
You searched for:"Rodrigo Magalhães Gurgel"
We found (2) results for your search.-
Clinical Report
Prospective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
- ,
- Israel Silva Maia
 ,
, - Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini , [ … ],
- Fernando Godinho Zampieri
Abstract
Clinical ReportProspective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
Crit Care Sci. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini ,
- Júlia Souza Oliveira,
- Erica Regina Ribeiro Sady ,
- Letícia Galvão Barbante,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel,
- Lucas Petri Damiani ,
- Karina Leal Negrelli,
- Tamiris Abait Miranda,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira,
- Glauco Adrieno Westphal ,
- Ruthy Perotto Fernandes,
- Cássio Luis Zandonai ,
- Mariangela Pimentel Pincelli ,
- Rodrigo Cruvinel Figueiredo,
- Cíntia Loss Sartori Bustamante,
- Luiz Fernando Norbin,
- Emerson Boschi ,
- Rafael Lessa,
- Marcelo Pereira Romano ,
- Mieko Cláudia Miura ,
- Meton Soares de Alencar Filho ,
- Vicente Cés de Souza Dantas ,
- Priscilla Alves Barreto,
- Mauro Esteves Hernandes ,
- Cintia Magalhães Carvalho Grion ,
- Alexandre Sanches Laranjeira,
- Ana Luiza Mezzaroba ,
- Marina Bahl ,
- Ana Carolina Starke ,
- Rodrigo Santos Biondi ,
- Felipe Dal-Pizzol ,
- Eliana Bernadete Caser,
- Marlus Muri Thompson,
- Andrea Allegrini Padial,
- Viviane Cordeiro Veiga ,
- Rodrigo Thot Leite,
- Gustavo Araújo,
- Mário Guimarães,
- Priscilla de Aquino Martins ,
- Fábio Holanda Lacerda ,
- Conrado Roberto Hoffmann Filho ,
- Livia Melro ,
- Eduardo Pacheco,
- Gustavo Adolfo Ospina-Táscon ,
- Juliana Carvalho Ferreira ,
- Fabricio Jocundo Calado Freires ,
- Flávia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
- Fernando Godinho Zampieri
Views77ABSTRACT
Background:
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
Objective:
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
Methods:
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
Outcomes:
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
Conclusion:
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Keywords:Extracorporeal membrane oxygenationPneumoniaPositive pressure respirationRespiration, artificialRespiratory distress syndromeVentilator-induced lung injurySee moreViews77

Abstract
Clinical ReportProspective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
Crit Care Sci. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini ,
- Júlia Souza Oliveira,
- Erica Regina Ribeiro Sady ,
- Letícia Galvão Barbante,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel,
- Lucas Petri Damiani ,
- Karina Leal Negrelli,
- Tamiris Abait Miranda,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira,
- Glauco Adrieno Westphal ,
- Ruthy Perotto Fernandes,
- Cássio Luis Zandonai ,
- Mariangela Pimentel Pincelli ,
- Rodrigo Cruvinel Figueiredo,
- Cíntia Loss Sartori Bustamante,
- Luiz Fernando Norbin,
- Emerson Boschi ,
- Rafael Lessa,
- Marcelo Pereira Romano ,
- Mieko Cláudia Miura ,
- Meton Soares de Alencar Filho ,
- Vicente Cés de Souza Dantas ,
- Priscilla Alves Barreto,
- Mauro Esteves Hernandes ,
- Cintia Magalhães Carvalho Grion ,
- Alexandre Sanches Laranjeira,
- Ana Luiza Mezzaroba ,
- Marina Bahl ,
- Ana Carolina Starke ,
- Rodrigo Santos Biondi ,
- Felipe Dal-Pizzol ,
- Eliana Bernadete Caser,
- Marlus Muri Thompson,
- Andrea Allegrini Padial,
- Viviane Cordeiro Veiga ,
- Rodrigo Thot Leite,
- Gustavo Araújo,
- Mário Guimarães,
- Priscilla de Aquino Martins ,
- Fábio Holanda Lacerda ,
- Conrado Roberto Hoffmann Filho ,
- Livia Melro ,
- Eduardo Pacheco,
- Gustavo Adolfo Ospina-Táscon ,
- Juliana Carvalho Ferreira ,
- Fabricio Jocundo Calado Freires ,
- Flávia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
- Fernando Godinho Zampieri
Views77ABSTRACT
Background:
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
Objective:
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
Methods:
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
Outcomes:
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
Conclusion:
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Keywords:Extracorporeal membrane oxygenationPneumoniaPositive pressure respirationRespiration, artificialRespiratory distress syndromeVentilator-induced lung injurySee more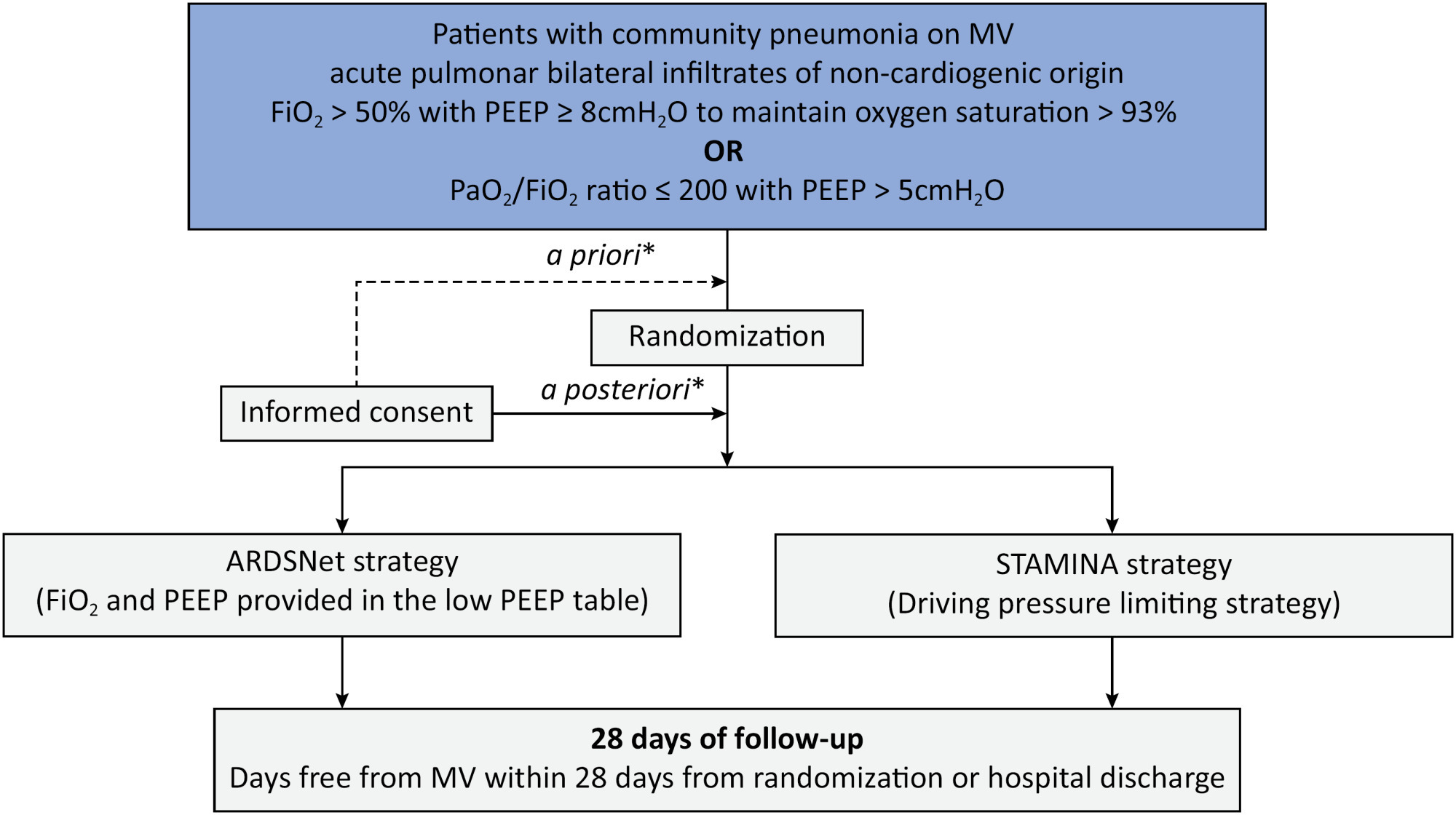
-
Special Article
Automated documentation of vital parameters in wards using portable stations – Effect on proper triggering of the rapid response team: a study protocol of a cluster randomized clinical trial
- José Cesar Ribeiro ,
- Cristina Sgorbissa ,
- Karla Aparecida Silva,
- Maria de Lourdes Dias Braz ,
- Ana Clara Peneluppi Horak , [ … ],
- Aline Marcadenti
Abstract
Special ArticleAutomated documentation of vital parameters in wards using portable stations – Effect on proper triggering of the rapid response team: a study protocol of a cluster randomized clinical trial
Rev Bras Ter Intensiva. 2022;34(3):319-326
DOI 10.5935/0103-507X.20220101-en
- José Cesar Ribeiro ,
- Cristina Sgorbissa ,
- Karla Aparecida Silva,
- Maria de Lourdes Dias Braz ,
- Ana Clara Peneluppi Horak ,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel ,
- Samira Martins Tokunaga ,
- Karina Leal Negrelli ,
- Gabriela Souza Murizine ,
- Fernando Medrado Júnior ,
- Rita de Cassia Pires Coli ,
- Alexandre Biasi Cavalcanti ,
- Aline Marcadenti
Views2ABSTRACT
Objective:
To evaluate the effectiveness of the Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ solution in activating the rapid response team in a timely manner compared to manual activation.
Methods:
The Hillrom study is a single-center, open-label, superiority, cluster-randomized, parallel-group (1:1 allocation ratio) clinical trial that will be conducted in a tertiary hospital. Two sets of three wards with 28 beds will be included (one as the intervention cluster and the other as the control). The wards will be randomly assigned to use the Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ automated solution (intervention cluster) or to maintain the usual routine (control cluster) regarding rapid response team activation. The primary outcome will be the absolute number of episodes of rapid response team triggering in an appropriate time; as secondary outcomes, clinical features (mortality, cardiac arrest, need for intensive care unit admission and duration of hospitalization) will be assessed according to clusters in an exploratory way. A sample size of 216 rapid response team activations was estimated to identify a possible difference between the groups. The protocol has been approved by the institutional Research Ethics Committee.
Expected results:
The Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ automated solution is expected to be more effective in triggering the nurse call system to activate the rapid response team in a timely and adequate manner compared to manual triggering (usual practice).
ClinicalTrials.gov:
NCT04648579
Keywords:computerizedHealth information interoperabilityHospital rapid response teamMedical records systemsNursing stationsVital signsSee moreViews2Abstract
Special ArticleAutomated documentation of vital parameters in wards using portable stations – Effect on proper triggering of the rapid response team: a study protocol of a cluster randomized clinical trial
Rev Bras Ter Intensiva. 2022;34(3):319-326
DOI 10.5935/0103-507X.20220101-en
- José Cesar Ribeiro ,
- Cristina Sgorbissa ,
- Karla Aparecida Silva,
- Maria de Lourdes Dias Braz ,
- Ana Clara Peneluppi Horak ,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel ,
- Samira Martins Tokunaga ,
- Karina Leal Negrelli ,
- Gabriela Souza Murizine ,
- Fernando Medrado Júnior ,
- Rita de Cassia Pires Coli ,
- Alexandre Biasi Cavalcanti ,
- Aline Marcadenti
Views2ABSTRACT
Objective:
To evaluate the effectiveness of the Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ solution in activating the rapid response team in a timely manner compared to manual activation.
Methods:
The Hillrom study is a single-center, open-label, superiority, cluster-randomized, parallel-group (1:1 allocation ratio) clinical trial that will be conducted in a tertiary hospital. Two sets of three wards with 28 beds will be included (one as the intervention cluster and the other as the control). The wards will be randomly assigned to use the Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ automated solution (intervention cluster) or to maintain the usual routine (control cluster) regarding rapid response team activation. The primary outcome will be the absolute number of episodes of rapid response team triggering in an appropriate time; as secondary outcomes, clinical features (mortality, cardiac arrest, need for intensive care unit admission and duration of hospitalization) will be assessed according to clusters in an exploratory way. A sample size of 216 rapid response team activations was estimated to identify a possible difference between the groups. The protocol has been approved by the institutional Research Ethics Committee.
