Você pesquisou por y - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(3):393-402
DOI 10.5935/0103-507X.20190062
To review the scientific evidence regarding the initiation of enteral nutrition in the pediatric burn population.
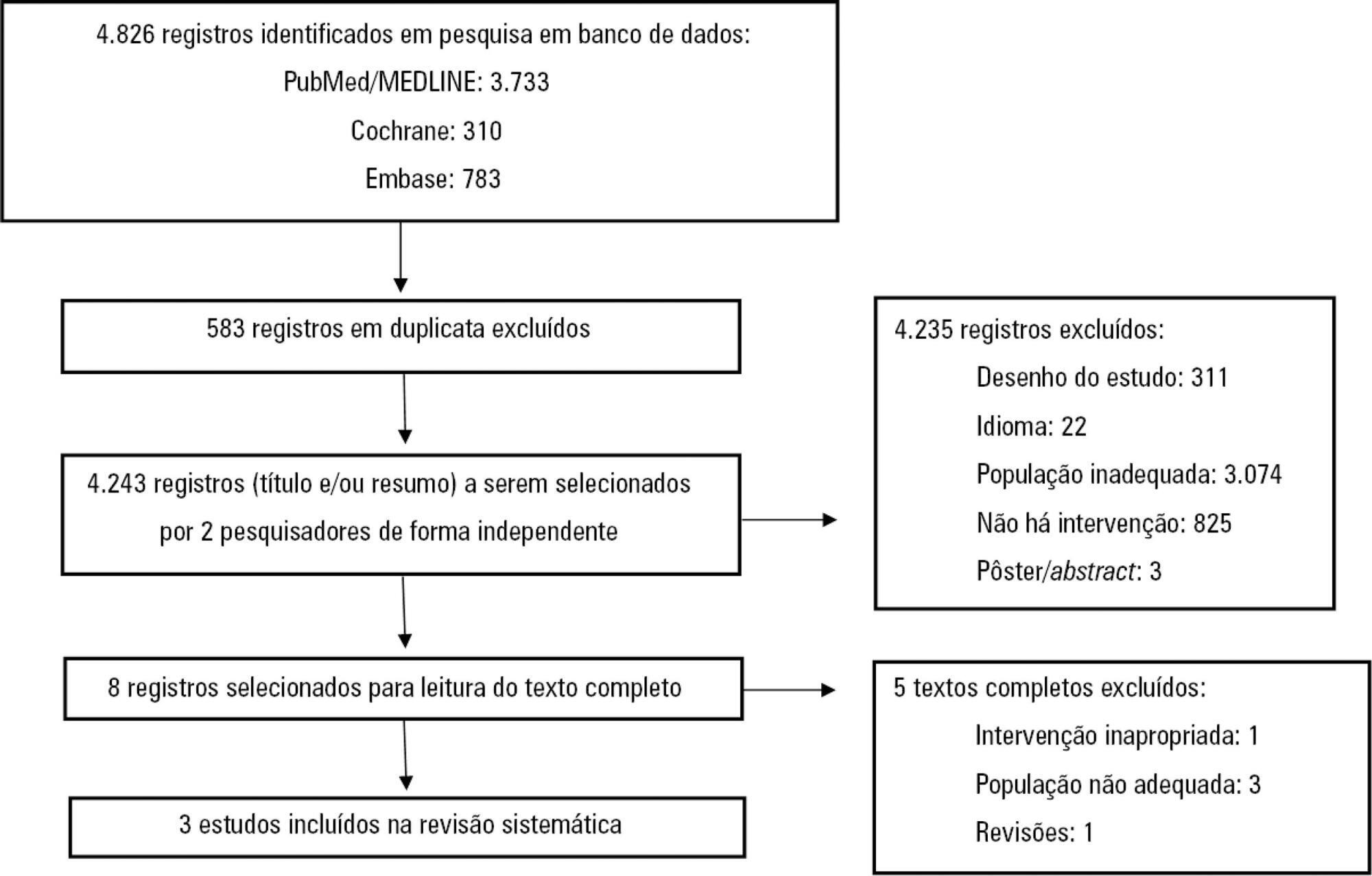
This study was a systematic review and meta-analysis of randomized clinical trials comparing early enteral nutrition and late enteral nutrition in individuals aged 1 month to 18 years with burns. The MEDLINE/PubMed, Embase and Cochrane Library databases were searched using the terms "burns", "fires", "child nutrition disorders", "nutritional support" and related terms.
Three articles that included a total of 781 patients were identified. There was no significant difference in the mortality rate between the early and late groups (OR = 0.72, 95%CI = 0.46 - 1.15, p = 0.17). Patients who received early enteral nutrition had a 3.69-day reduction in the length of hospital stay (mean difference = -3.69, 95%CI = -4.11 - -3.27, p < 0.00001). There was a higher incidence of diarrhea and vomiting and decreased intestinal permeability in the early group. This group also presented higher a serum insulin concentration and insulin/glucagon ratio as well as lower caloric deficit and weight loss when compared to the control group.
Analysis of the different intragroup variables suggests the importance of starting nutritional support early. Considering the number of pediatric burn patients, there is a need for robust studies with greater scientific impact.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):393-402
DOI 10.5935/0103-507X.20190062
To review the scientific evidence regarding the initiation of enteral nutrition in the pediatric burn population.
This study was a systematic review and meta-analysis of randomized clinical trials comparing early enteral nutrition and late enteral nutrition in individuals aged 1 month to 18 years with burns. The MEDLINE/PubMed, Embase and Cochrane Library databases were searched using the terms "burns", "fires", "child nutrition disorders", "nutritional support" and related terms.
Three articles that included a total of 781 patients were identified. There was no significant difference in the mortality rate between the early and late groups (OR = 0.72, 95%CI = 0.46 - 1.15, p = 0.17). Patients who received early enteral nutrition had a 3.69-day reduction in the length of hospital stay (mean difference = -3.69, 95%CI = -4.11 - -3.27, p < 0.00001). There was a higher incidence of diarrhea and vomiting and decreased intestinal permeability in the early group. This group also presented higher a serum insulin concentration and insulin/glucagon ratio as well as lower caloric deficit and weight loss when compared to the control group.
Analysis of the different intragroup variables suggests the importance of starting nutritional support early. Considering the number of pediatric burn patients, there is a need for robust studies with greater scientific impact.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):403-409
DOI 10.5935/0103-507X.20190050
Brain death, defined as the complete and irreversible loss of brain functions, has a history that is linked to the emergence of intensive care units and the advancement of artificial ventilatory support. In Brazil, by federal law, the criteria for the diagnosis of brain death have been defined by the Federal Council of Medicine since 1997 and apply to the entire Brazilian territory. Resolution 2,173/2017 of the Federal Council of Medicine updated the criteria for diagnosing brain death. These changes include the following: the requirement for the patient to meet specific physiological prerequisites and for the physician to provide optimized care to the patient before starting the procedures for diagnosing brain death and to perform complementary tests, as well as the need for specific training for physicians who make this diagnosis. Other changes include the reduction of the time interval between the two clinical examinations, the possibility of continuing procedures in the presence of unilateral ear or eye injury, the performance of a single apnea test and the creation of a statement of brain death determination that includes the recording of all procedures in a single document. This document, despite the controversy surrounding it, increases the safety necessary when establishing a diagnosis of such importance and has positive implications that extend beyond the patient and the physician to reach the entire health system.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):403-409
DOI 10.5935/0103-507X.20190050
