postoperative care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval - 95%CI 3.3% - 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 - 4.0) days, and the length of hospital stay was 9.5 (5.4 - 18.6) days. The complication rate was 29.9% (95%CI 26.4 - 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 - 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio - OR = 1.02; 95%CI 1.01 - 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 - 1.25), surgical time (OR = 1.001, 95%CI 1.000 - 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 - 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 - 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 - 1.279), SOFA (OR = 1.175, 95%CI 1.069 - 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 - 6.051).
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval - 95%CI 3.3% - 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 - 4.0) days, and the length of hospital stay was 9.5 (5.4 - 18.6) days. The complication rate was 29.9% (95%CI 26.4 - 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 - 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio - OR = 1.02; 95%CI 1.01 - 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 - 1.25), surgical time (OR = 1.001, 95%CI 1.000 - 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 - 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 - 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 - 1.279), SOFA (OR = 1.175, 95%CI 1.069 - 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 - 6.051).
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):197-204
DOI 10.5935/0103-507X.20130035
To show that alterations in the plasma chloride concentration ([Cl-]plasma) during the postoperative period are largely dependent on the urinary strong ion difference ([SID]urine=[Na+]urine+[K+]urine-[Cl-]urine) and not on differences in fluid therapy.
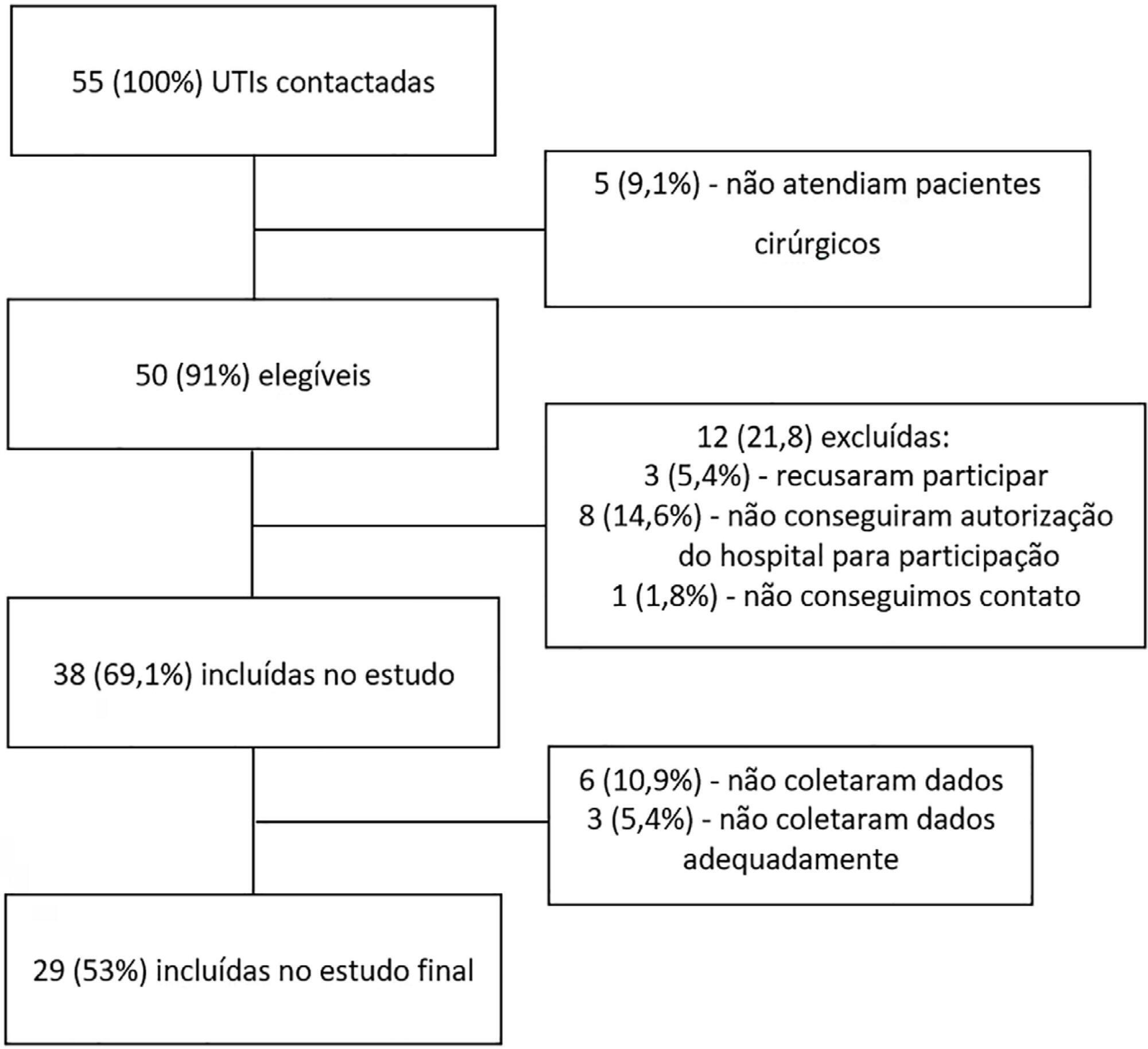
Measurements were performed at intensive care unit admission and 24 hours later in a total of 148 postoperative patients. Patients were assigned into one of three groups according to the change in [Cl-]plasma at the 24 hours time point: increased [Cl-]plasma (n=39), decreased [Cl-]plasma (n=56) or unchanged [Cl-]plasma (n=53).
