
You searched for:"Marco Aurélio de Valois Correia Júnior"
We found (2) results for your search.-
Original Articles – Clinical Research
Expiratory peak flow and respiratory system resistance in mechanically ventilated patients undergoing two different forms of manually assisted cough
Rev Bras Ter Intensiva. 2012;24(1):58-63
Abstract
Original Articles – Clinical ResearchExpiratory peak flow and respiratory system resistance in mechanically ventilated patients undergoing two different forms of manually assisted cough
Rev Bras Ter Intensiva. 2012;24(1):58-63
DOI 10.1590/S0103-507X2012000100009
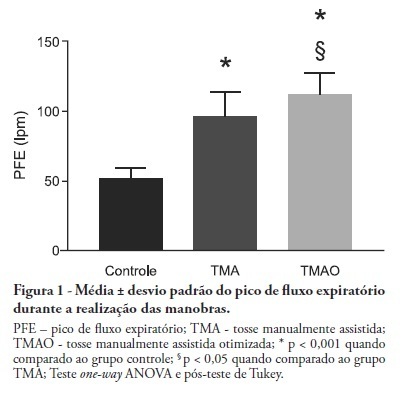
Views0See moreOBJECTIVE: Mechanical ventilation is associated with retained airway secretions. Manually assisted cough contributes to the displacement of bronchial mucus, whereas positive end-expiratory pressure increases collateral ventilation and maintains airway patency. This study aimed to assess the effects of manually assisted cough, either alone or added to increased positive end-expiratory pressure and inspiratory time (optimized manually assisted cough), on the expiratory peak flow and respiratory system mechanics in mechanically ventilated patients. METHODS: In this controlled and randomized clinical trial, respiratory mechanics and expiratory peak flow were assessed in male and female patients undergoing either tracheal suctioning alone, manually assisted cough followed by tracheal suctioning or optimized manually assisted cough followed by tracheal suctioning. RESULTS: Thirty-five patients completed the trial. Respiratory system resistance was significantly reduced after optimized manually assisted cough (16.0 ± 3.6 versus 12.4 ± 3.1 cmH2O/L/s; p = 0.04). The expiratory peak flow during optimized manually assisted cough was significantly higher in comparison with the values observed during manually assisted cough (112.3 ± 15.6 versus 95.8 ± 18.3 Lpm; p < 0.05). Both values were significantly higher than the values observed in the group undergoing tracheal suctioning alone (52.0 ± 7.6 Lpm; p < 0.001). CONCLUSION: Optimized manually assisted cough increases the expiratory peak flow in comparison with manually assisted cough; in addition, this procedure reduces respiratory system resistance.
Views0

Abstract
Original Articles – Clinical ResearchExpiratory peak flow and respiratory system resistance in mechanically ventilated patients undergoing two different forms of manually assisted cough
Rev Bras Ter Intensiva. 2012;24(1):58-63
DOI 10.1590/S0103-507X2012000100009
Views0See moreOBJECTIVE: Mechanical ventilation is associated with retained airway secretions. Manually assisted cough contributes to the displacement of bronchial mucus, whereas positive end-expiratory pressure increases collateral ventilation and maintains airway patency. This study aimed to assess the effects of manually assisted cough, either alone or added to increased positive end-expiratory pressure and inspiratory time (optimized manually assisted cough), on the expiratory peak flow and respiratory system mechanics in mechanically ventilated patients. METHODS: In this controlled and randomized clinical trial, respiratory mechanics and expiratory peak flow were assessed in male and female patients undergoing either tracheal suctioning alone, manually assisted cough followed by tracheal suctioning or optimized manually assisted cough followed by tracheal suctioning. RESULTS: Thirty-five patients completed the trial. Respiratory system resistance was significantly reduced after optimized manually assisted cough (16.0 ± 3.6 versus 12.4 ± 3.1 cmH2O/L/s; p = 0.04). The expiratory peak flow during optimized manually assisted cough was significantly higher in comparison with the values observed during manually assisted cough (112.3 ± 15.6 versus 95.8 ± 18.3 Lpm; p < 0.05). Both values were significantly higher than the values observed in the group undergoing tracheal suctioning alone (52.0 ± 7.6 Lpm; p < 0.001). CONCLUSION: Optimized manually assisted cough increases the expiratory peak flow in comparison with manually assisted cough; in addition, this procedure reduces respiratory system resistance.
