Depression Archives - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(2):147-155
DOI 10.5935/2965-2774.20230422-pt
To assess factors associated with long-term neuropsychiatric outcomes, including biomarkers measured after discharge from the intensive care unit.
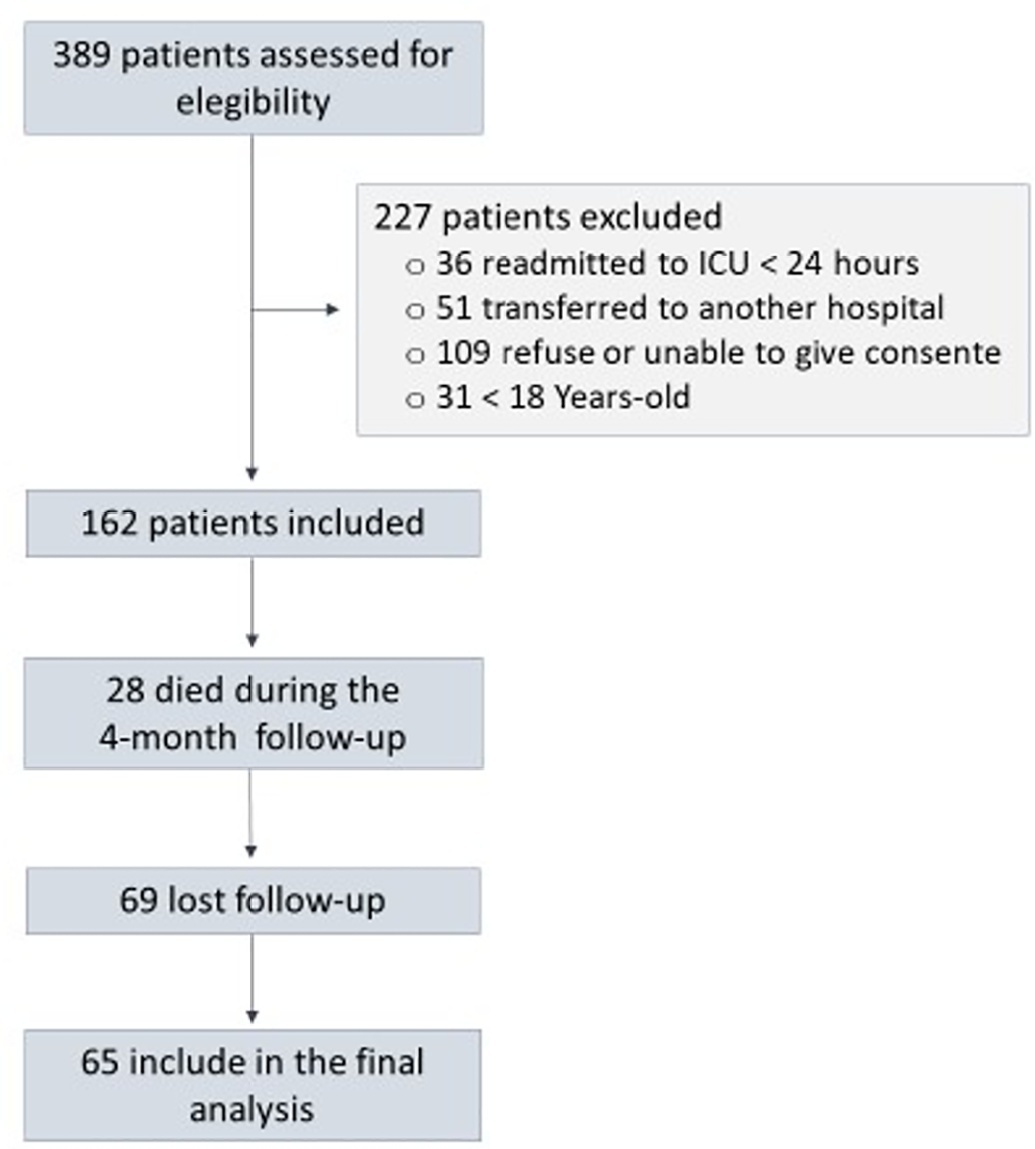
A prospective cohort study was performed with 65 intensive care unit survivors. The cognitive evaluation was performed through the Mini-Mental State Examination, the symptoms of anxiety and depression were evaluated using the Hospital Anxiety and Depression Scale, and posttraumatic stress disorder was evaluated using the Impact of Event Scale-6. Plasma levels of amyloid-beta (1-42) [Aβ (1-42)], Aβ (1-40), interleukin (IL)-10, IL-6, IL-33, IL-4, IL-5, tumor necrosis factor alpha, C-reactive protein, and brain-derived neurotrophic factor were measured at intensive care unit discharge.
Of the variables associated with intensive care, only delirium was independently related to the occurrence of long-term cognitive impairment. In addition, higher levels of IL-10 and IL-6 were associated with cognitive dysfunction. Only IL-6 was independently associated with depression. Mechanical ventilation, IL-33 levels, and C-reactive protein levels were independently associated with anxiety. No variables were independently associated with posttraumatic stress disorder.
Cognitive dysfunction, as well as symptoms of depression, anxiety, and posttraumatic stress disorder, are present in patients who survive a critical illness, and some of these outcomes are associated with the levels of inflammatory biomarkers measured at discharge from the intensive care unit.
Abstract
Crit Care Sci. 2023;35(2):147-155
DOI 10.5935/2965-2774.20230422-pt
To assess factors associated with long-term neuropsychiatric outcomes, including biomarkers measured after discharge from the intensive care unit.
A prospective cohort study was performed with 65 intensive care unit survivors. The cognitive evaluation was performed through the Mini-Mental State Examination, the symptoms of anxiety and depression were evaluated using the Hospital Anxiety and Depression Scale, and posttraumatic stress disorder was evaluated using the Impact of Event Scale-6. Plasma levels of amyloid-beta (1-42) [Aβ (1-42)], Aβ (1-40), interleukin (IL)-10, IL-6, IL-33, IL-4, IL-5, tumor necrosis factor alpha, C-reactive protein, and brain-derived neurotrophic factor were measured at intensive care unit discharge.
Of the variables associated with intensive care, only delirium was independently related to the occurrence of long-term cognitive impairment. In addition, higher levels of IL-10 and IL-6 were associated with cognitive dysfunction. Only IL-6 was independently associated with depression. Mechanical ventilation, IL-33 levels, and C-reactive protein levels were independently associated with anxiety. No variables were independently associated with posttraumatic stress disorder.
Cognitive dysfunction, as well as symptoms of depression, anxiety, and posttraumatic stress disorder, are present in patients who survive a critical illness, and some of these outcomes are associated with the levels of inflammatory biomarkers measured at discharge from the intensive care unit.
Abstract
Crit Care Sci. 2023;35(1):31-36
DOI 10.5935/2965-2774.20230113-pt
To evaluate the impact of an educational website on satisfaction and symptoms of anxiety and depression among family members of critically ill adult patients.
We embedded an analysis of website access in a cohort study conducted in intensive care units with flexible visiting hours in Brazil. Family members were guided to access an educational website designed to help them understand the processes and emotions associated with an intensive care unit stay. Subjects were evaluated for baseline data within the first 48 hours following enrollment and outcome assessment at up to 7 days after patient discharge from the intensive care unit, death, or until the 30th day of the study. The main outcomes were satisfaction using the Critical Care Family Needs Inventory and the presence of anxiety and depression symptoms using the Hospital Anxiety and Depression Scale.
A total of 532 family members were evaluated during the study period. Of these, 61 (11.5%) accessed the website. After adjustments, family members who accessed the website had significantly better mean Critical Care Family Needs Inventory scores (152.8 versus 145.2, p = 0.01) and a lower prevalence of probable clinical anxiety (prevalence ratio 0.35; 95%CI 0.14 - 0.89) than family members who did not access the website. There were no differences regarding symptoms of depression.
Access to an educational website was associated with higher family satisfaction with care and a lower prevalence of clinical anxiety.
Abstract
Crit Care Sci. 2023;35(1):31-36
DOI 10.5935/2965-2774.20230113-pt
To evaluate the impact of an educational website on satisfaction and symptoms of anxiety and depression among family members of critically ill adult patients.
We embedded an analysis of website access in a cohort study conducted in intensive care units with flexible visiting hours in Brazil. Family members were guided to access an educational website designed to help them understand the processes and emotions associated with an intensive care unit stay. Subjects were evaluated for baseline data within the first 48 hours following enrollment and outcome assessment at up to 7 days after patient discharge from the intensive care unit, death, or until the 30th day of the study. The main outcomes were satisfaction using the Critical Care Family Needs Inventory and the presence of anxiety and depression symptoms using the Hospital Anxiety and Depression Scale.
A total of 532 family members were evaluated during the study period. Of these, 61 (11.5%) accessed the website. After adjustments, family members who accessed the website had significantly better mean Critical Care Family Needs Inventory scores (152.8 versus 145.2, p = 0.01) and a lower prevalence of probable clinical anxiety (prevalence ratio 0.35; 95%CI 0.14 - 0.89) than family members who did not access the website. There were no differences regarding symptoms of depression.
Access to an educational website was associated with higher family satisfaction with care and a lower prevalence of clinical anxiety.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):499-506
DOI 10.5935/0103-507X.20220080-en
To evaluate the prevalence and factors associated with depression in family members of people hospitalized in intensive care units.
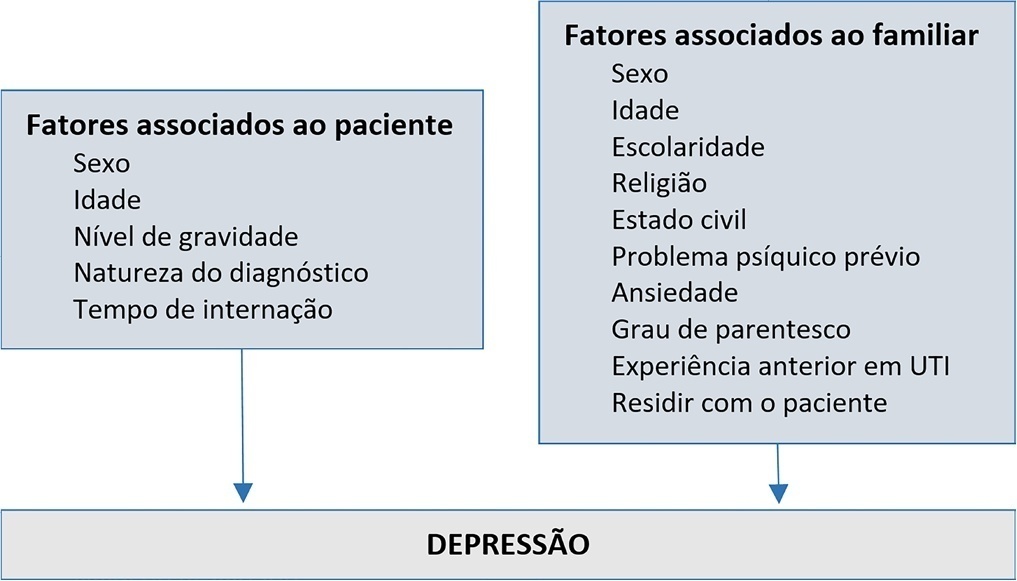
A cross-sectional study was conducted with 980 family members of patients admitted to the intensive care units of a large public hospital in the interior of Bahia. Depression was measured using the Patient Health Questionnaire-8. The multivariate model consisted of the following variables: sex and age of the patient, sex and age of the family member, education level, religion, living with the family member, previous mental illness and anxiety.
Depression had a prevalence of 43.5%. In the multivariate analysis, the model with the best representativeness indicated that factors associated with a higher prevalence of depression were being female (39%), age younger than 40 years (26%) and previous mental illness (38%). A higher education level was associated with a 19% lower prevalence of depression in family members.
The increase in the prevalence of depression was associated with female sex, age younger than 40 years and previous psychological problems. Such elements should be valued in actions aimed at family members of people hospitalized in intensive care.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):499-506
DOI 10.5935/0103-507X.20220080-en
To evaluate the prevalence and factors associated with depression in family members of people hospitalized in intensive care units.
A cross-sectional study was conducted with 980 family members of patients admitted to the intensive care units of a large public hospital in the interior of Bahia. Depression was measured using the Patient Health Questionnaire-8. The multivariate model consisted of the following variables: sex and age of the patient, sex and age of the family member, education level, religion, living with the family member, previous mental illness and anxiety.
Depression had a prevalence of 43.5%. In the multivariate analysis, the model with the best representativeness indicated that factors associated with a higher prevalence of depression were being female (39%), age younger than 40 years (26%) and previous mental illness (38%). A higher education level was associated with a 19% lower prevalence of depression in family members.
The increase in the prevalence of depression was associated with female sex, age younger than 40 years and previous psychological problems. Such elements should be valued in actions aimed at family members of people hospitalized in intensive care.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):458-467
DOI 10.5935/0103-507X.20200076
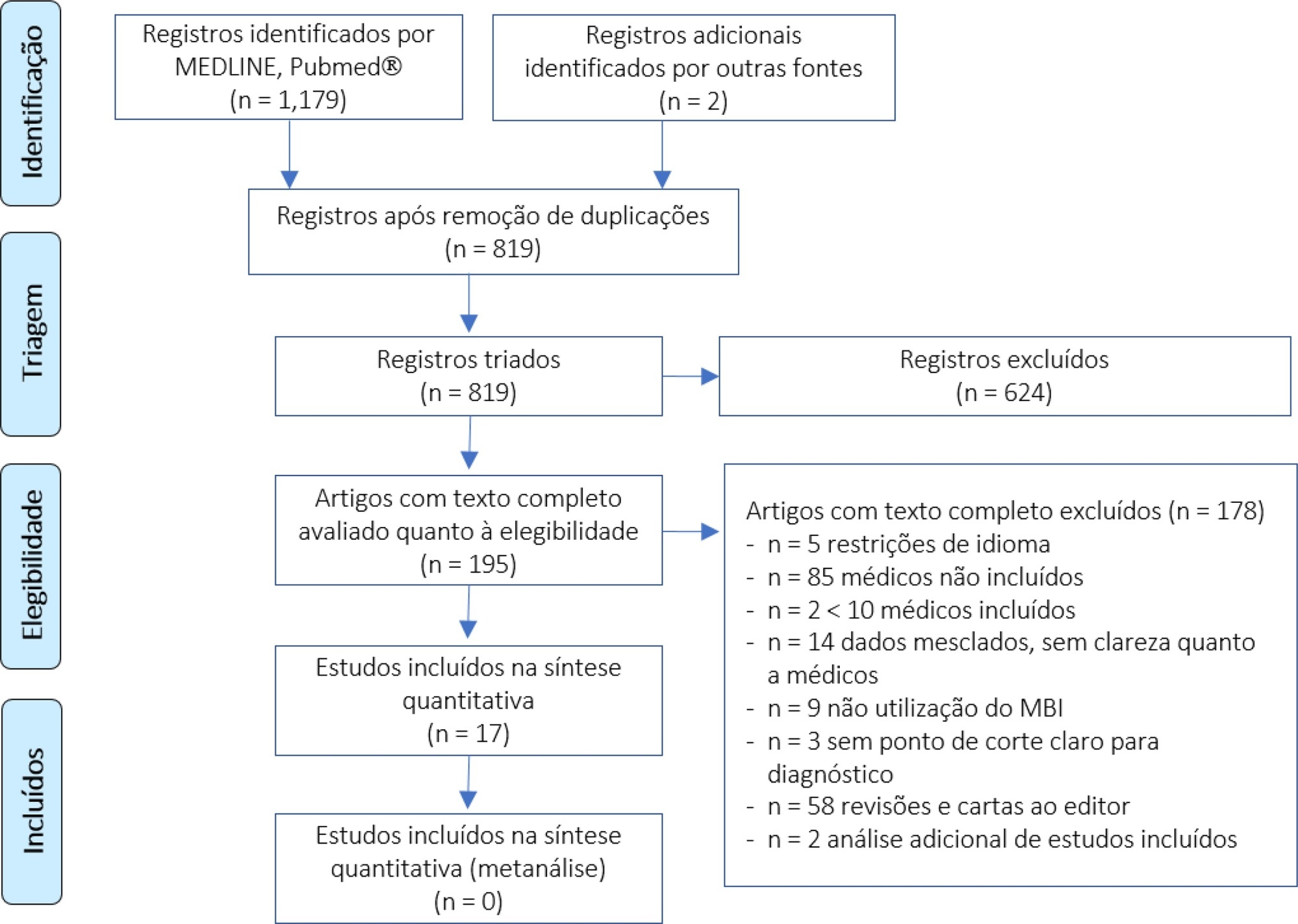
We performed a systematic review to summarize the knowledge regarding the prevalence of burnout among intensive care unit physicians.
We conducted a systematic review of the MEDLINE and PubMed® databases (last update 04.02.2019) with the goal of summarizing the evidence on burnout among intensive care unit physicians. We included all studies reporting burnout in intensive care unit personnel according to the Maslach Burnout Inventory questionnaire and then screened studies for data on burnout among intensive care unit physician specifically.
We found 31 studies describing burnout in intensive care unit staff and including different healthcare profiles. Among these, 5 studies focused on physicians only, and 12 others investigated burnout in mixed intensive care unit personnel but provided separate data on physicians. The prevalence of burnout varied greatly across studies (range 18% - 49%), but several methodological discrepancies, among them cut-off criteria for defining burnout and variability in the Likert scale, precluded a meaningful pooled analysis.
The prevalence of burnout syndrome among intensive care unit physicians is relatively high, but significant methodological heterogeneities warrant caution being used in interpreting our results. The lower reported levels of burnout seem higher than those found in studies investigating mixed intensive care unit personnel. There is an urgent need for consensus recommending a consistent use of the Maslach Burnout Inventory test to screen burnout, in order to provide precise figures on burnout in intensive care unit physicians.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):458-467
DOI 10.5935/0103-507X.20200076
We performed a systematic review to summarize the knowledge regarding the prevalence of burnout among intensive care unit physicians.
We conducted a systematic review of the MEDLINE and PubMed® databases (last update 04.02.2019) with the goal of summarizing the evidence on burnout among intensive care unit physicians. We included all studies reporting burnout in intensive care unit personnel according to the Maslach Burnout Inventory questionnaire and then screened studies for data on burnout among intensive care unit physician specifically.
We found 31 studies describing burnout in intensive care unit staff and including different healthcare profiles. Among these, 5 studies focused on physicians only, and 12 others investigated burnout in mixed intensive care unit personnel but provided separate data on physicians. The prevalence of burnout varied greatly across studies (range 18% - 49%), but several methodological discrepancies, among them cut-off criteria for defining burnout and variability in the Likert scale, precluded a meaningful pooled analysis.
The prevalence of burnout syndrome among intensive care unit physicians is relatively high, but significant methodological heterogeneities warrant caution being used in interpreting our results. The lower reported levels of burnout seem higher than those found in studies investigating mixed intensive care unit personnel. There is an urgent need for consensus recommending a consistent use of the Maslach Burnout Inventory test to screen burnout, in order to provide precise figures on burnout in intensive care unit physicians.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):381-390
DOI 10.5935/0103-507X.20200066
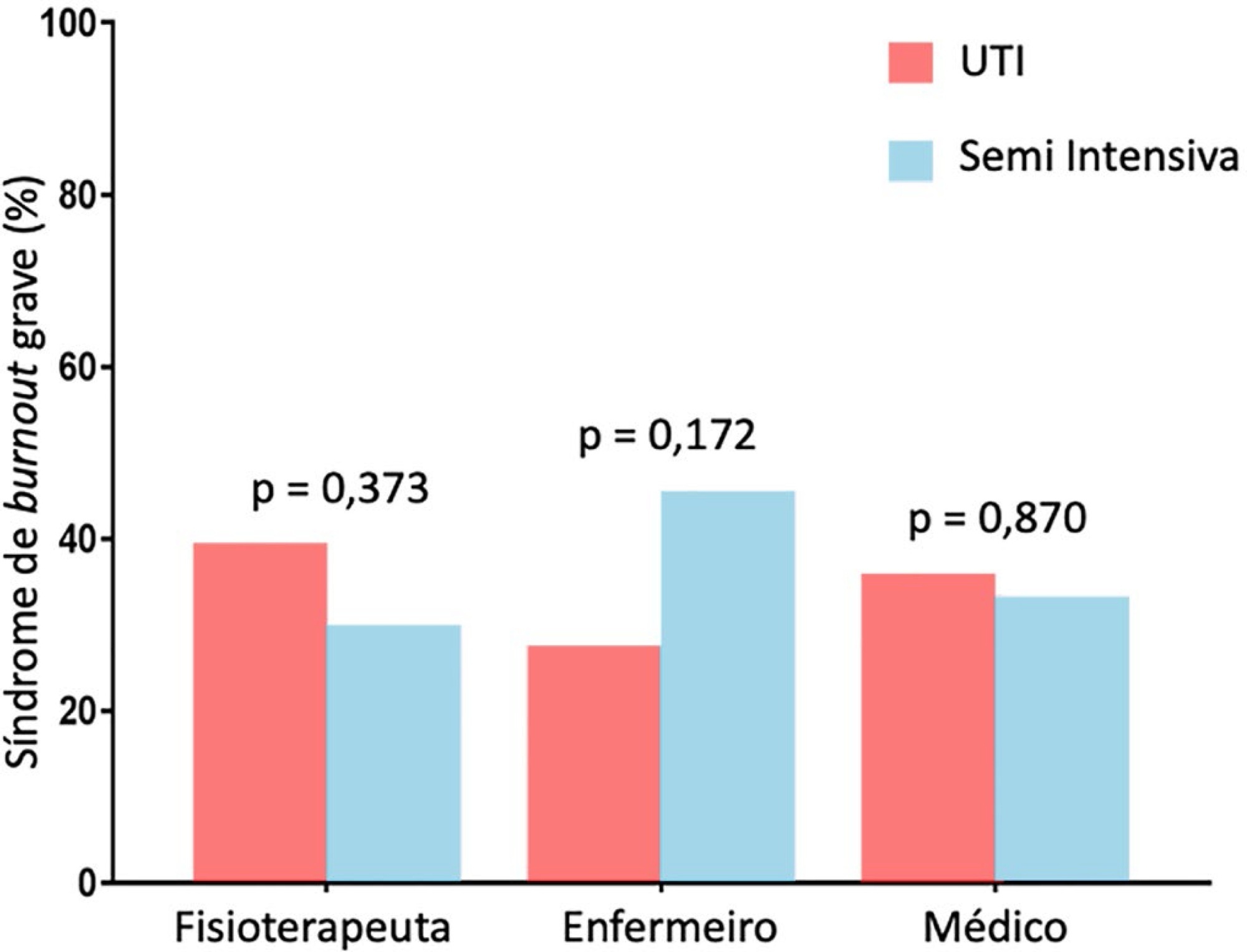
To evaluate the frequency of severe burnout syndrome among critical care providers and to correlate it with work engagement.
A self-administered survey including the Maslach Burnout Inventory, Depression Anxiety and Stress Scales, and Gallup questionnaire was distributed. All analyses were stratified by setting (intensive care unit or step-down unit) and by professional group (nurses versus physicians versus physiotherapists).
Between February 2017 and June 2017, 206 out of 325 invited professionals (63.4%) answered the questionnaires. Of these, 55 were physicians (26.7%), 88 were physiotherapists (42.7%) and 63 were nurses (30.6%). The frequency of severe burnout was 34.3% (27.9 - 41.4%), and no difference was found between professional groups or settings. The frequency of severe or very severe cases of depression, anxiety or stress was 12.9%, 11.4% and 10.5%, respectively. The median (interquartile range) score observed on the Gallup questionnaire was 41 (34 - 48), and no differences were found between professional groups or settings. There was a negative correlation between burnout and work engagement (r = -0.148; p = 0.035).
There is a high frequency of severe burnout among critical care providers working in the intensive care unit and step-down unit. There was a negative correlation between burnout and work engagement.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):381-390
DOI 10.5935/0103-507X.20200066
To evaluate the frequency of severe burnout syndrome among critical care providers and to correlate it with work engagement.
A self-administered survey including the Maslach Burnout Inventory, Depression Anxiety and Stress Scales, and Gallup questionnaire was distributed. All analyses were stratified by setting (intensive care unit or step-down unit) and by professional group (nurses versus physicians versus physiotherapists).
Between February 2017 and June 2017, 206 out of 325 invited professionals (63.4%) answered the questionnaires. Of these, 55 were physicians (26.7%), 88 were physiotherapists (42.7%) and 63 were nurses (30.6%). The frequency of severe burnout was 34.3% (27.9 - 41.4%), and no difference was found between professional groups or settings. The frequency of severe or very severe cases of depression, anxiety or stress was 12.9%, 11.4% and 10.5%, respectively. The median (interquartile range) score observed on the Gallup questionnaire was 41 (34 - 48), and no differences were found between professional groups or settings. There was a negative correlation between burnout and work engagement (r = -0.148; p = 0.035).
There is a high frequency of severe burnout among critical care providers working in the intensive care unit and step-down unit. There was a negative correlation between burnout and work engagement.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):147-155
DOI 10.5935/0103-507X.20190024
To analyze the satisfaction, medical situation understanding and symptoms of anxiety and depression in family members of patients admitted to the intensive care unit.
The family members of patients who were hospitalized for ≥ 72 hours were invited to participate in the study, which was performed in a public hospital. Questionnaires were answered to assess the understanding of the diagnosis, treatment and prognosis, and the support received in the intensive care unit. The family needs were also evaluated using a modified version of the Critical Care Family Needs Inventory (CCFNI). The Hospital Anxiety and Depression Scale (HADS) was used to assess the symptoms of anxiety and depression.
A total of 35 family members were interviewed within the patients' first week of stay in the intensive care unit. Most patients (57.1%) were male, aged 54 ± 19 years. Sepsis was the main reason for admission to the intensive care unit (40%); the median of the Simplified Acute Physiology Score (SAPS) 3 was 68 (48 - 77), and 51.4% of the patients died in the intensive care unit. The majority of the family members were female (74.3%) and were sons or daughters of patients (54.3%), with a mean age of 43.2 ± 14 years. Overall, 77.1% of the family members were satisfied with the intensive care unit. A total of 37.1% of the family members did not understand the prognosis. Receiving clear and complete information in the intensive care unit and the doctor being accessible were factors that were significantly correlated with the overall family satisfaction. The prevalence of symptoms of anxiety (60%) and depression (54.3%) in the family members was high.
The emotional distress of family members is high during a patient's hospitalization in the intensive care unit, although satisfaction is also high. Clear and complete information provided by the intensivist and the support received in the intensive care unit are significantly correlated with the satisfaction of family members in a public hospital.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):147-155
DOI 10.5935/0103-507X.20190024
To analyze the satisfaction, medical situation understanding and symptoms of anxiety and depression in family members of patients admitted to the intensive care unit.
The family members of patients who were hospitalized for ≥ 72 hours were invited to participate in the study, which was performed in a public hospital. Questionnaires were answered to assess the understanding of the diagnosis, treatment and prognosis, and the support received in the intensive care unit. The family needs were also evaluated using a modified version of the Critical Care Family Needs Inventory (CCFNI). The Hospital Anxiety and Depression Scale (HADS) was used to assess the symptoms of anxiety and depression.
A total of 35 family members were interviewed within the patients' first week of stay in the intensive care unit. Most patients (57.1%) were male, aged 54 ± 19 years. Sepsis was the main reason for admission to the intensive care unit (40%); the median of the Simplified Acute Physiology Score (SAPS) 3 was 68 (48 - 77), and 51.4% of the patients died in the intensive care unit. The majority of the family members were female (74.3%) and were sons or daughters of patients (54.3%), with a mean age of 43.2 ± 14 years. Overall, 77.1% of the family members were satisfied with the intensive care unit. A total of 37.1% of the family members did not understand the prognosis. Receiving clear and complete information in the intensive care unit and the doctor being accessible were factors that were significantly correlated with the overall family satisfaction. The prevalence of symptoms of anxiety (60%) and depression (54.3%) in the family members was high.
The emotional distress of family members is high during a patient's hospitalization in the intensive care unit, although satisfaction is also high. Clear and complete information provided by the intensivist and the support received in the intensive care unit are significantly correlated with the satisfaction of family members in a public hospital.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):405-413
DOI 10.5935/0103-507X.20180063
To establish the prevalence of physical, cognitive and psychiatric disabilities, associated factors and their relationship with the qualities of life of intensive care survivors in Brazil.
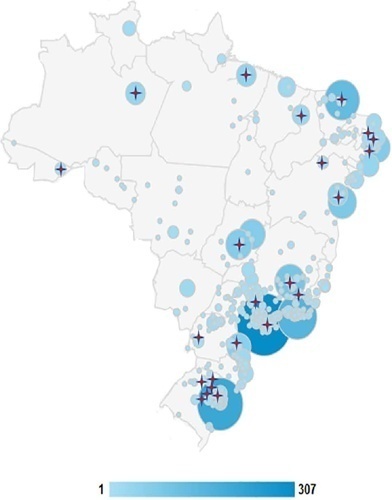
A prospective multicenter cohort study is currently being conducted at 10 adult medical-surgical intensive care units representative of the 5 Brazilian geopolitical regions. Patients aged ≥ 18 years who are discharged from the participating intensive care units and stay 72 hours or more in the intensive care unit for medical or emergency surgery admissions or 120 hours or more for elective surgery admissions are consecutively included. Patients are followed up for a period of one year by means of structured telephone interviews conducted at 3, 6 and 12 months after discharge from the intensive care unit. The outcomes are functional dependence, cognitive dysfunction, anxiety and depression symptoms, posttraumatic stress symptoms, health-related quality of life, rehospitalization and long-term mortality.
The present study has the potential to contribute to current knowledge of the prevalence and factors associated with postintensive care syndrome among adult intensive care survivors in Brazil. In addition, an association might be established between postintensive care syndrome and health-related quality of life.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):405-413
DOI 10.5935/0103-507X.20180063
To establish the prevalence of physical, cognitive and psychiatric disabilities, associated factors and their relationship with the qualities of life of intensive care survivors in Brazil.
A prospective multicenter cohort study is currently being conducted at 10 adult medical-surgical intensive care units representative of the 5 Brazilian geopolitical regions. Patients aged ≥ 18 years who are discharged from the participating intensive care units and stay 72 hours or more in the intensive care unit for medical or emergency surgery admissions or 120 hours or more for elective surgery admissions are consecutively included. Patients are followed up for a period of one year by means of structured telephone interviews conducted at 3, 6 and 12 months after discharge from the intensive care unit. The outcomes are functional dependence, cognitive dysfunction, anxiety and depression symptoms, posttraumatic stress symptoms, health-related quality of life, rehospitalization and long-term mortality.
The present study has the potential to contribute to current knowledge of the prevalence and factors associated with postintensive care syndrome among adult intensive care survivors in Brazil. In addition, an association might be established between postintensive care syndrome and health-related quality of life.

Abstract
Rev Bras Ter Intensiva. 2018;30(1):35-41
DOI 10.5935/0103-507X.20180004
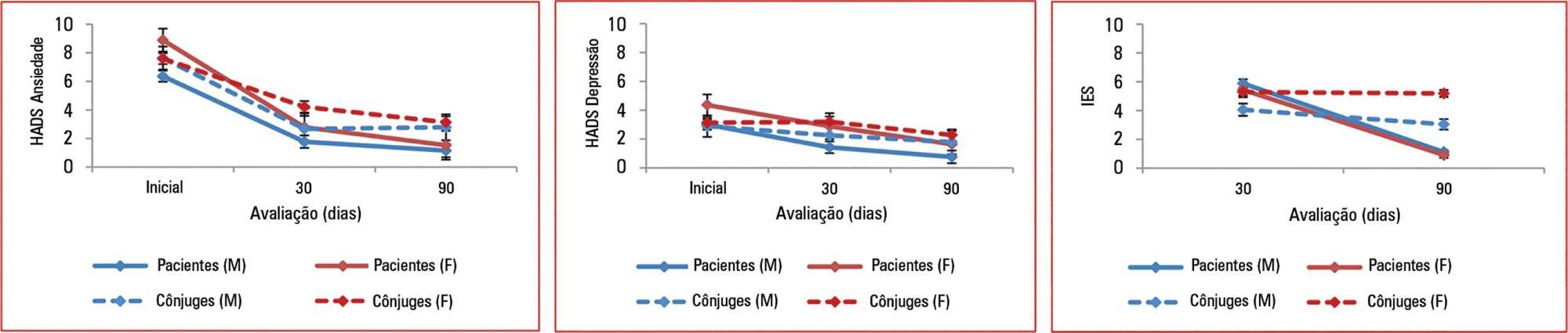
To assess the effect of sex and spouse condition on symptoms of anxiety, depression and posttraumatic stress symptoms in patients and their spouses.
A prospective study conducted in a 22-bed adult mixed intensive care unit in a tertiary hospital in São Paulo, Brazil. Patients and their spouses were enrolled 2 days after intensive care unit admission. They were interviewed while in the intensive care unit using the Hospital Anxiety and Depression Scale. At 30 and 90 days after intensive care unit discharge, they completed the Impact of Event Scale and Hospital Anxiety and Depression Scale by phone.
From March 2011 to March 2013, we analyzed 118 patients and their spouses. We observed that female sex was associated with higher scores than male sex was in terms of the anxiety Hospital Anxiety and Depression Scale - subscale (p = 0.032) and depression (p = 0.034). There was no association between sex and posttraumatic stress disorder symptoms. However, spouses had higher Impact of Event Scale points compared with patients (p = 0.001).
Female sex was associated with anxiety and depression, and spouses were more vulnerable to post-traumatic stress symptoms than the patients were. Increasing age and a later time of assessment were also associated with lower scores on the Impact of Event Scale.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):35-41
DOI 10.5935/0103-507X.20180004
To assess the effect of sex and spouse condition on symptoms of anxiety, depression and posttraumatic stress symptoms in patients and their spouses.
A prospective study conducted in a 22-bed adult mixed intensive care unit in a tertiary hospital in São Paulo, Brazil. Patients and their spouses were enrolled 2 days after intensive care unit admission. They were interviewed while in the intensive care unit using the Hospital Anxiety and Depression Scale. At 30 and 90 days after intensive care unit discharge, they completed the Impact of Event Scale and Hospital Anxiety and Depression Scale by phone.
From March 2011 to March 2013, we analyzed 118 patients and their spouses. We observed that female sex was associated with higher scores than male sex was in terms of the anxiety Hospital Anxiety and Depression Scale - subscale (p = 0.032) and depression (p = 0.034). There was no association between sex and posttraumatic stress disorder symptoms. However, spouses had higher Impact of Event Scale points compared with patients (p = 0.001).
Female sex was associated with anxiety and depression, and spouses were more vulnerable to post-traumatic stress symptoms than the patients were. Increasing age and a later time of assessment were also associated with lower scores on the Impact of Event Scale.