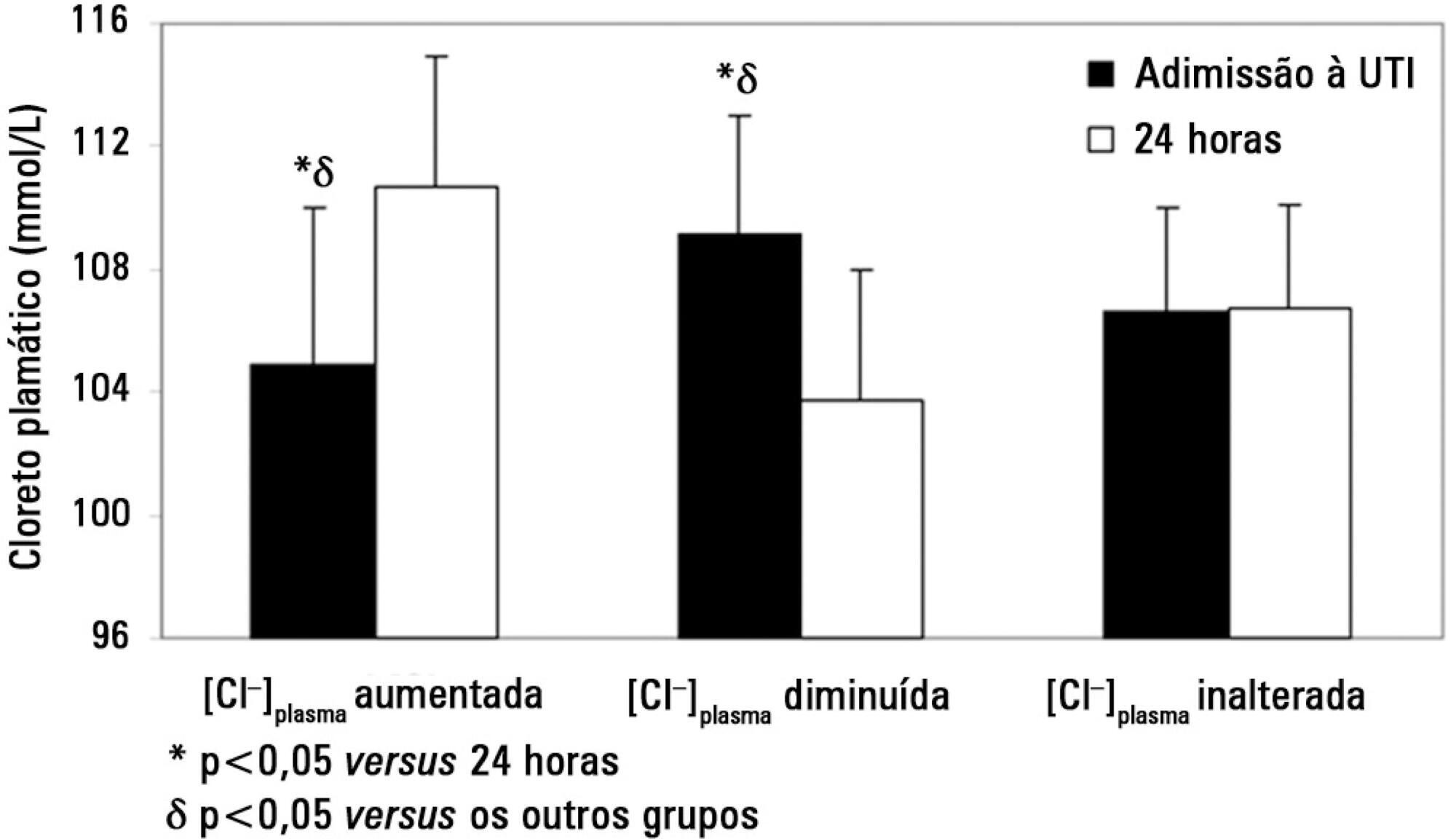
On admission, the increased [Cl-]plasma group had a lower [Cl-]plasma (105±5 versus 109±4 and 106±3mmol/L, p<0.05), a higher plasma anion gap concentration ([AG]plasma) and a higher strong ion gap concentration ([SIG]). After 24 hours, the increased [Cl-]plasma group showed a higher [Cl-]plasma (111±4 versus 104±4 and 107±3mmol/L, p<0.05) and lower [AG]plasma and [SIG]. The volume and [SID] of administered fluids were similar between groups except that the [SID]urine was higher (38±37 versus 18±22 and 23±18mmol/L, p<0.05) in the increased [Cl-]plasma group at the 24 hours time point. A multiple linear regression analysis showed that the [Cl-]plasma on admission and [SID]urine were independent predictors of the variation in [Cl-]plasma 24 hours later.
Changes in [Cl-]plasma during the first postoperative day were largely related to [SID]urine and [Cl-]plasma on admission and not to the characteristics of the infused fluids. Therefore, decreasing [SID]urine could be a major mechanism for preventing the development of salineinduced hyperchloremia.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):197-204
DOI 10.5935/0103-507X.20130035
To show that alterations in the plasma chloride concentration ([Cl-]plasma) during the postoperative period are largely dependent on the urinary strong ion difference ([SID]urine=[Na+]urine+[K+]urine-[Cl-]urine) and not on differences in fluid therapy.
Measurements were performed at intensive care unit admission and 24 hours later in a total of 148 postoperative patients. Patients were assigned into one of three groups according to the change in [Cl-]plasma at the 24 hours time point: increased [Cl-]plasma (n=39), decreased [Cl-]plasma (n=56) or unchanged [Cl-]plasma (n=53).
On admission, the increased [Cl-]plasma group had a lower [Cl-]plasma (105±5 versus 109±4 and 106±3mmol/L, p<0.05), a higher plasma anion gap concentration ([AG]plasma) and a higher strong ion gap concentration ([SIG]). After 24 hours, the increased [Cl-]plasma group showed a higher [Cl-]plasma (111±4 versus 104±4 and 107±3mmol/L, p<0.05) and lower [AG]plasma and [SIG]. The volume and [SID] of administered fluids were similar between groups except that the [SID]urine was higher (38±37 versus 18±22 and 23±18mmol/L, p<0.05) in the increased [Cl-]plasma group at the 24 hours time point. A multiple linear regression analysis showed that the [Cl-]plasma on admission and [SID]urine were independent predictors of the variation in [Cl-]plasma 24 hours later.
Changes in [Cl-]plasma during the first postoperative day were largely related to [SID]urine and [Cl-]plasma on admission and not to the characteristics of the infused fluids. Therefore, decreasing [SID]urine could be a major mechanism for preventing the development of salineinduced hyperchloremia.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):162-168
DOI 10.1590/S0103-507X2009000200008
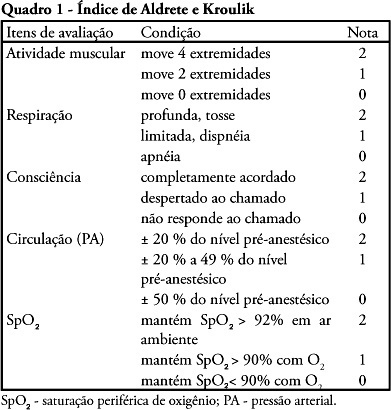
OBJECTIVE: The purpose of this study was to determine the place of stay at postoperative and to verify medical-surgical complications that would justify admission to the intensive care unit, including death. METHODS: Cross-over, prospective, open study that evaluated 120 patients who were submitted to primary bariatric surgery by video laparoscopy from May 2007 to April 2008 in a tertiary hospital. The Aldrete Kroulik index was used for release from the post-anesthesia recovery room and to define where the patient should be routinely referred for postoperative. RESULTS: Among the 120 patients, 83 were women and 37 men with a mean age ranging from 35.4 ± 10.5 years (18 to 66 years), body mass index 45.6 ± 10.5. The time between hospital admission and start of surgery was 140.7 ± 81.8 minutes, surgery time was 105 ± 28.6 minutes, time of post-anesthesia recovery room was between 125 ± 38 minutes and length of hospital stay was 47.7 ± 12.4 hours, with 100% of the patients walking in 24 hours. The Aldrete and Kroulik index in the post-anesthesia recovery room achieved scores of 10 to 120 minutes in all patients, with a 100% survival . CONCLUSION: Using the Aldrete and Kroulik index in the post-anesthesia of gastric bypass by video laparoscopy in primary bariatric surgery, no patient was admitted in intensive care unit and no major complication was observed.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):162-168
DOI 10.1590/S0103-507X2009000200008
OBJECTIVE: The purpose of this study was to determine the place of stay at postoperative and to verify medical-surgical complications that would justify admission to the intensive care unit, including death. METHODS: Cross-over, prospective, open study that evaluated 120 patients who were submitted to primary bariatric surgery by video laparoscopy from May 2007 to April 2008 in a tertiary hospital. The Aldrete Kroulik index was used for release from the post-anesthesia recovery room and to define where the patient should be routinely referred for postoperative. RESULTS: Among the 120 patients, 83 were women and 37 men with a mean age ranging from 35.4 ± 10.5 years (18 to 66 years), body mass index 45.6 ± 10.5. The time between hospital admission and start of surgery was 140.7 ± 81.8 minutes, surgery time was 105 ± 28.6 minutes, time of post-anesthesia recovery room was between 125 ± 38 minutes and length of hospital stay was 47.7 ± 12.4 hours, with 100% of the patients walking in 24 hours. The Aldrete and Kroulik index in the post-anesthesia recovery room achieved scores of 10 to 120 minutes in all patients, with a 100% survival . CONCLUSION: Using the Aldrete and Kroulik index in the post-anesthesia of gastric bypass by video laparoscopy in primary bariatric surgery, no patient was admitted in intensive care unit and no major complication was observed.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):205-209
DOI 10.1590/S0103-507X2007000200011
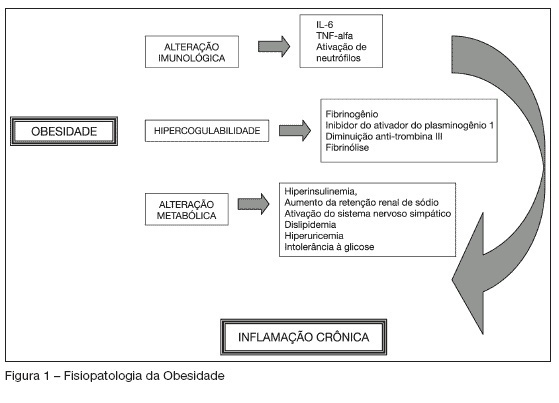
BACKGROUND AND OBJECTIVES: Obesity is an epidemic disease reaching more than 300 million people all over the world. Its prevalence has increased during the past few years and according to some studies its mortality in the critically ill patient seems to be much higher, especially among patients who were submitted to surgery. This study has as objective to discuss some particularities of managing obese patients in the intensive care unit after bariatric surgery. CONTENTS: The rate of obese patient in the ICU ranges from 9% to 26% and the increase in the number of bariatric surgeries has raised the number of obese patients in the ICU. It is important to know the physiopathology of obesity and to treat its particularities during the postoperative care. Such as pulmonary restriction, that causes an increase in pulmonary complications, coronary artery disease and thromboembolic events. CONCLUSIONS: The number of patients that undergo to bariatric surgery has increased; therefore, the number of obese patients in the ICU has also risen. Different physiological events and complications in obese patients are challenges to clinical practice. The knowledge of obese physiopathology helps in the managing routine procedures and complications after bariatric surgery.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):205-209
DOI 10.1590/S0103-507X2007000200011
BACKGROUND AND OBJECTIVES: Obesity is an epidemic disease reaching more than 300 million people all over the world. Its prevalence has increased during the past few years and according to some studies its mortality in the critically ill patient seems to be much higher, especially among patients who were submitted to surgery. This study has as objective to discuss some particularities of managing obese patients in the intensive care unit after bariatric surgery. CONTENTS: The rate of obese patient in the ICU ranges from 9% to 26% and the increase in the number of bariatric surgeries has raised the number of obese patients in the ICU. It is important to know the physiopathology of obesity and to treat its particularities during the postoperative care. Such as pulmonary restriction, that causes an increase in pulmonary complications, coronary artery disease and thromboembolic events. CONCLUSIONS: The number of patients that undergo to bariatric surgery has increased; therefore, the number of obese patients in the ICU has also risen. Different physiological events and complications in obese patients are challenges to clinical practice. The knowledge of obese physiopathology helps in the managing routine procedures and complications after bariatric surgery.