physical therapy Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(1):167-171
DOI 10.5935/0103-507X.20210018
The natural history of the disease, and the treatment of post-COVID-19 patients, are still being built. Symptoms are persistent, even in mild cases, and the infection consequences include fatigue, dyspnea, tachycardia, muscle loss, and reduced functional capacity. Regarding cardiopulmonary rehabilitation, there seems to be an improvement in functional capacity, quality of life, and prognosis with the 6-Minute Walk Test used as a prognostic and therapeutic evaluator. Therefore, this case series report aims to present our experience with four cases of different severity levels, involved in a post-COVID-19 cardiopulmonary rehabilitation program. These patients were assessed with the 6-Minute Walk Test, peripheral muscle strength, and double product at rest, to assess the results after a three-month rehabilitation protocol of at least 300 minutes per week. The four patients had their distance covered during the walk test increased between 16% and 94%. Peripheral muscle strength was improved by 20% to six times the baseline values, and double product at rest was reduced by 8% to 42%. The cardiopulmonary rehabilitation program had a positive impact on these cases, improving functional capacity despite the different severity levels in these post-COVID-19 cases.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):167-171
DOI 10.5935/0103-507X.20210018
The natural history of the disease, and the treatment of post-COVID-19 patients, are still being built. Symptoms are persistent, even in mild cases, and the infection consequences include fatigue, dyspnea, tachycardia, muscle loss, and reduced functional capacity. Regarding cardiopulmonary rehabilitation, there seems to be an improvement in functional capacity, quality of life, and prognosis with the 6-Minute Walk Test used as a prognostic and therapeutic evaluator. Therefore, this case series report aims to present our experience with four cases of different severity levels, involved in a post-COVID-19 cardiopulmonary rehabilitation program. These patients were assessed with the 6-Minute Walk Test, peripheral muscle strength, and double product at rest, to assess the results after a three-month rehabilitation protocol of at least 300 minutes per week. The four patients had their distance covered during the walk test increased between 16% and 94%. Peripheral muscle strength was improved by 20% to six times the baseline values, and double product at rest was reduced by 8% to 42%. The cardiopulmonary rehabilitation program had a positive impact on these cases, improving functional capacity despite the different severity levels in these post-COVID-19 cases.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):399-407
DOI 10.1590/S0103-507X2007000300023
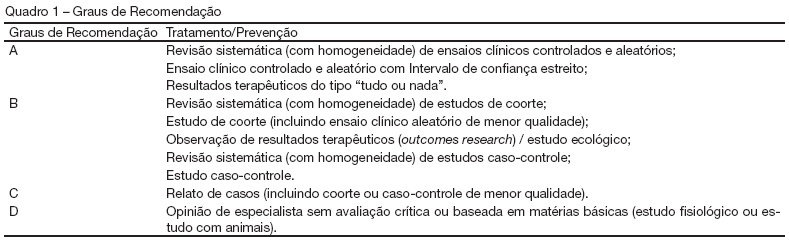
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Physical therapy during mechanical ventilation has been one of the updated topics. This objective was described the most important topics on the physical therapy during mechanical ventilation. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words: mechanical ventilation and physical therapy. RESULTS: Recommendations on the most important techniques applied during mechanical ventilation. CONCLUSIONS: Physical therapy has a central role at the Intensive Care environment, mainly in patients submitted to a mechanical ventilatory support invasive or non invasive.
Abstract
Rev Bras Ter Intensiva. 2007;19(3):399-407
DOI 10.1590/S0103-507X2007000300023
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Physical therapy during mechanical ventilation has been one of the updated topics. This objective was described the most important topics on the physical therapy during mechanical ventilation. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words: mechanical ventilation and physical therapy. RESULTS: Recommendations on the most important techniques applied during mechanical ventilation. CONCLUSIONS: Physical therapy has a central role at the Intensive Care environment, mainly in patients submitted to a mechanical ventilatory support invasive or non invasive.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):221-225
DOI 10.1590/S0103-507X2007000200014
BACKGROUND AND OBJECTIVES: Mechanically ventilated patients usually present larger amounts of pulmonary secretions because of impairment in mucociliary function and mucus transport. The manual resuscitator is considered a resource for pulmonary hyperinflation with the aim of preventing mucus retention and pulmonary complications, improving oxygenation and reexpanding collapsed areas. Alternatively, the hyperinflation by mechanical ventilator is a reliable and practical device to promote lung expansion and desobstruction. The objective of this study was to review the literature concerning manual and ventilator hyperinflation treatments for patients in the intensive care units (ICU) setting. CONTENTS: Literature searches were performed using the databases MedLine, CINAHL, SciElo and LILACS with appropriate keywords, including: intensive care units, manual hyperinflation, mechanical ventilator, physiotherapy, physical therapy and ventilator hyperinflation. CONCLUSIONS: Although there are few studies demonstrating the efficacy of ventilator hyperinflation as a physical therapy device, it can be a safety option to promote therapeutic hyperinflation in ICU, compared to manual hyperinflation.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):221-225
DOI 10.1590/S0103-507X2007000200014
BACKGROUND AND OBJECTIVES: Mechanically ventilated patients usually present larger amounts of pulmonary secretions because of impairment in mucociliary function and mucus transport. The manual resuscitator is considered a resource for pulmonary hyperinflation with the aim of preventing mucus retention and pulmonary complications, improving oxygenation and reexpanding collapsed areas. Alternatively, the hyperinflation by mechanical ventilator is a reliable and practical device to promote lung expansion and desobstruction. The objective of this study was to review the literature concerning manual and ventilator hyperinflation treatments for patients in the intensive care units (ICU) setting. CONTENTS: Literature searches were performed using the databases MedLine, CINAHL, SciElo and LILACS with appropriate keywords, including: intensive care units, manual hyperinflation, mechanical ventilator, physiotherapy, physical therapy and ventilator hyperinflation. CONCLUSIONS: Although there are few studies demonstrating the efficacy of ventilator hyperinflation as a physical therapy device, it can be a safety option to promote therapeutic hyperinflation in ICU, compared to manual hyperinflation.