Expected results:
The Welch Allyn Connex® Spot Monitor/Hillrom Connecta™ automated solution is expected to be more effective in triggering the nurse call system to activate the rapid response team in a timely and adequate manner compared to manual triggering (usual practice).
ClinicalTrials.gov:
NCT04648579
Keywords:computerizedHealth information interoperabilityHospital rapid response teamMedical records systemsNursing stationsVital signsSee more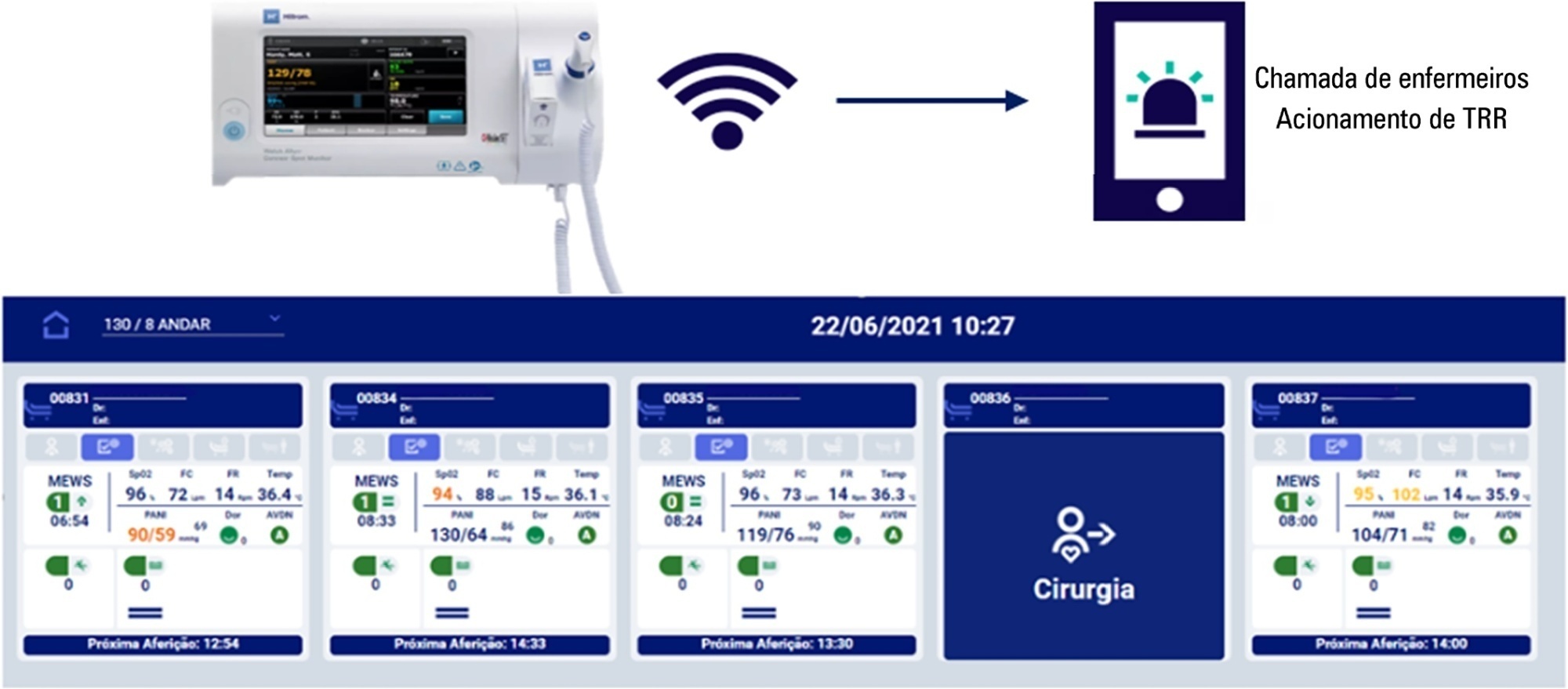
- José Cesar Ribeiro
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis