Consensus Archives - Critical Care Science (CCS)

Abstract
Critical Care Science. 2023;35(1):2-10
DOI 10.5935/2965-2774.20230307-en
The use of echocardiography by physicians who are not echocardiographers has become common throughout the world across highly diverse settings where the care of acutely ill patients is provided. Echocardiographic evaluation performed in a point-of-care manner can provide relevant information regarding the mechanism of causes of shock, for example, increasing the rates of correct diagnosis and allowing for faster informed decision-making than through evaluation methods. Considering that the accurate diagnosis of life-threatening situations is essential for professionals working with acutely ill patients, several international associations recommend that physicians responsible for critically ill patients acquire and develop the ability to perform bedside ultrasound examinations, including echocardiographic examinations. However, there is no consensus in the literature regarding which specific applications should be included in the list of skills for nonechocardiographer physicians. Taking into account the multiplicity of applications of echocardiography in different scenarios related to acutely ill patients; the differences in the published protocols, with regard to both the teaching methodology and competence verification; and the heterogeneity of training among highly diverse specialties responsible for their care at different levels, this consensus document aimed to reflect the position of representatives of related Brazilian medical societies on the subject and may thus serve as a starting point both for standardization among different specialties and for the transmission of knowledge and verification of the corresponding competencies.
Abstract
Critical Care Science. 2023;35(1):2-10
DOI 10.5935/2965-2774.20230307-en
The use of echocardiography by physicians who are not echocardiographers has become common throughout the world across highly diverse settings where the care of acutely ill patients is provided. Echocardiographic evaluation performed in a point-of-care manner can provide relevant information regarding the mechanism of causes of shock, for example, increasing the rates of correct diagnosis and allowing for faster informed decision-making than through evaluation methods. Considering that the accurate diagnosis of life-threatening situations is essential for professionals working with acutely ill patients, several international associations recommend that physicians responsible for critically ill patients acquire and develop the ability to perform bedside ultrasound examinations, including echocardiographic examinations. However, there is no consensus in the literature regarding which specific applications should be included in the list of skills for nonechocardiographer physicians. Taking into account the multiplicity of applications of echocardiography in different scenarios related to acutely ill patients; the differences in the published protocols, with regard to both the teaching methodology and competence verification; and the heterogeneity of training among highly diverse specialties responsible for their care at different levels, this consensus document aimed to reflect the position of representatives of related Brazilian medical societies on the subject and may thus serve as a starting point both for standardization among different specialties and for the transmission of knowledge and verification of the corresponding competencies.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(1):78-85
DOI 10.1590/S0103-507X2006000100013
BACKGROUND AND OBJECTIVES: Cardiac output and preload as absolute data do not offer helpful information about the hemodynamic of critically ill patients. However, monitoring the response of these variables to volume challenge or inotropic drugs is a very useful tool in the critical care setting, particularly for patients with signs of tissue hypoperfusion. Although PAC remains the " gold standard" to measure cardiac output and preload, new and alternative technologies were developed to evaluate these hemodynamic variables. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty three physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations regarding the use of arterial pulse pressure variation during mechanical ventilation, continuous arterial pulse contour and lithium dilution cardiac output measurements, esophageal Doppler waveform, thoracic electrical bioimpedance, echocardiography and partial CO2 rebreathing for monitoring cardiac output and preload were created. CONCLUSIONS: The new and less invasive techniques for the measurement of cardiac output, preload or fluid responsiveness are accurate and may be an alternative to PAC in critically ill patients.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(1):78-85
DOI 10.1590/S0103-507X2006000100013
BACKGROUND AND OBJECTIVES: Cardiac output and preload as absolute data do not offer helpful information about the hemodynamic of critically ill patients. However, monitoring the response of these variables to volume challenge or inotropic drugs is a very useful tool in the critical care setting, particularly for patients with signs of tissue hypoperfusion. Although PAC remains the " gold standard" to measure cardiac output and preload, new and alternative technologies were developed to evaluate these hemodynamic variables. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty three physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations regarding the use of arterial pulse pressure variation during mechanical ventilation, continuous arterial pulse contour and lithium dilution cardiac output measurements, esophageal Doppler waveform, thoracic electrical bioimpedance, echocardiography and partial CO2 rebreathing for monitoring cardiac output and preload were created. CONCLUSIONS: The new and less invasive techniques for the measurement of cardiac output, preload or fluid responsiveness are accurate and may be an alternative to PAC in critically ill patients.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
BACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
BACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(2):161-176
DOI 10.1590/S0103-507X2006000200010
BACKGROUND AND OBJECTIVES: Shock occurs when the circulatory system cannot maintain adequate cellular perfusion. If this condition is not reverted irreversible cellular injury establishes. Shock treatment has as its initial priority the fast and vigorous correction of mean arterial pressure and cardiac output to maintain life and avoid or lessen organic dysfunctions. Fluid challenge and vasoactive drugs are necessary to warrant an adequate tissue perfusion and maintenance of function of different organs and systems, always guided by cardiovascular monitorization. The recommendations built in this consensus are aimed to guide hemodynamic support needed to maintain adequate tisular perfusion. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty five physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made answering 17 questions about hemodynamic support with focus on fluid challenge, red blood cell transfusions, vasoactive drugs and perioperative hemodynamic optimization. CONCLUSIONS: Hemodynamic monitoring by itself does not reduce the mortality of critically ill patients, however, we believe that the correct interpretation of the data obtained by the hemodynamic monitoring and the use of hemodynamic support protocols based on well defined tissue perfusion goals can improve the outcome of these patients.
Abstract
Revista Brasileira de Terapia Intensiva. 2006;18(2):161-176
DOI 10.1590/S0103-507X2006000200010
BACKGROUND AND OBJECTIVES: Shock occurs when the circulatory system cannot maintain adequate cellular perfusion. If this condition is not reverted irreversible cellular injury establishes. Shock treatment has as its initial priority the fast and vigorous correction of mean arterial pressure and cardiac output to maintain life and avoid or lessen organic dysfunctions. Fluid challenge and vasoactive drugs are necessary to warrant an adequate tissue perfusion and maintenance of function of different organs and systems, always guided by cardiovascular monitorization. The recommendations built in this consensus are aimed to guide hemodynamic support needed to maintain adequate tisular perfusion. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty five physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made answering 17 questions about hemodynamic support with focus on fluid challenge, red blood cell transfusions, vasoactive drugs and perioperative hemodynamic optimization. CONCLUSIONS: Hemodynamic monitoring by itself does not reduce the mortality of critically ill patients, however, we believe that the correct interpretation of the data obtained by the hemodynamic monitoring and the use of hemodynamic support protocols based on well defined tissue perfusion goals can improve the outcome of these patients.
Abstract
Revista Brasileira de Terapia Intensiva. 2007;19(2):264-272
DOI 10.1590/S0103-507X2007000200021
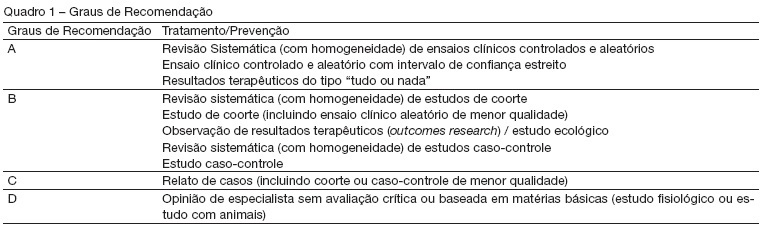
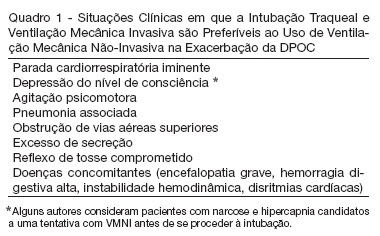
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Mechanical ventilation in COPD exacerbation has been one of the updated topics. Describe the most important topics on the mechanical ventilation during the COPD exacerbation and suggest the main therapeutic approaches. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the keywords "mechanical ventilation" and "COPD". RESULTS: We present recommendations on the ventilatory modes and settings to be adopted when ventilating a patient during an asthma attack, as well as the recommended monitoring. Alternative ventilation techniques are also presented. CONCLUSIONS: Protective ventilatory strategies are recommended when ventilating a patient during a.
Abstract
Revista Brasileira de Terapia Intensiva. 2007;19(2):264-272
DOI 10.1590/S0103-507X2007000200021
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Mechanical ventilation in COPD exacerbation has been one of the updated topics. Describe the most important topics on the mechanical ventilation during the COPD exacerbation and suggest the main therapeutic approaches. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the keywords "mechanical ventilation" and "COPD". RESULTS: We present recommendations on the ventilatory modes and settings to be adopted when ventilating a patient during an asthma attack, as well as the recommended monitoring. Alternative ventilation techniques are also presented. CONCLUSIONS: Protective ventilatory strategies are recommended when ventilating a patient during a.
Abstract
Revista Brasileira de Terapia Intensiva. 2007;19(2):258-263
DOI 10.1590/S0103-507X2007000200020
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Mechanical ventilation in the asthma attack has been one of the updated topics. Describe the most important topics on the mechanical ventilation during the asthma attack and suggest the main therapeutic approaches. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words "mechanical ventilation" and "asthma". RESULTS: We present recommendations on the ventilatory modes and settings to be adopted when ventilating a patient during an asthma attack, as well as the recommended monitoring. Alternative ventilation techniques are also presented. CONCLUSIONS: Protective ventilatory strategies are recommended when ventilating a patient during a severe asthma attack.
Abstract
Revista Brasileira de Terapia Intensiva. 2007;19(2):258-263
DOI 10.1590/S0103-507X2007000200020
BACKGROUND AND OBJECTIVES: The II Brazilian Consensus Conference on Mechanical Ventilation was published in 2000. Knowledge on the field of mechanical ventilation evolved rapidly since then, with the publication of numerous clinical studies with potential impact on the ventilatory management of critically ill patients. Moreover, the evolving concept of evidence - based medicine determined the grading of clinical recommendations according to the methodological value of the studies on which they are based. This explicit approach has broadened the understanding and adoption of clinical recommendations. For these reasons, AMIB - Associação de Medicina Intensiva Brasileira and SBPT - Sociedade Brasileira de Pneumologia e Tisiologia - decided to update the recommendations of the II Brazilian Consensus. Mechanical ventilation in the asthma attack has been one of the updated topics. Describe the most important topics on the mechanical ventilation during the asthma attack and suggest the main therapeutic approaches. METHODS: Systematic review of the published literature and gradation of the studies in levels of evidence, using the key words "mechanical ventilation" and "asthma". RESULTS: We present recommendations on the ventilatory modes and settings to be adopted when ventilating a patient during an asthma attack, as well as the recommended monitoring. Alternative ventilation techniques are also presented. CONCLUSIONS: Protective ventilatory strategies are recommended when ventilating a patient during a severe asthma attack.