Brain death, defined as the complete and irreversible loss of brain functions, has a history that is linked to the emergence of intensive care units and the advancement of artificial ventilatory support. In Brazil, by federal law, the criteria for the diagnosis of brain death have been defined by the Federal Council of Medicine since 1997 and apply to the entire Brazilian territory. Resolution 2,173/2017 of the Federal Council of Medicine updated the criteria for diagnosing brain death. These changes include the following: the requirement for the patient to meet specific physiological prerequisites and for the physician to provide optimized care to the patient before starting the procedures for diagnosing brain death and to perform complementary tests, as well as the need for specific training for physicians who make this diagnosis. Other changes include the reduction of the time interval between the two clinical examinations, the possibility of continuing procedures in the presence of unilateral ear or eye injury, the performance of a single apnea test and the creation of a statement of brain death determination that includes the recording of all procedures in a single document. This document, despite the controversy surrounding it, increases the safety necessary when establishing a diagnosis of such importance and has positive implications that extend beyond the patient and the physician to reach the entire health system.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):410-424
DOI 10.5935/0103-507X.20190063
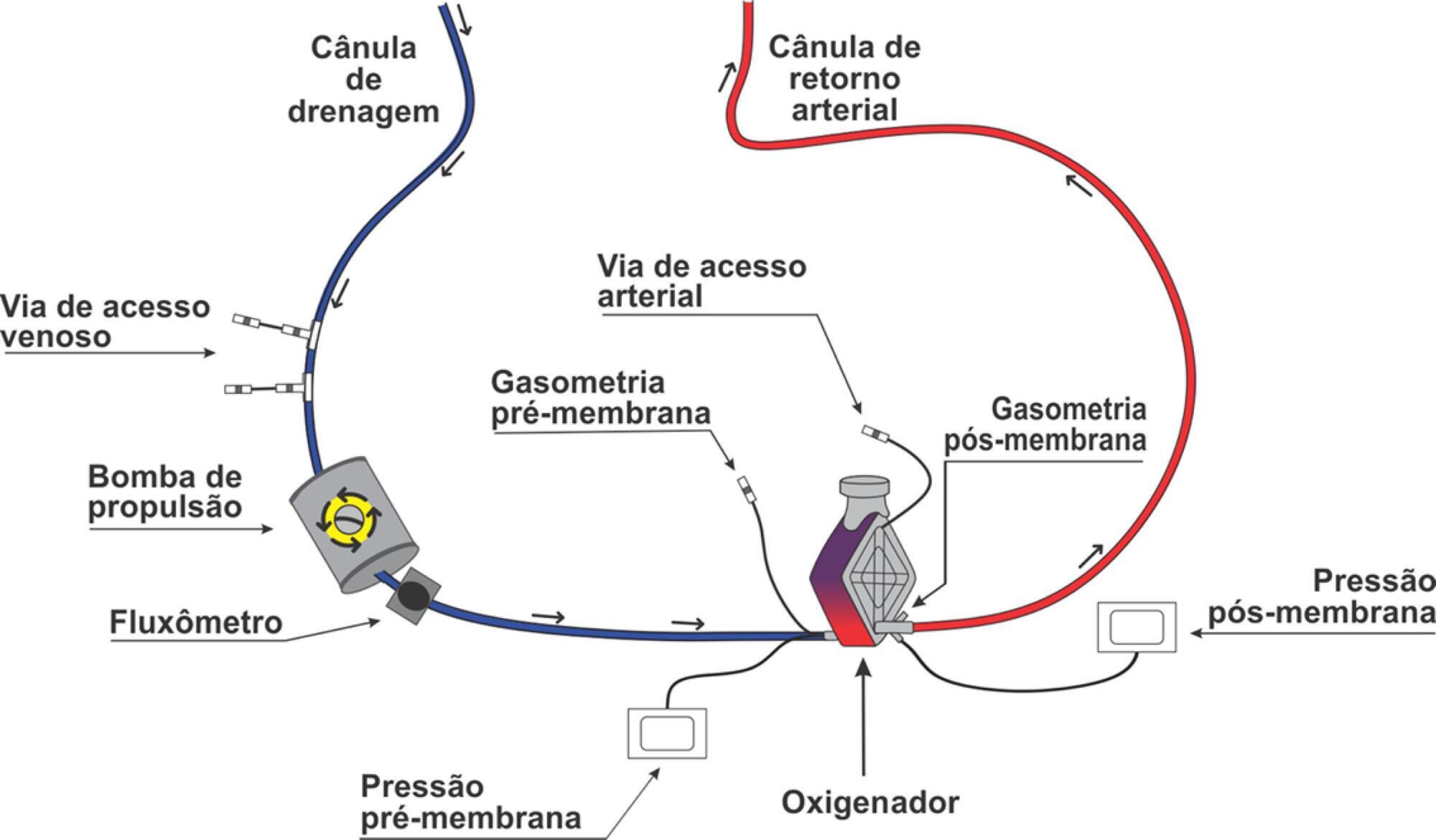
Extracorporeal membrane oxygenation is a modality of extracorporeal life support that allows for temporary support in pulmonary and/or cardiac failure refractory to conventional therapy. Since the first descriptions of extracorporeal membrane oxygenation, significant improvements have occurred in the device and the management of patients and, consequently, in the outcomes of critically ill patients during extracorporeal membrane oxygenation. Many important studies about the use of extracorporeal membrane oxygenation in patients with acute respiratory distress syndrome refractory to conventional clinical support, under in-hospital cardiac arrest and with cardiogenic refractory shock have been published in recent years. The objective of this literature review is to present the theoretical and practical aspects of extracorporeal membrane oxygenation support for respiratory and/or cardiac functions in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):410-424
DOI 10.5935/0103-507X.20190063
Extracorporeal membrane oxygenation is a modality of extracorporeal life support that allows for temporary support in pulmonary and/or cardiac failure refractory to conventional therapy. Since the first descriptions of extracorporeal membrane oxygenation, significant improvements have occurred in the device and the management of patients and, consequently, in the outcomes of critically ill patients during extracorporeal membrane oxygenation. Many important studies about the use of extracorporeal membrane oxygenation in patients with acute respiratory distress syndrome refractory to conventional clinical support, under in-hospital cardiac arrest and with cardiogenic refractory shock have been published in recent years. The objective of this literature review is to present the theoretical and practical aspects of extracorporeal membrane oxygenation support for respiratory and/or cardiac functions in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):425-427
DOI 10.5935/0103-507X.20190046
Abstract
Rev Bras Ter Intensiva. 2019;31(3):425-427
DOI 10.5935/0103-507X.20190046
Abstract
Rev Bras Ter Intensiva. 2019;31(3):428-429
DOI 10.5935/0103-507X.20190048
Abstract
Rev Bras Ter Intensiva. 2019;31(3):428-429
DOI 10.5935/0103-507X.20190048