-
Noise in the intensive care unit: quantification and perception by healthcare professionals
Rev Bras Ter Intensiva. 2010;22(4):369-374
Abstract
Noise in the intensive care unit: quantification and perception by healthcare professionals
Rev Bras Ter Intensiva. 2010;22(4):369-374
DOI 10.1590/S0103-507X2010000400010
Views0OBJECTIVE: The several multidisciplinary team personnel and device alarms make intensive care units noisy environments. This study aimed to measure the noise level of a medical-surgical intensive care unit in Recife, Brazil, and to assess the noise perception by the unit’s healthcare professionals. METHODS: A decibel meter was used for continuous every five seconds one week noise levels recording. After this measurement, an interview shaped noise perception questionnaire was applied to the healthcare professionals, approaching the discomfort level and noise control possibilities. RESULTS: Mean 58.21 ± 5.93 dB noise was recorded. The morning noise level was higher than at night (60.85 ± 4.90 versus 55.60 ± 5.98, p <0.001), as well as work-days versus weekend (58. 77 ± 6.05 versus 56.83 ± 5.90, p <0.001). The evening staff shift change noise was louder than by daytime change (62.31 ± 4.70 versus 61.35 ± 5.08 dB; p < 0.001). Of the 73 questionnaire respondents, 97.3% believe that the intensive care unit has moderate or intense noise levels; 50.7% consider the noise harmful; and 98.6% believe that noise levels can be reduced. CONCLUSION: The measured noise levels were above the recommended. Preventive and educational programs approaching the importance of noise levels reduction should be encouraged in intensive care units.
Keywords:Humanization of assistanceIntensive care unitsmonitoringNoiseNoise levelsOutcome assessment (Healthcare)See moreViews0Abstract
Noise in the intensive care unit: quantification and perception by healthcare professionals
Rev Bras Ter Intensiva. 2010;22(4):369-374
DOI 10.1590/S0103-507X2010000400010
Views0OBJECTIVE: The several multidisciplinary team personnel and device alarms make intensive care units noisy environments. This study aimed to measure the noise level of a medical-surgical intensive care unit in Recife, Brazil, and to assess the noise perception by the unit’s healthcare professionals. METHODS: A decibel meter was used for continuous every five seconds one week noise levels recording. After this measurement, an interview shaped noise perception questionnaire was applied to the healthcare professionals, approaching the discomfort level and noise control possibilities. RESULTS: Mean 58.21 ± 5.93 dB noise was recorded. The morning noise level was higher than at night (60.85 ± 4.90 versus 55.60 ± 5.98, p <0.001), as well as work-days versus weekend (58. 77 ± 6.05 versus 56.83 ± 5.90, p <0.001). The evening staff shift change noise was louder than by daytime change (62.31 ± 4.70 versus 61.35 ± 5.08 dB; p < 0.001). Of the 73 questionnaire respondents, 97.3% believe that the intensive care unit has moderate or intense noise levels; 50.7% consider the noise harmful; and 98.6% believe that noise levels can be reduced. CONCLUSION: The measured noise levels were above the recommended. Preventive and educational programs approaching the importance of noise levels reduction should be encouraged in intensive care units.
Keywords:Humanization of assistanceIntensive care unitsmonitoringNoiseNoise levelsOutcome assessment (Healthcare)See more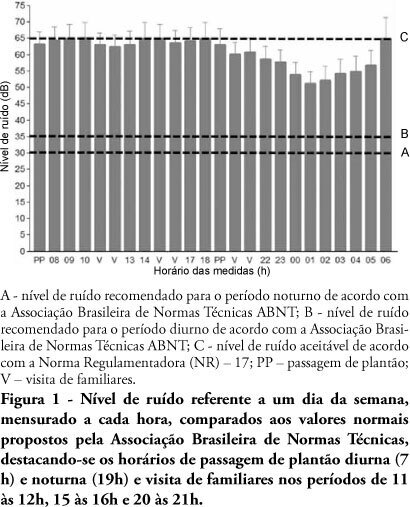
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis