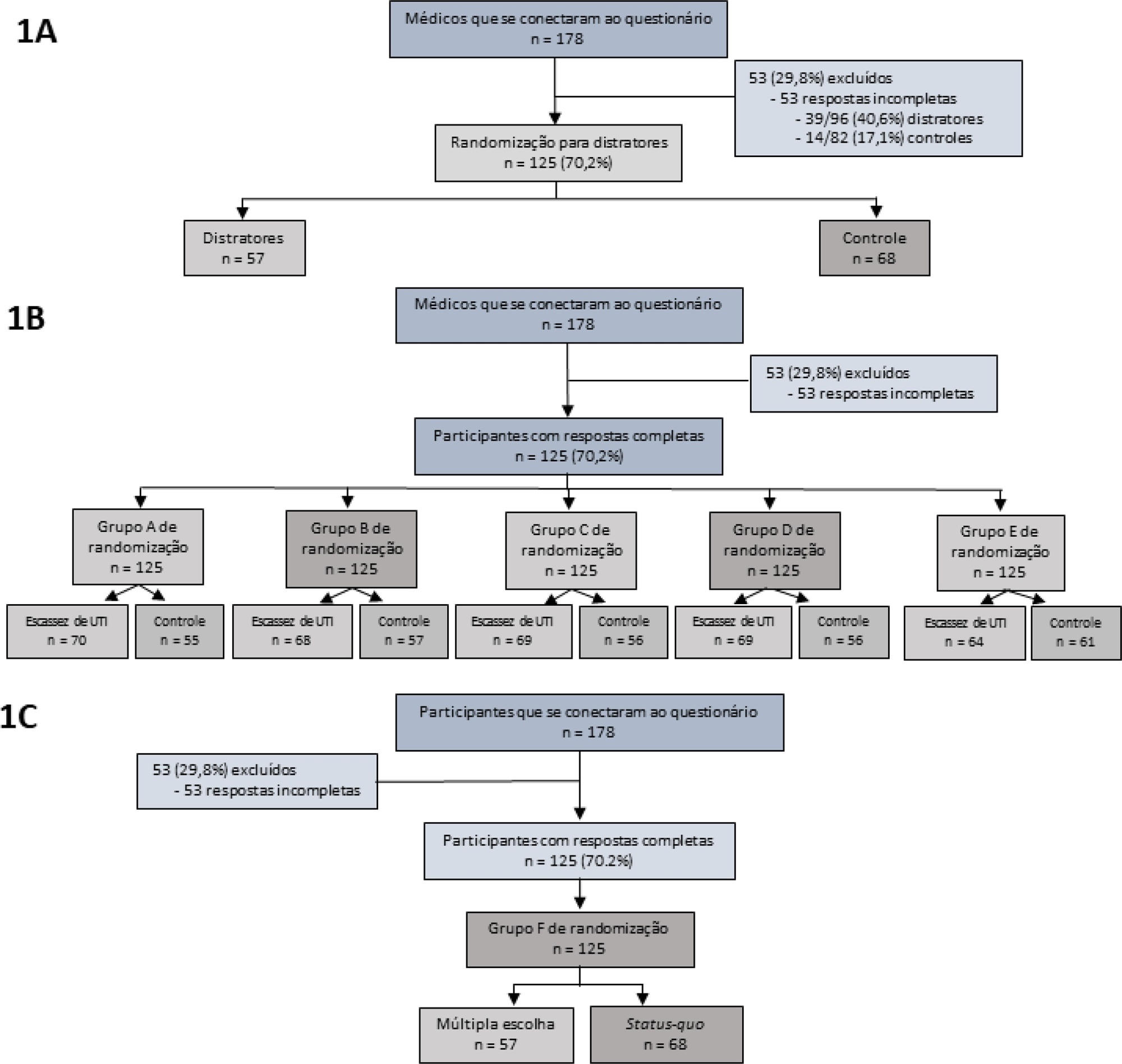
This study was a randomized factorial trial using patient-based vignettes. The vignettes were deemed archetypical for intensive care unit admission or refusal, as judged by a group of experts. Intensive care unit physicians were randomized to 1) an increased distraction (intervention) or a control group, 2) an intensive care unit bed scarcity or nonscarcity (availability) setting, and 3) a multiple-choice or omission (status quo) vignette scenario. The primary outcome was the proportion of appropriate intensive care unit allocations, defined as concordance with the allocation decision made by the group of experts.
We analyzed 125 physicians. Overall, distractors had no impact on the outcome; however, there was a differential drop-out rate, with fewer physicians in the intervention arm completing the questionnaire. Intensive care unit bed availability was associated with an inappropriate allocation of vignettes deemed inappropriate for intensive care unit admission (OR = 2.47; 95%CI 1.19 - 5.11) but not of vignettes appropriate for intensive care unit admission. There was a significant interaction with the presence of distractors (p = 0.007), with intensive care unit bed availability being associated with increased intensive care unit admission of vignettes inappropriate for intensive care unit admission in the distractor (intervention) arm (OR = 9.82; 95%CI 2.68 - 25.93) but not in the control group (OR = 1.02; 95%CI 0.38 - 2.72). Multiple choices were associated with increased inappropriate allocation in comparison to the omission group (OR = 5.18; 95%CI 1.37 - 19.61).
Intensive care unit bed availability and cognitive biases were associated with inappropriate intensive care unit allocation decisions. These findings may have implications for intensive care unit admission policies.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):219-230
DOI 10.5935/0103-507X.20210029
To assess the impact of intensive care unit bed availability, distractors and choice framing on intensive care unit admission decisions.
This study was a randomized factorial trial using patient-based vignettes. The vignettes were deemed archetypical for intensive care unit admission or refusal, as judged by a group of experts. Intensive care unit physicians were randomized to 1) an increased distraction (intervention) or a control group, 2) an intensive care unit bed scarcity or nonscarcity (availability) setting, and 3) a multiple-choice or omission (status quo) vignette scenario. The primary outcome was the proportion of appropriate intensive care unit allocations, defined as concordance with the allocation decision made by the group of experts.
We analyzed 125 physicians. Overall, distractors had no impact on the outcome; however, there was a differential drop-out rate, with fewer physicians in the intervention arm completing the questionnaire. Intensive care unit bed availability was associated with an inappropriate allocation of vignettes deemed inappropriate for intensive care unit admission (OR = 2.47; 95%CI 1.19 - 5.11) but not of vignettes appropriate for intensive care unit admission. There was a significant interaction with the presence of distractors (p = 0.007), with intensive care unit bed availability being associated with increased intensive care unit admission of vignettes inappropriate for intensive care unit admission in the distractor (intervention) arm (OR = 9.82; 95%CI 2.68 - 25.93) but not in the control group (OR = 1.02; 95%CI 0.38 - 2.72). Multiple choices were associated with increased inappropriate allocation in comparison to the omission group (OR = 5.18; 95%CI 1.37 - 19.61).
Intensive care unit bed availability and cognitive biases were associated with inappropriate intensive care unit allocation decisions. These findings may have implications for intensive care unit admission policies.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):243-250
DOI 10.5935/0103-507X.20210031
To relate functional independence to the degree of pulmonary impairment in adult patients 3 months after discharge from the intensive care unit.
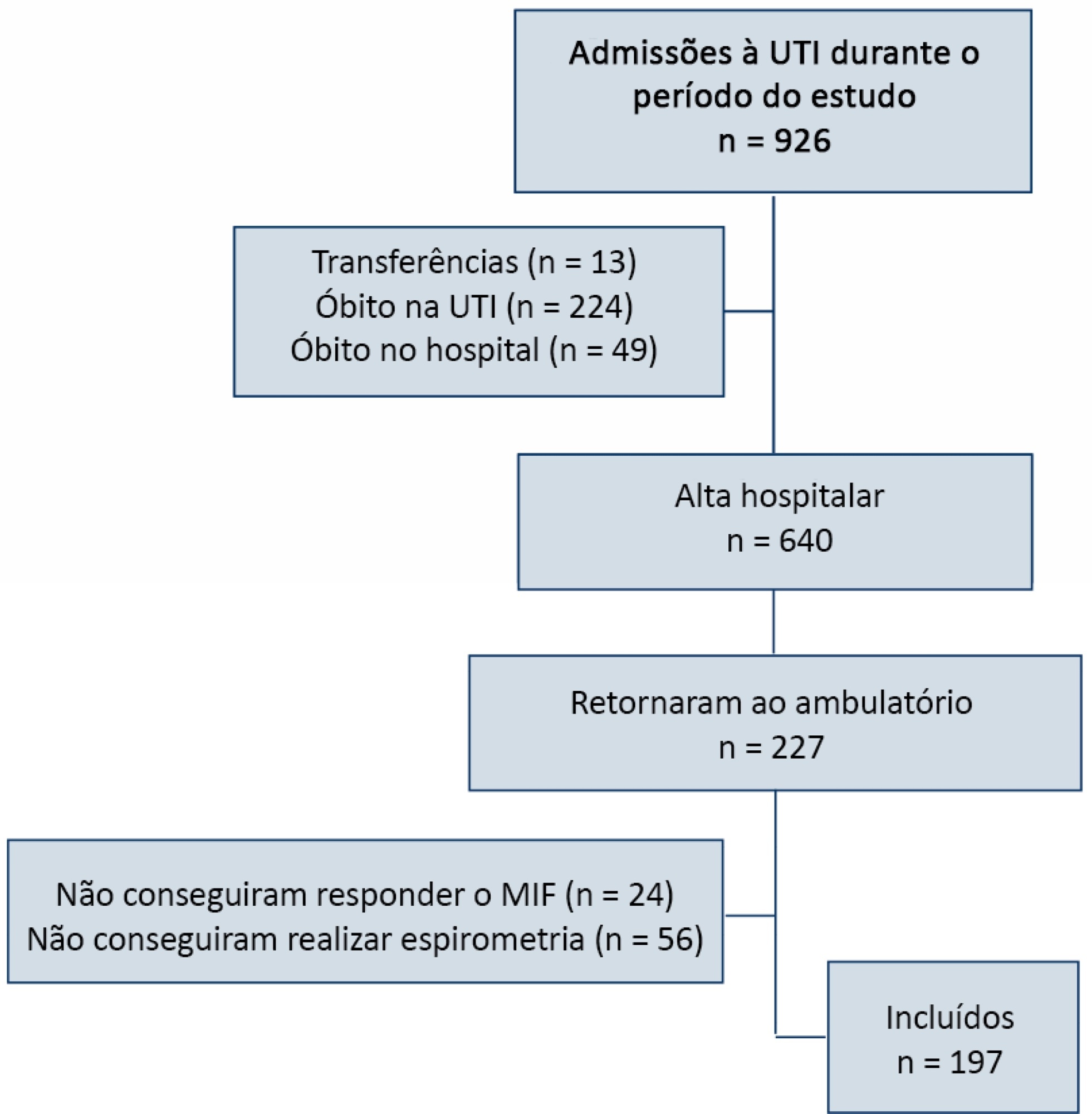
This was a retrospective cohort study conducted in one adult intensive care unit and a multi-professional post-intensive care unit outpatient clinic of a single center. Patients admitted to the intensive care unit from January 2012 to December 2013 who underwent (3 months later) spirometry and answered the Functional Independence Measure Questionnaire were included.
Patients were divided into groups according to the classification of functional independence and spirometry. The study included 197 patients who were divided into greater dependence (n = 4), lower dependence (n = 12) and independent (n = 181) groups. Comparing the three groups, regarding the classification of the Functional Independence Measure, patients with greater dependence had higher Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment values at intensive care unit admission with more advanced age, more days on mechanical ventilation, and longer stay in the intensive care unit and hospital. The majority of patients presented with pulmonary impairment, which was the obstructive pattern observed most frequently. When comparing functional independence with pulmonary function, it was observed that the lower the functional status, the worse the pulmonary function, with a significant difference being observed in peak expiratory flow (p = 0.030).
The majority of patients who returned to the outpatient clinic 3 months after discharge had good functional status but did present with pulmonary impairment, which is related to the degree of functional dependence.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):243-250
DOI 10.5935/0103-507X.20210031
To relate functional independence to the degree of pulmonary impairment in adult patients 3 months after discharge from the intensive care unit.
This was a retrospective cohort study conducted in one adult intensive care unit and a multi-professional post-intensive care unit outpatient clinic of a single center. Patients admitted to the intensive care unit from January 2012 to December 2013 who underwent (3 months later) spirometry and answered the Functional Independence Measure Questionnaire were included.
Patients were divided into groups according to the classification of functional independence and spirometry. The study included 197 patients who were divided into greater dependence (n = 4), lower dependence (n = 12) and independent (n = 181) groups. Comparing the three groups, regarding the classification of the Functional Independence Measure, patients with greater dependence had higher Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment values at intensive care unit admission with more advanced age, more days on mechanical ventilation, and longer stay in the intensive care unit and hospital. The majority of patients presented with pulmonary impairment, which was the obstructive pattern observed most frequently. When comparing functional independence with pulmonary function, it was observed that the lower the functional status, the worse the pulmonary function, with a significant difference being observed in peak expiratory flow (p = 0.030).
The majority of patients who returned to the outpatient clinic 3 months after discharge had good functional status but did present with pulmonary impairment, which is related to the degree of functional dependence.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):261-265
DOI 10.5935/0103-507X.20210033
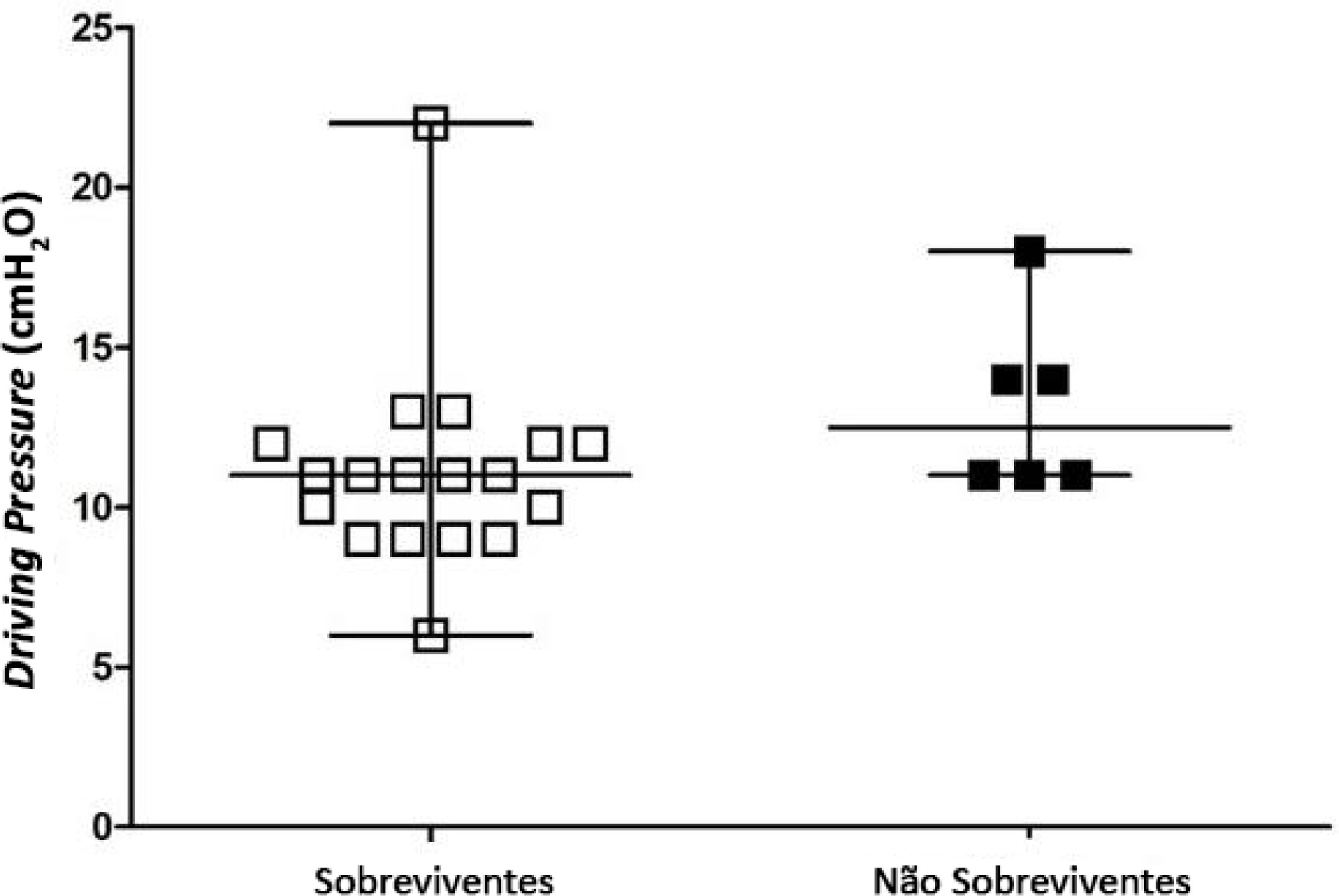
To identify the possible association between driving pressure and mechanical power values and oxygenation index on the first day of mechanical ventilation with the mortality of trauma patients without a diagnosis of acute respiratory distress syndrome.
Patients under pressure-controlled or volume-controlled ventilation were included, with data collection 24 hours after orotracheal intubation. Patient follow-up was performed for 30 days to obtain the clinical outcome. The patients were admitted to two intensive care units of the Hospital de Pronto Socorro de Porto Alegre from June to September 2019.
A total of 24 patients were evaluated. Driving pressure, mechanical power and oxygenation index were similar among patients who survived and those who died, with no statistically significant difference between groups.
Driving pressure, mechanical power and oxygenation index values obtained on the first day of mechanical ventilation were not associated with mortality of trauma patients without acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):261-265
DOI 10.5935/0103-507X.20210033
To identify the possible association between driving pressure and mechanical power values and oxygenation index on the first day of mechanical ventilation with the mortality of trauma patients without a diagnosis of acute respiratory distress syndrome.
Patients under pressure-controlled or volume-controlled ventilation were included, with data collection 24 hours after orotracheal intubation. Patient follow-up was performed for 30 days to obtain the clinical outcome. The patients were admitted to two intensive care units of the Hospital de Pronto Socorro de Porto Alegre from June to September 2019.
A total of 24 patients were evaluated. Driving pressure, mechanical power and oxygenation index were similar among patients who survived and those who died, with no statistically significant difference between groups.
Driving pressure, mechanical power and oxygenation index values obtained on the first day of mechanical ventilation were not associated with mortality of trauma patients without acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):68-74
DOI 10.5935/0103-507X.20210006
To analyze whether changes in medical care due to the application of COVID-19 protocols affected clinical outcomes in patients without COVID-19 during the pandemic.
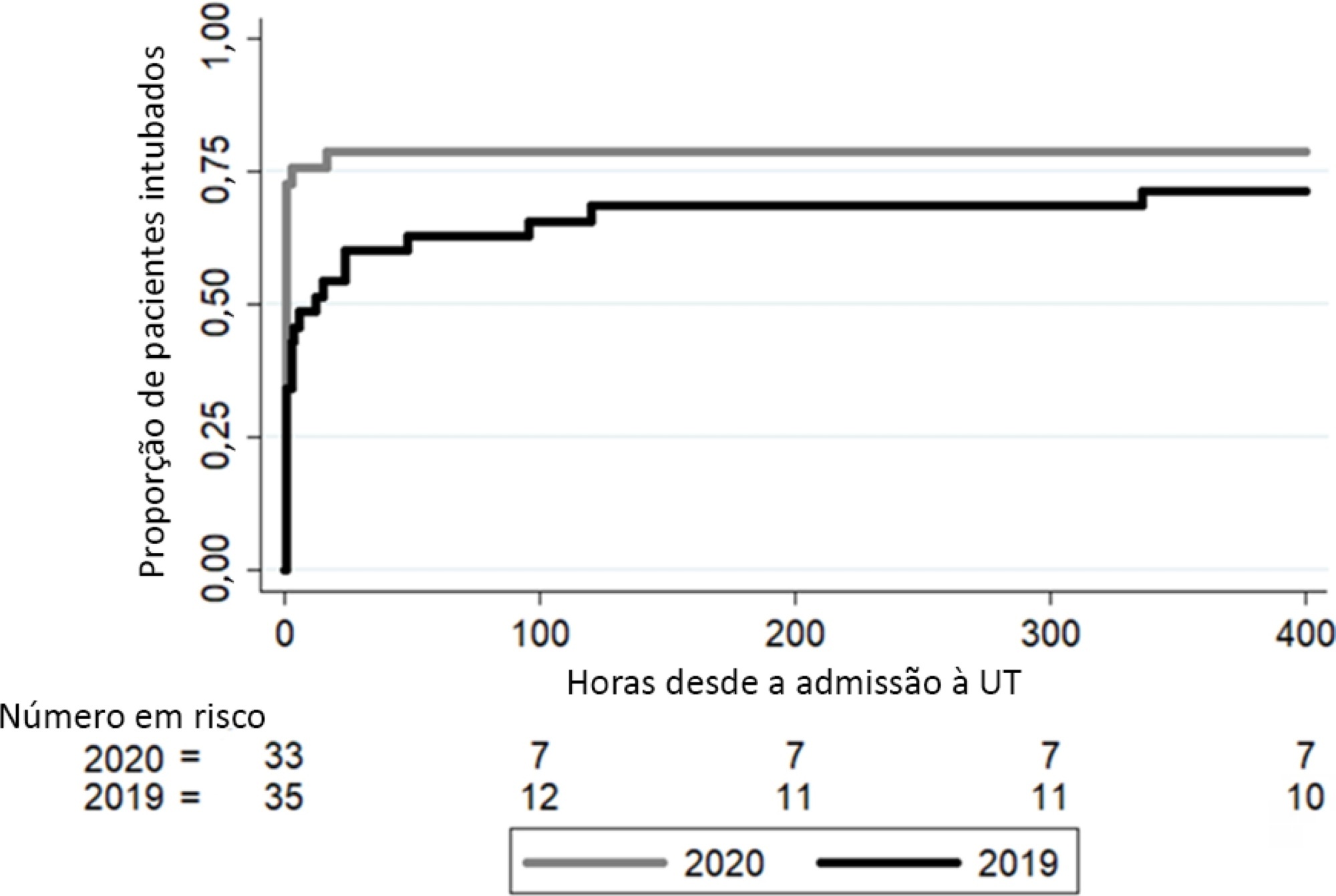
This was a retrospective, observational cohort study carried out in a thirty-eight-bed surgical and medical intensive care unit of a high complexity private hospital. Patients with respiratory failure admitted to the intensive care unit during March and April 2020 and the same months in 2019 were selected. We compared interventions and outcomes of patients without COVID-19 during the pandemic with patients admitted in 2019. The main variables analyzed were intensive care unit respiratory management, number of chest tomography scans and bronchoalveolar lavages, intensive care unit complications, and status at hospital discharge.
In 2020, a significant reduction in the use of a high-flow nasal cannula was observed: 14 (42%) in 2019 compared to 1 (3%) in 2020. Additionally, in 2020, a significant increase was observed in the number of patients under mechanical ventilation admitted to the intensive care unit from the emergency department, 23 (69%) compared to 11 (31%) in 2019. Nevertheless, the number of patients with mechanical ventilation after 5 days of admission was similar in both years: 24 (69%) in 2019 and 26 (79%) in 2020.
Intensive care unit protocols based on international recommendations for the COVID-19 pandemic have produced a change in non-COVID-19 patient management. We observed a reduction in the use of a high-flow nasal cannula and an increased number of tracheal intubations in the emergency department. However, no changes in the percentage of intubated patients in the intensive care unit, the number of mechanical ventilation days or the length of stay in intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):68-74
DOI 10.5935/0103-507X.20210006
To analyze whether changes in medical care due to the application of COVID-19 protocols affected clinical outcomes in patients without COVID-19 during the pandemic.
This was a retrospective, observational cohort study carried out in a thirty-eight-bed surgical and medical intensive care unit of a high complexity private hospital. Patients with respiratory failure admitted to the intensive care unit during March and April 2020 and the same months in 2019 were selected. We compared interventions and outcomes of patients without COVID-19 during the pandemic with patients admitted in 2019. The main variables analyzed were intensive care unit respiratory management, number of chest tomography scans and bronchoalveolar lavages, intensive care unit complications, and status at hospital discharge.
In 2020, a significant reduction in the use of a high-flow nasal cannula was observed: 14 (42%) in 2019 compared to 1 (3%) in 2020. Additionally, in 2020, a significant increase was observed in the number of patients under mechanical ventilation admitted to the intensive care unit from the emergency department, 23 (69%) compared to 11 (31%) in 2019. Nevertheless, the number of patients with mechanical ventilation after 5 days of admission was similar in both years: 24 (69%) in 2019 and 26 (79%) in 2020.
Intensive care unit protocols based on international recommendations for the COVID-19 pandemic have produced a change in non-COVID-19 patient management. We observed a reduction in the use of a high-flow nasal cannula and an increased number of tracheal intubations in the emergency department. However, no changes in the percentage of intubated patients in the intensive care unit, the number of mechanical ventilation days or the length of stay in intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):82-87
DOI 10.5935/0103-507X.20210008
To assess the frequency of multidisciplinary rounds during ICU days, to evaluate the participation of diverse healthcare professionals, to identify the reasons why rounds were not performed on specific days, and whether bed occupancy rate and nurse workload were associated with the conduction of multidisciplinary rounds.
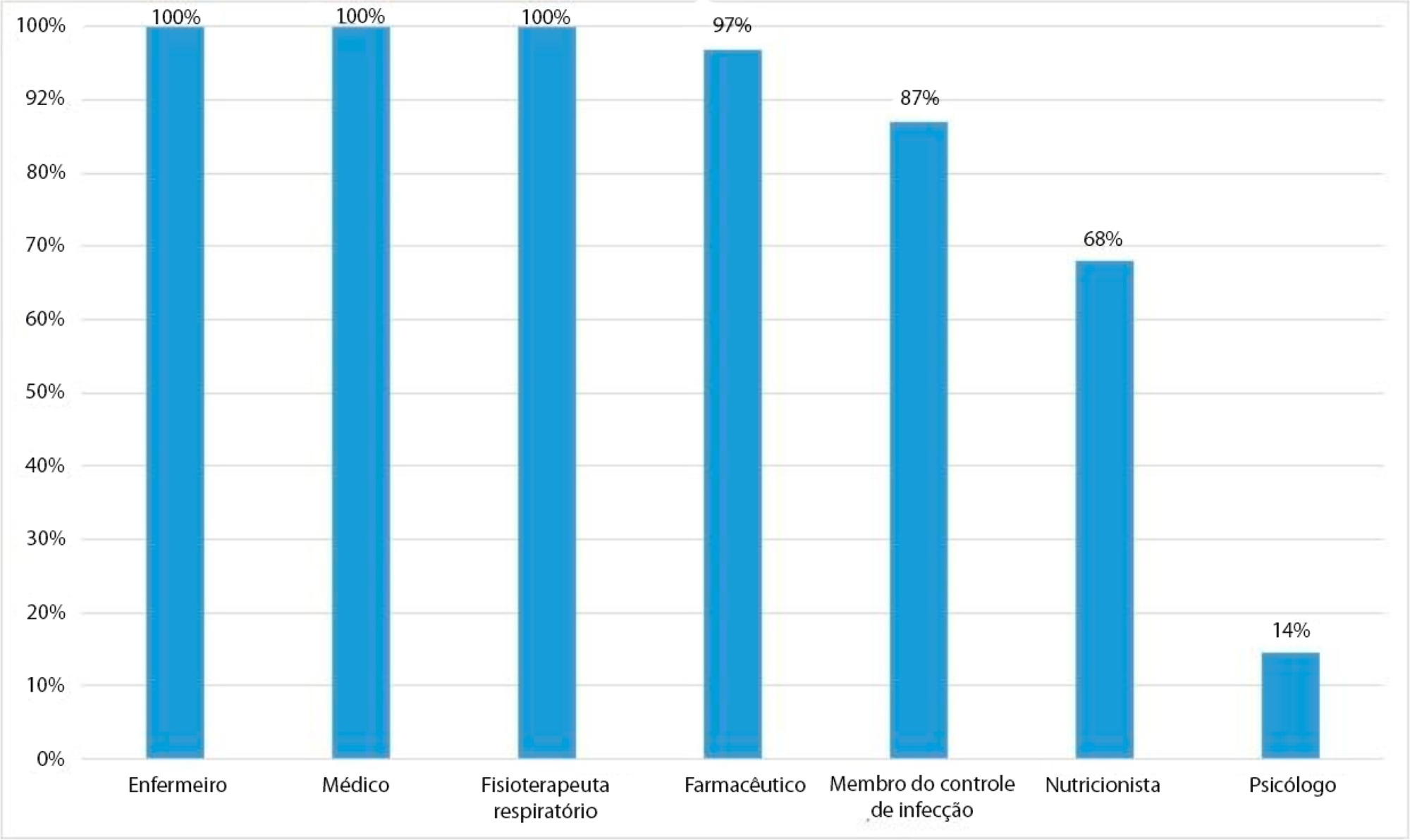
We performed a cross-sectional study to assess the frequency of multidisciplinary rounds in four intensive care units in a cancer center. We also collected data on rates of professional participation, reasons for not performing rounds when they did not occur, and daily bed occupancy rates and assessed nurse workload by measuring the Nursing Activity Score.
Rounds were conducted on 595 (65.8%) of 889 surveyed intensive care unit days. Nurses, physicians, respiratory therapists, pharmacists, and infection control practitioners participated most often. Rounds did not occur due to admission of new patients at the scheduled time (136; 44.7%) and involvement of nurses in activities unrelated to patients’ care (97; 31.9%). In multivariate analysis, higher Nursing Activity Scores were associated with greater odds of conducting multidisciplinary rounds (OR = 1.06; 95%CI 1.04 - 1.10; p < 0.01), whereas bed occupancy rates were not (OR = 0.99; 95%CI 0.97 - 1.00; p = 0.18).
Multidisciplinary rounds were conducted on less than two-thirds of surveyed intensive care unit days. Many rounds were cancelled due to activities unrelated to patient care. Unexpectedly, increased workload was associated with higher odds of conducting rounds. Workload is a possible trigger to discuss daily goals to improve patient outcomes and to enhance the effectiveness of multidisciplinary teams.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):82-87
DOI 10.5935/0103-507X.20210008
To assess the frequency of multidisciplinary rounds during ICU days, to evaluate the participation of diverse healthcare professionals, to identify the reasons why rounds were not performed on specific days, and whether bed occupancy rate and nurse workload were associated with the conduction of multidisciplinary rounds.
We performed a cross-sectional study to assess the frequency of multidisciplinary rounds in four intensive care units in a cancer center. We also collected data on rates of professional participation, reasons for not performing rounds when they did not occur, and daily bed occupancy rates and assessed nurse workload by measuring the Nursing Activity Score.
Rounds were conducted on 595 (65.8%) of 889 surveyed intensive care unit days. Nurses, physicians, respiratory therapists, pharmacists, and infection control practitioners participated most often. Rounds did not occur due to admission of new patients at the scheduled time (136; 44.7%) and involvement of nurses in activities unrelated to patients’ care (97; 31.9%). In multivariate analysis, higher Nursing Activity Scores were associated with greater odds of conducting multidisciplinary rounds (OR = 1.06; 95%CI 1.04 - 1.10; p < 0.01), whereas bed occupancy rates were not (OR = 0.99; 95%CI 0.97 - 1.00; p = 0.18).
Multidisciplinary rounds were conducted on less than two-thirds of surveyed intensive care unit days. Many rounds were cancelled due to activities unrelated to patient care. Unexpectedly, increased workload was associated with higher odds of conducting rounds. Workload is a possible trigger to discuss daily goals to improve patient outcomes and to enhance the effectiveness of multidisciplinary teams.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):528-534
DOI 10.5935/0103-507X.20200090
To describe the characteristics and outcomes of patients undergoing mechanical ventilation withdrawal and to compare them to mechanically ventilated patients with limitations (withhold or withdrawal) of life-sustaining therapies but who did not undergo mechanical ventilation withdrawal.
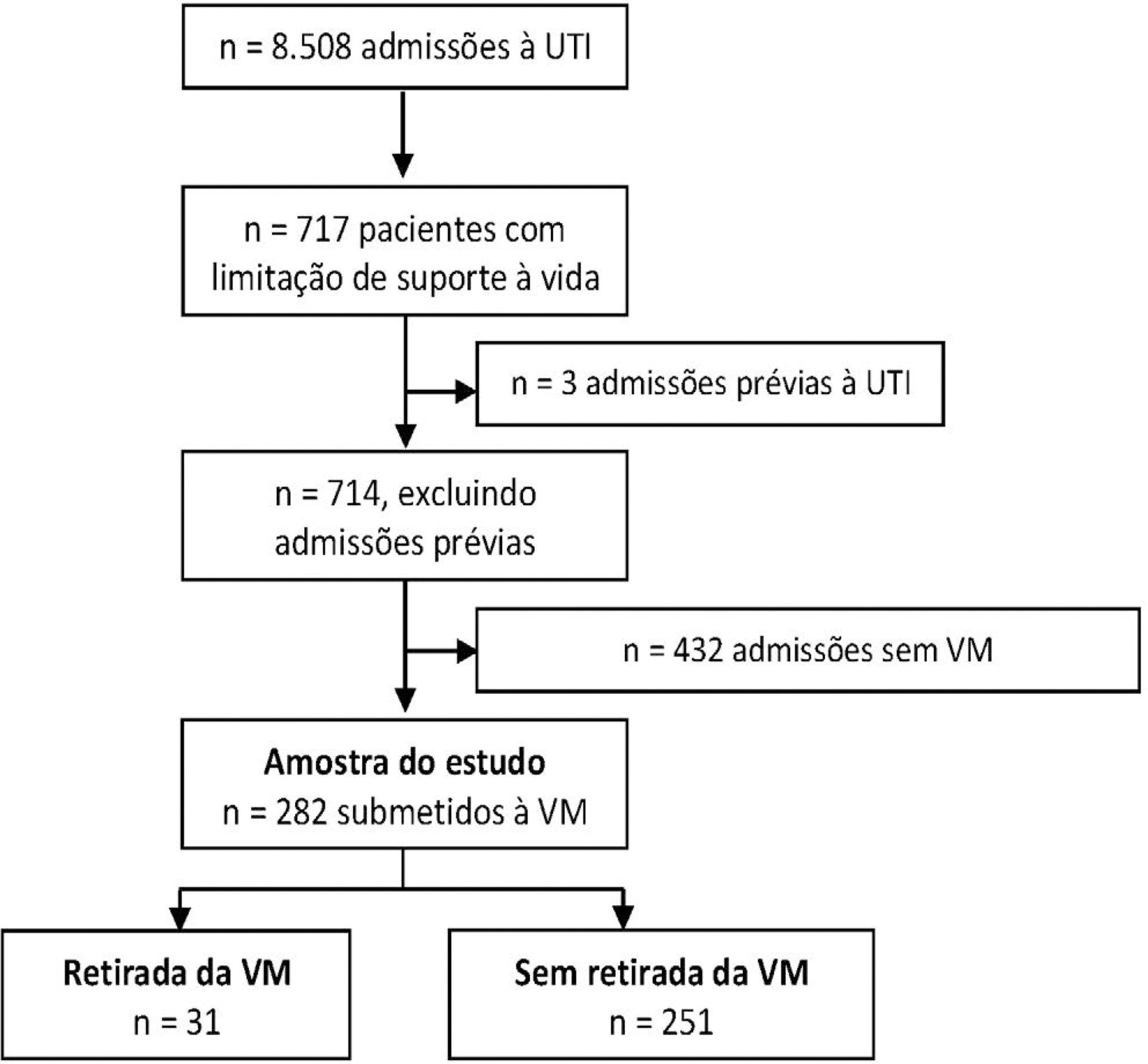
This was a retrospective cohort study from January 2014 to December 2018 of mechanically ventilated patients with any organ support limitation admitted to a single intensive care unit. We compared patients who underwent mechanical ventilation withdrawal and those who did not regarding intensive care unit and hospital mortality and length of stay in both an unadjusted analysis and a propensity score matched subsample. We also analyzed the time from mechanical ventilation withdrawal to death.
Out of 282 patients with life-sustaining therapy limitations, 31 (11%) underwent mechanical ventilation withdrawal. There was no baseline difference between groups. Intensive care unit and hospital mortality rates were 71% versus 57% and 93% versus 80%, respectively, among patients who underwent mechanical ventilation withdrawal and those who did not. The median intensive care unit length of stay was 7 versus 8 days (p = 0.6), and the hospital length of stay was 9 versus 15 days (p = 0.015). Hospital mortality was not significantly different (25/31; 81% versus 29/31; 93%; p = 0.26) after matching. The median time from mechanical ventilation withdrawal until death was 2 days [0 - 5], and 10/31 (32%) patients died within 24 hours after mechanical ventilation withdrawal.
In this Brazilian report, mechanical ventilation withdrawal represented 11% of all patients with treatment limitations and was not associated with increased hospital mortality after propensity score matching on relevant covariates.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):528-534
DOI 10.5935/0103-507X.20200090
To describe the characteristics and outcomes of patients undergoing mechanical ventilation withdrawal and to compare them to mechanically ventilated patients with limitations (withhold or withdrawal) of life-sustaining therapies but who did not undergo mechanical ventilation withdrawal.
This was a retrospective cohort study from January 2014 to December 2018 of mechanically ventilated patients with any organ support limitation admitted to a single intensive care unit. We compared patients who underwent mechanical ventilation withdrawal and those who did not regarding intensive care unit and hospital mortality and length of stay in both an unadjusted analysis and a propensity score matched subsample. We also analyzed the time from mechanical ventilation withdrawal to death.
Out of 282 patients with life-sustaining therapy limitations, 31 (11%) underwent mechanical ventilation withdrawal. There was no baseline difference between groups. Intensive care unit and hospital mortality rates were 71% versus 57% and 93% versus 80%, respectively, among patients who underwent mechanical ventilation withdrawal and those who did not. The median intensive care unit length of stay was 7 versus 8 days (p = 0.6), and the hospital length of stay was 9 versus 15 days (p = 0.015). Hospital mortality was not significantly different (25/31; 81% versus 29/31; 93%; p = 0.26) after matching. The median time from mechanical ventilation withdrawal until death was 2 days [0 - 5], and 10/31 (32%) patients died within 24 hours after mechanical ventilation withdrawal.
In this Brazilian report, mechanical ventilation withdrawal represented 11% of all patients with treatment limitations and was not associated with increased hospital mortality after propensity score matching on relevant covariates.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):603-605
DOI 10.5935/0103-507X.20200098
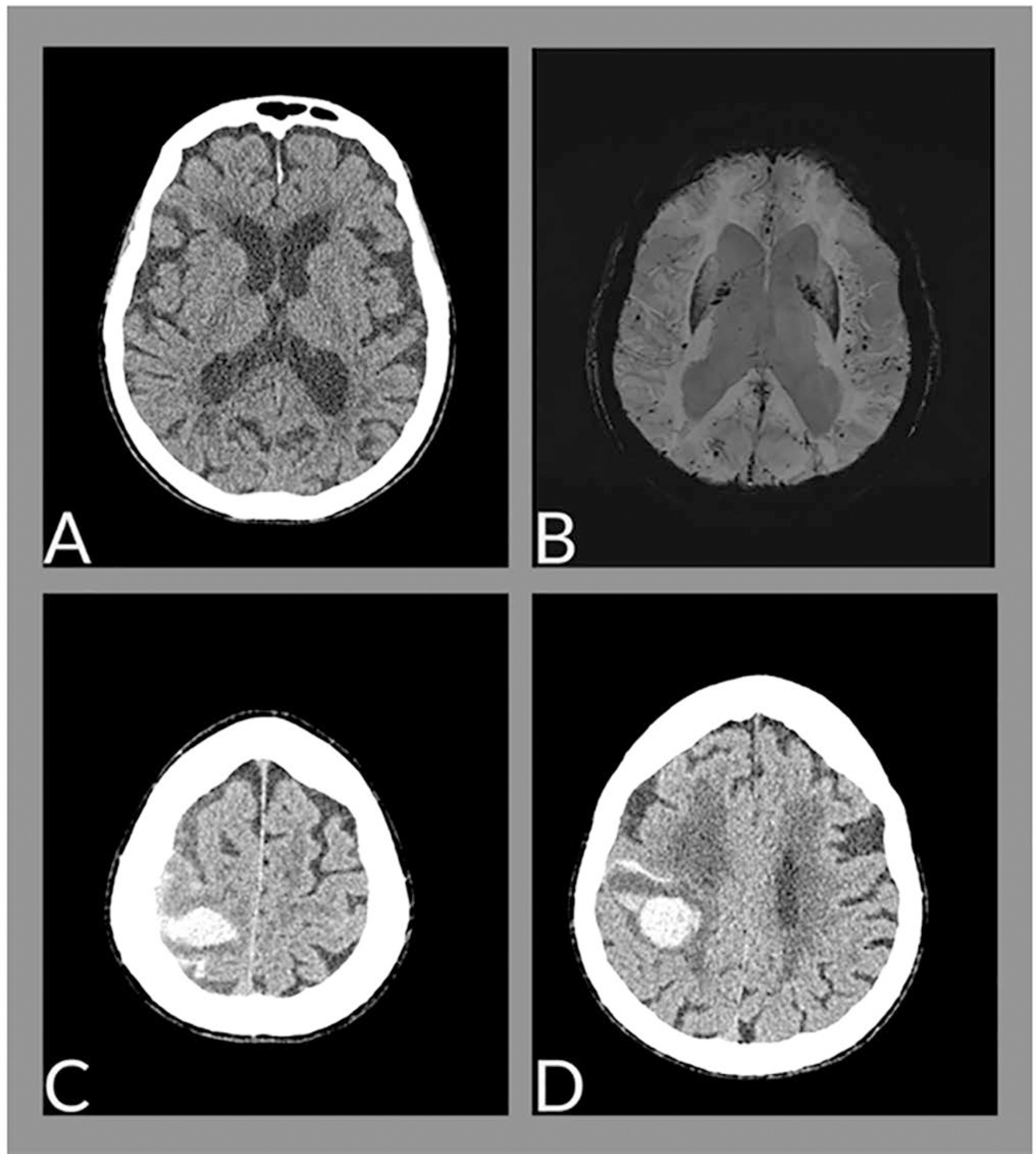
The neurological changes associated with COVID-19 have been frequently described, especially in cases of greater severity, and are related to multifactorial causes, such as endothelial dysfunction, inflammatory mediator release (cytokine storm), endothelial dysfunction and hypoxemia. We report the case of a female patient, 88 years old, with cerebral hemorrhage associated with amyloid angiopathy in the context of SARS-CoV-2 infection.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):603-605
DOI 10.5935/0103-507X.20200098
The neurological changes associated with COVID-19 have been frequently described, especially in cases of greater severity, and are related to multifactorial causes, such as endothelial dysfunction, inflammatory mediator release (cytokine storm), endothelial dysfunction and hypoxemia. We report the case of a female patient, 88 years old, with cerebral hemorrhage associated with amyloid angiopathy in the context of SARS-CoV-2 infection.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):493-505
DOI 10.5935/0103-507X.20200081
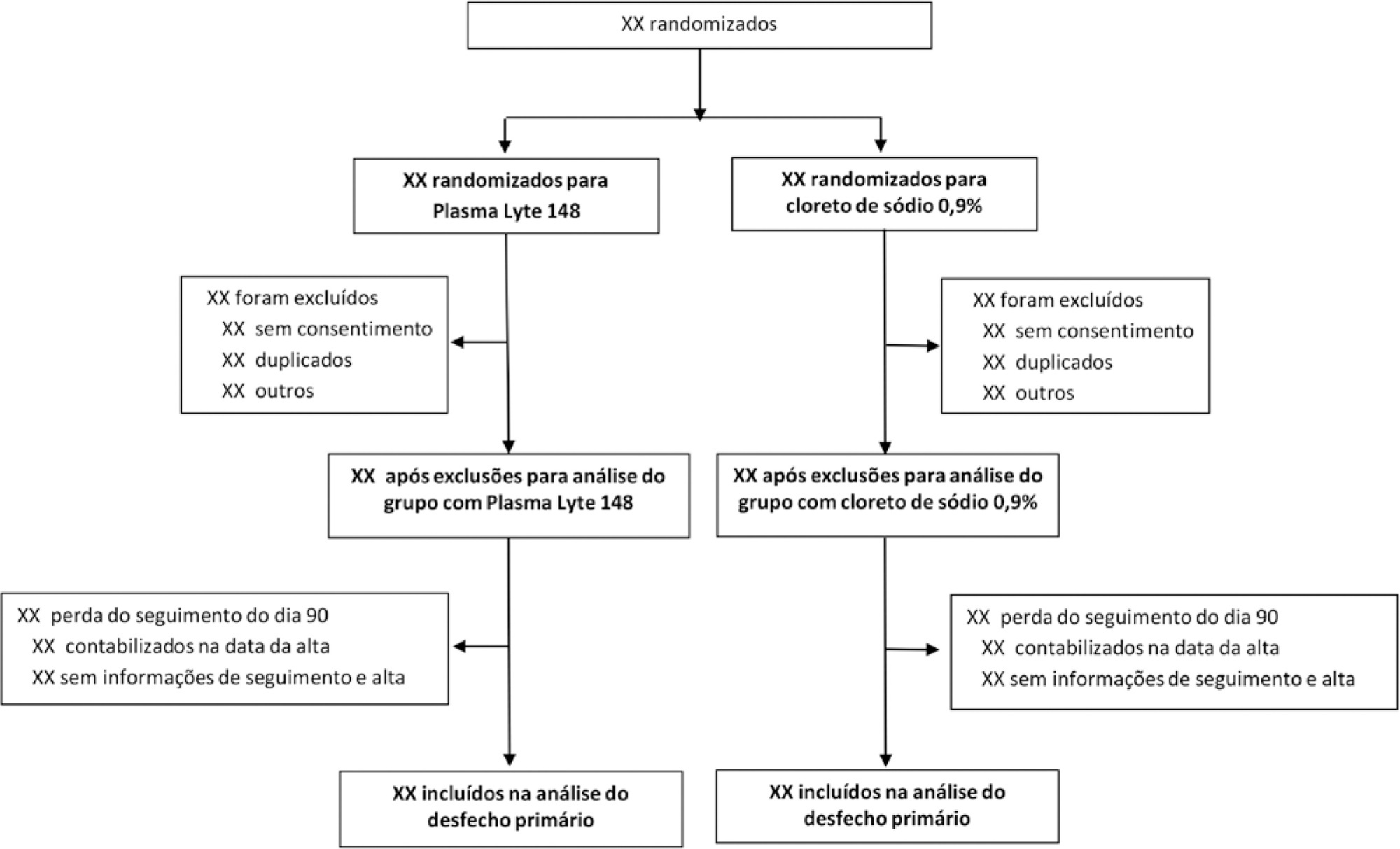
To report the statistical analysis plan (first version) for the Balanced Solutions versus Saline in Intensive Care Study (BaSICS).
BaSICS is a multicenter factorial randomized controlled trial that will assess the effects of Plasma-Lyte 148 versus 0.9% saline as the fluid of choice in critically ill patients, as well as the effects of a slow (333mL/h) versus rapid (999mL/h) infusion speed during fluid challenges, on important patient outcomes. The fluid type will be blinded for investigators, patients and the analyses. No blinding will be possible for the infusion speed for the investigators, but all analyses will be kept blinded during the analysis procedure.
BaSICS will have 90-day mortality as its primary endpoint, which will be tested using mixed-effects Cox proportional hazard models, considering sites as a random variable (frailty models) adjusted for age, organ dysfunction and admission type. Important secondary endpoints include renal replacement therapy up to 90 days, acute renal failure, organ dysfunction at days 3 and 7, and mechanical ventilation-free days within 28 days.
This manuscript provides details on the first version of the statistical analysis plan for the BaSICS trial and will guide the study’s analysis when follow-up is finished.
Abstract
Rev Bras Ter Intensiva. 2020;32(4):493-505
DOI 10.5935/0103-507X.20200081
To report the statistical analysis plan (first version) for the Balanced Solutions versus Saline in Intensive Care Study (BaSICS).
BaSICS is a multicenter factorial randomized controlled trial that will assess the effects of Plasma-Lyte 148 versus 0.9% saline as the fluid of choice in critically ill patients, as well as the effects of a slow (333mL/h) versus rapid (999mL/h) infusion speed during fluid challenges, on important patient outcomes. The fluid type will be blinded for investigators, patients and the analyses. No blinding will be possible for the infusion speed for the investigators, but all analyses will be kept blinded during the analysis procedure.
BaSICS will have 90-day mortality as its primary endpoint, which will be tested using mixed-effects Cox proportional hazard models, considering sites as a random variable (frailty models) adjusted for age, organ dysfunction and admission type. Important secondary endpoints include renal replacement therapy up to 90 days, acute renal failure, organ dysfunction at days 3 and 7, and mechanical ventilation-free days within 28 days.
This manuscript provides details on the first version of the statistical analysis plan for the BaSICS trial and will guide the study’s analysis when follow-up is finished.